
Abstract
Background:
Sleep restores physiology and neurochemical components of our body and is essential for physical and mental health. Sleep disorders (SDs) are associated with insulin resistance and metabolic disorders. The association between SDs and diabetes needs to be understood in the Indian population.
Purpose:
The purpose was to investigate the association between SD and diabetes in the Indian population.
Methods:
As a part of nationwide Niyantrita Madhumeha Bharata Abhiyaan-2017 (NMB-2017), a cross-sectional study was conducted and data was collected from seven zones of India, after screening through the Indian Diabetes Risk Score (IDRS). The sleep quality was assessed on a scale of 1 to 4 (very good = 1, very bad = 4). The time taken to fall asleep (sleep latency) was assessed on a scale of 0 to 5 (“0” = nil and “5” = >1.5 h). Stress was assessed by the perceived stress scale.
Results:
Bad sleep quality was positively (odds ratio 1.055, CI [1.001, 1.113], and P < .01) associated with self-reported known diabetes. Increased time taken to fall in sleep (sleep latency) was associated significantly with IDRS high risk (odds ratio 1.085, CI [1.008, 1.168], and P = .01), with an average sleep latency /time takes to fall in sleep (maximum range 5 [>1.5 h], mode 2 [10 to 30 min]) minutes. Moderate stress was significantly associated with bad sleep quality (odds ratio 1.659).
Conclusion:
A positive association of bad sleep quality and stress with diabetes, and an increased sleep latency in the IDRS high-risk population point to the role of modifiable risk factors. Behavioral modification and stress reduction by using yoga may be beneficial in the better management of diabetes.
Introduction
Sleep is a biological process involving both physiological and neurochemical aspects of life.1, 2 Circadian rhythm and sleep homeostasis influence each other and regulate the sleep–wake cycle. 3 Sleep can be considered as a health indicator. 4 The quality of sleep decides the physical and mental wellbeing of an individual, 3 especially slow-wave sleep or deep sleep has been demonstrated to be practically identified with optimal recovery and neuroplasticity.5 – 6 Seven to eight hours of night sleep is medically considered to be good enough to refresh the body.
Sleep promotes and performs important restorative functions for body homeostasis. 2 Sleep deprivation or inadequate sleep is directly associated with sleep disorders (SDs) and other health issues, such as mood disturbance, 7 impaired memory, 8 metabolic disorders like diabetes, obesity, 9 and hypertension. 10 It is estimated that approximately 20% to 30% of the general population has one or the other type of SD. 11
It has been seen that common health conditions such as diabetes, cardiovascular, neurological, urinary, or respiratory disorders are some of the major SD-associated comorbidities. 12 Low quality of sleep has been reported in 38.4% of diabetes patients. Homeostasis model assessment of insulin resistance showed a strong association of obstructive sleep apnea (OSA) with high insulin resistance, excessive body weight or obesity, and hypertension. 13 Another study showed a lack of sleep or fragmented sleep leads to insulin resistance, gain in body weight, type 2 diabetes,14, 15 and hypertension.16, 17 The duration of sleep also plays a major role as a diabetes risk factor. Tan et al. 18 in their review on the effect of sleep duration on diabetes individuals showed that both short-duration sleep (≤5 and 6 h/night) and long-duration sleep (>8 h/night) are detrimental to diabetes individuals.19, 20
India, the second-most populous country, reports around seven million new diabetes patients every year, and SDs are common amongst these patients. 21 Previous studies show that type 2 diabetes mellitus (DM) patients have a higher prevalence of insomnia, increased daytime sleep, and increased rapid eye movement sleep timing. OSA and DM are common amongst the aged and obese individuals. Both OSA and DM are associated with a higher risk of developing cardiovascular complications, resulting in increased morbidity and mortality. 22 Earlier studies on short sleep or disturbed sleep suggest impaired glucose tolerance in healthy individuals. 22 However, an association between SDs and diabetes is poorly understood in the Indian population. Hence, our study explored the prevalence of SDs in individuals with a high risk for diabetes, based on Indian Diabetes Risk Score (IDRS) which is a validated simple screening tool used to detect undiagnosed individuals with DM or those at a higher risk of developing DM. 23
Trial Profile
Methods
Study Design
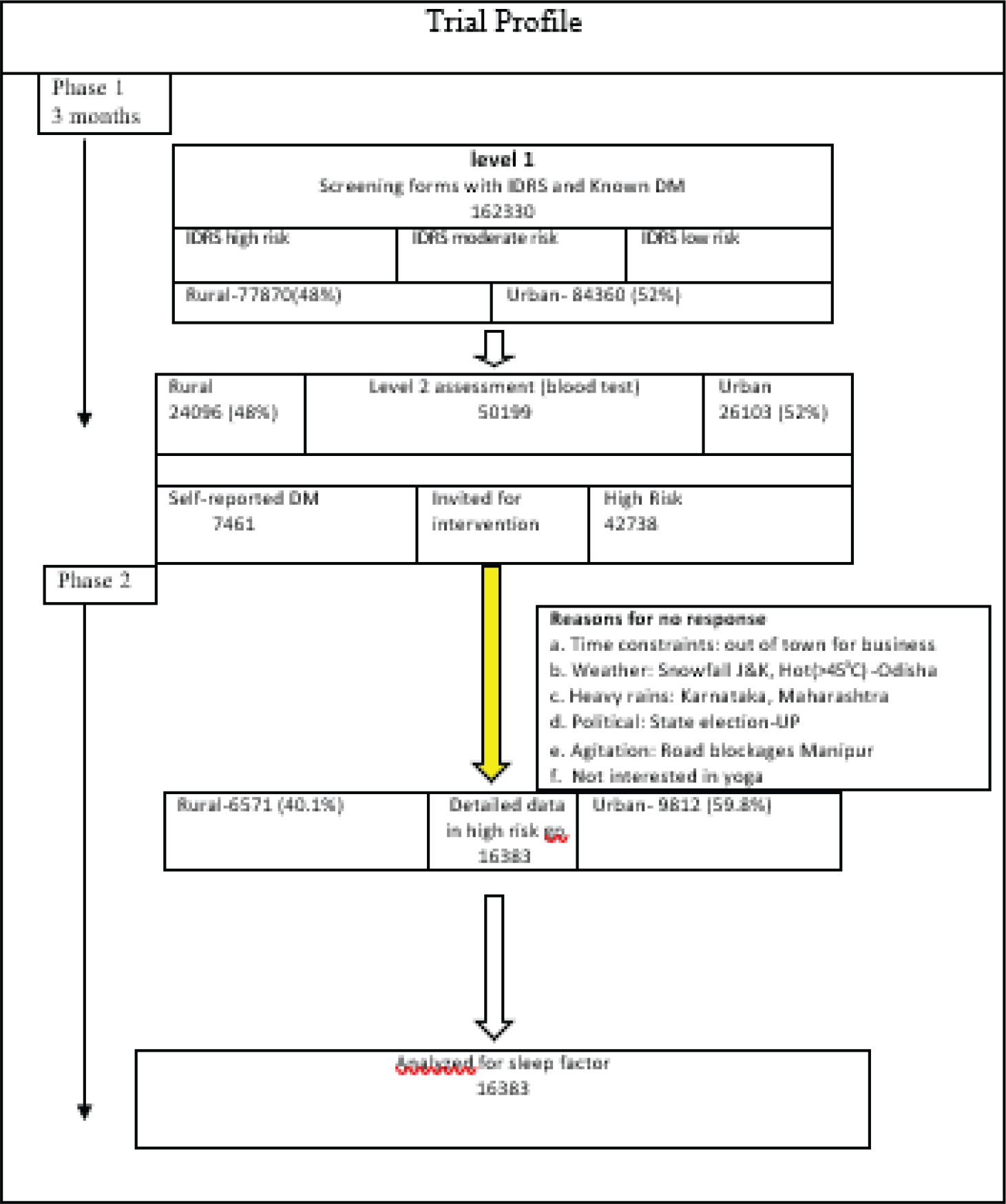
As a part of nationwide trial, the data was collected from seven zones of India (east, west, central, north, northeast, northwest, and south) in 2017 (the details have been published in methodology of our part 1 paper). 24 In short, the sampling process was divided into seven levels. With the help of 1,200 volunteers for diabetes movements, 35 senior research fellows, 2 research associates, and 7 zonal coordinators, this cross-sectional survey was completed. IDRS was used to identify high-risk individuals. Detail’s methodology is given in (Figure 1).
Participants
A total of 1,62,330 subjects [rural, 77,870 (48%); urban, 84,360 (52%)] were screened. Of these, 50,199 subjects [rural, 24,096 (48%); urban, 26,103 (52%); IDRS high risk, 42,738; self-reported DM, 7,461] with IDRS high risk and self-reported DM were selected for detailed investigations. Data for a sleep factor analysis was acquired from 16,383 subjects [rural, 6,571 (40.1%); urban, 9,812 (59.8%)].
Outcome Measures
An initial survey was done to screen the participants by the IDRS to identify high-risk individuals. IDRS consists of four parameters: age, family history, physical activity, and waist circumference. A score of 0 to 30 is considered as low risk, 30 to 50 moderate risk, and ≥60 as high risk.
Of these, the two most important questions were taken for the present sleep analysis.
(a) Sleep quality: During the past month, how would you rate your sleep quality overall? (Score 1, very good; 2, fairly good; 3, fairly bad; and 4, very bad.)
(b) How long has it taken you to fall asleep each night? (None 0; at least 10 min, 1; 10 to 30 min, 2; 30 min to 1 h, 3; 1 to 1.5 h, 4; and >1.5 h, 5.)
Statistical Analysis
Data was uploaded via Mobile Apps by trained field personnel under the supervision of senior research fellows. The data set was analyzed using the SPSS software for biostatistical analyses.
To calculate the odds ratio, ordinal regression was implemented; reference was set to sequential contrast for all ordinal variables. For known diabetes and known hypertension, unknown diabetes and unknown hypertension were the references, respectively. For IDRS high risk, IDRS low risk was the reference category. For obesity, normal was the reference. Regression was done to analyze the association of overall stress with overall sleep quality and that of overall depression with sleep quality.
Ethical clearance was obtained from the ethical committee of Indian Yoga Association.
Results
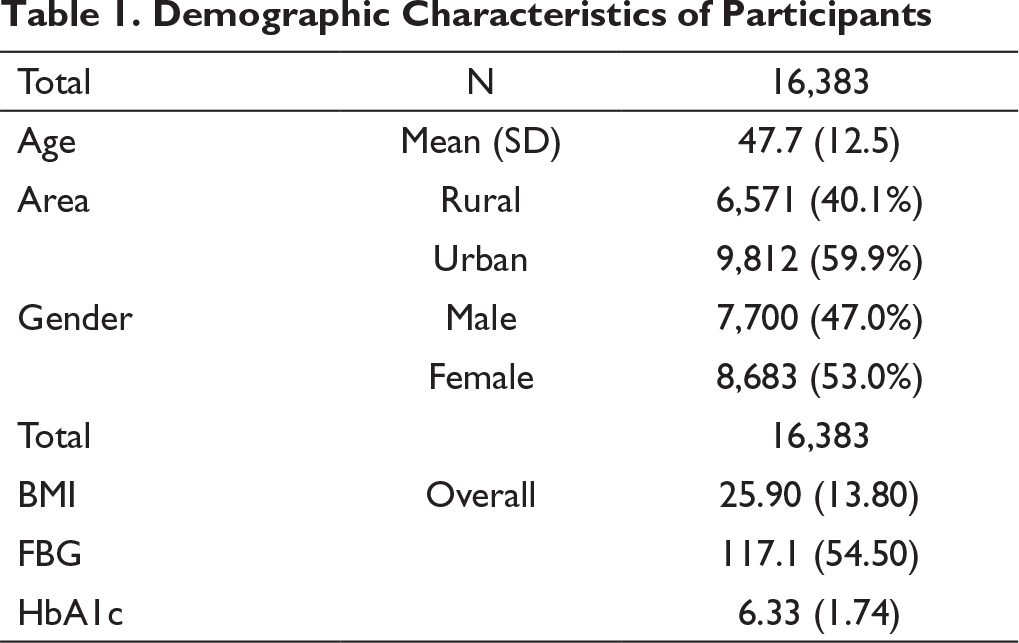
Table 1 represents the demographic details of 16,383 participants; the mean age of the participants was 48 years. The distribution of participants with respect to their location was as follows: urban cluster constituted 60%, and rural 40%, females constituted 53% of the study population, while males constituted 47%. The average body mass index (BMI) of the participants was 25.90, which suggest that the participants fall under the overweight category based on BMI estimates. Overall fasting blood glucose (FBG) was 117.1 mg/dL and glycated hemoglobin (HbA1c) was 6.33%.
Table 2 represents the sleep quality and sleep latency in different groups; 1.055 (1.001–1.113) is significantly associated with the status of known diabetes. Increased sleep time/sleep latency is associated significantly with IDRS high risk, with an odds ratio of 1.085 (CI [1.008, 1.168]). Bad sleep quality and increased sleep time are associated nonsignificantly with obesity and the status of known hypertension.
Demographic Characteristics of Participants
Sleep Quality and Sleep Latency in Different Groups
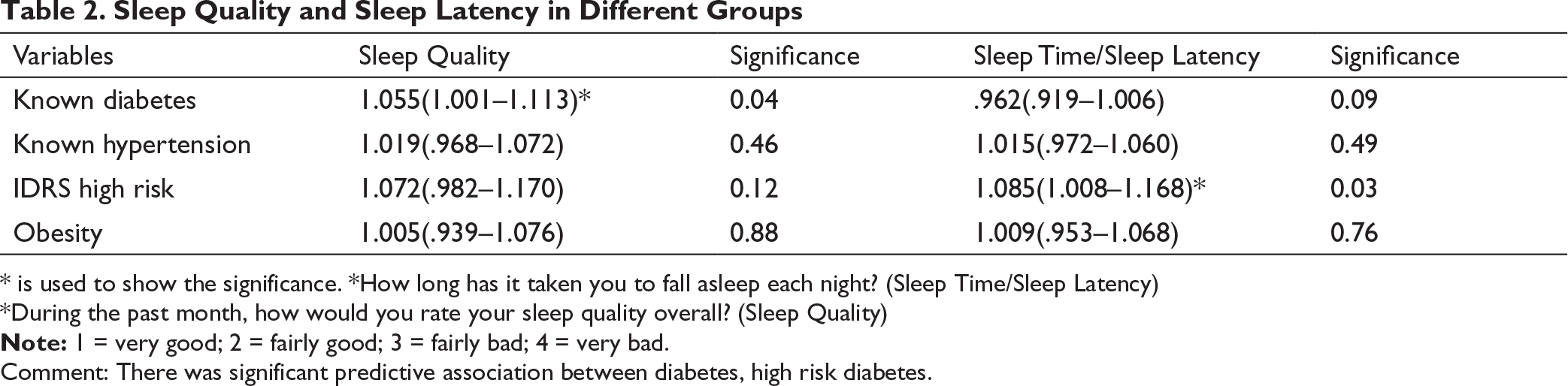
Note: 1 = very good; 2 = fairly good; 3 = fairly bad; 4 = very bad.
* is used to show the significance. *How long has it taken you to fall asleep each night? (Sleep Time/Sleep Latency)
*During the past month, how would you rate your sleep quality overall? (Sleep Quality)
Comment: There was significant predictive association between diabetes, high risk diabetes.
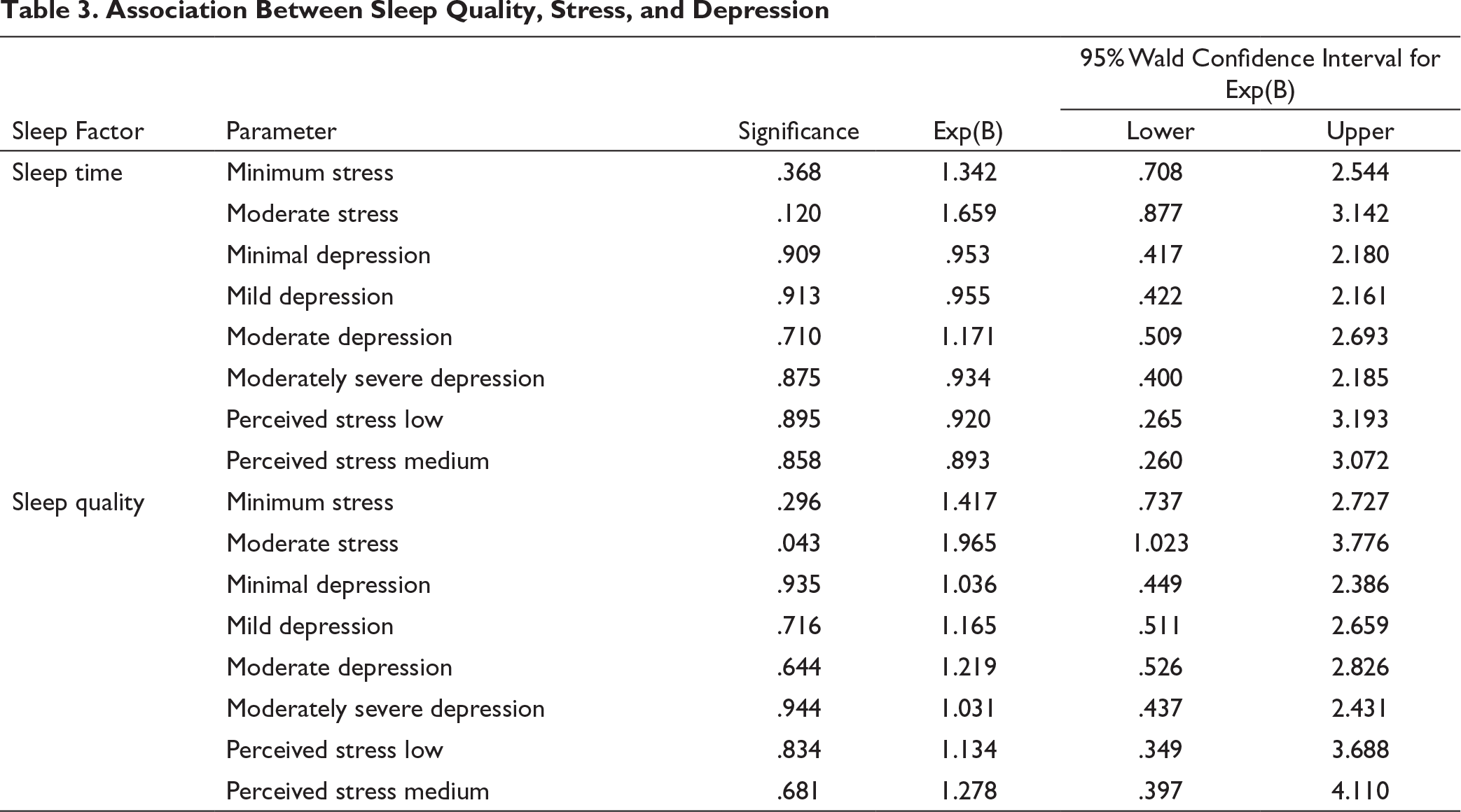
Association Between Sleep Quality, Stress, and Depression
Discussion
This pan-India data that used two general questions to assess the previous month’s sleep quality and sleep latency of the participants revealed a significant positive association of sleep quality and sleep latency with known diabetes and IDRS high diabetes risk, respectively. It was a noninterventional study. So, there is no control group. We have taken nondiabetics to compare diabetic subjects. We have done the regression analysis, and the results showed that moderate stress was significantly associated with poor sleep quality, but not associated with sleep latency.
Earlier studies showed that stress is significantly associated with the bad quality of sleep.26, 27 Our study showed a significant association between moderate stress and poor sleep quality.
A previous study showed complications and durations of diabetes can influence the quality of sleep and depression in a diabetes population. 28 In our study, we checked the association of sleep quality with depression and perceived stress. Even though it shows a positive association, it was not significant.
A cross-sectional study on 332 Gujarati subjects (between 13 and 20 years of age) showed that inadequate sleep does not affect the blood glucose levels in adolescents. 29 That study was on adolescents, but our study was on adults; this seems to point out that although insufficient sleep does not affect the blood glucose level of adolescents, it may affect the blood glucose level of adults. Another cross-sectional study on 1,258 subjects (Indian = 855, Malay = 403) between 40 and 80 years of age showed that the abnormal sleep duration is associated with the diabetic kidney disease. 30 Another review showed that poor sleep quality and short sleep duration were associated with cardiometabolic risk and adverse effects on diabetes, hypertension, obesity, and in turn some epigenetic changes.32–34 Our study showed similar results with a significant association between poor sleep quality and known diabetes. Our study did not show any significant association between sleep quality and obesity or sleep quality and hypertension.
This is the first study from the Indian population consisting of a large sample size where an association between sleep factors and diabetes risk has been demonstrated.
In our earlier studies, we have examined various markers for different neurodegenerative disorders such as age-related macular degeneration,35–40 amyotrophic lateral sclerosis,41, 42 and Parkinson’s disease, 43 and described various treatment strategies for the brain and nervous system, 44 and retinal degeneration. 45 However, in our study, we did not include any biomarker to examine the sleep factor. As sleep is associated with our brain function, therefore further studies can be undertaken to examine the correlation between the neurodegenerative diseases and sleep factor in this diabetic population. Alzheimer’s disease and Brahmi (Bacopa monniera) as one of the treatment modalities for it have also been discussed in our previous review paper.46, 47 An association between memory loss, sleep deficits, and the corresponding interventions such as yoga and Brahmi can add a new dimension to the research in the diabetic population. Our earlier literature has also provided evidence for the correlation between oxidative stress and neurodegenerative disorders 48 and stem cell transplantation for neural disorders. 49 Stress biomarkers and a sleep factor analysis for a larger diabetic population are thus warranted in future. We have developed different animal models for various diseases such as Alzheimer’s disease, 50 and amnesia,51, 52 and also discussed various animal models of neural metabolism for developing the treatment modalities.53 For mechanistic studies, the animal model resources can be used.
Limitation of the Study
The limitation of the study is that a standardized validated questionnaire was not used to assess the sleep factor. So, we were unable to do the domain analysis of different variables of sleep.
Conclusion
Poor sleep quality is associated with known diabetes, and increased sleep latency is associated with a high diabetes risk. Bad sleep quality or SD can be an indicator of diabetes, and increased sleep latency can be an indicator of IDRS high risk. However, further study is required by using a comprehensive sleep questionnaire to confirm the results in the Indian diabetes population.
Footnotes
Acknowledgment
We would like to thankfully acknowledge the Ministry of Health and Family Welfare, and the Ministry of AYUSH, Government of India, New Delhi, India, for funding this project. We would like to thank Dr Ishwar Acharya for his great contribution. He helped in accomplishing this project by monitoring the project and preparing the necessary DVDs (by Mr. Advaitadd a new dimension to the research in the diabetic population. Our earlier literature has also provided evidence fo,r Mrs. Akanksha, and the team) and books for the project. We are appreciative to all individuals of the scientific advisory committee of Niyantrita Madhumeha Bharata (NMB). We would also like to thank the members of advisory committee, members of executive board, each and every individual involved in developing the common yoga protocol for NMBA, and Dr Anand Balayogi Bhavanani, Director, Standing Research Committee of the Indian Yoga Association (IYA), for their simultaneousness and dynamic investment at various periods of the venture. We would like to thank all directors and masters of all the major yoga institutions around the nation for providing trained and responsible yoga volunteers. We thank the software development team for their extraordinary support throughout the project. We are appreciative to all yoga volunteer for diabetes movements, junior research fellows, senior research fellows, and research associates who worked with incredible energy to finish the venture inside the booked timetables under troublesome climate conditions and political and other issues. We express gratitude toward Mr. Jain and the office staff of NMBA. We would like to thank all the staff and students of S-VYASA for their support and service.
Author Contribution
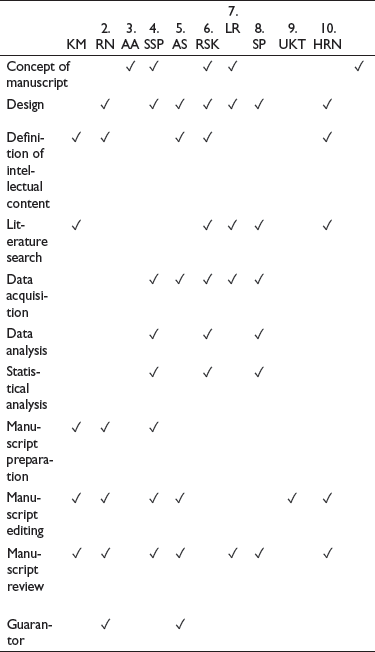
| KM | 2.RN | 3.AA | 4.SSP | 5.AS | 6.RSK | 7.LR | 8.SP | 9.UKT | 10.HRN | ||
| Concept of manuscript |
|
|
✓ | ✓ | ✓ | ||||||
| Design |
|
|
|
|
|
|
|
||||
| Definition of intellectual content | ✓ |
|
|
|
|
||||||
| Literature search |
|
✓ | ✓ | ✓ | ✓ | ||||||
| Data acquisition | ✓ |
|
✓ | ✓ | ✓ | ||||||
| Data analysis |
|
✓ | ✓ | ||||||||
| Statistical analysis |
|
✓ | ✓ | ||||||||
| Manuscript preparation |
|
|
|
||||||||
| Manuscript editing |
|
|
|
✓ | ✓ | ✓ | |||||
| Manuscript review |
|
|
|
✓ | ✓ | ✓ | ✓ | ||||
| Guarantor | ✓ | ✓ | |||||||||
Declaration of Conflicting Interests
Ethical Statement
The study was conducted after obtaining the ethical clearance from the Institutional Ethics Committee (IEC) of Indian Yoga Association (IYA). Written informed consent in their native language was taken from every individual before physical/biochemical assessment. IEC reference no: RES/IEC-IYA/001 (dated. 16/12/2016). CTRI registration no: CTRI/2018/03/01280.
Funding
The Ministry of Health and Family Welfare and the Ministry of AYUSH, Government of India, New Delhi was the funding source for this project.