
Abstract
Background:
The corpus callosum (CC) is a connecting bridge between two cerebral hemispheres and helps in interhemispheric integration of information.
Purpose:
The primary objective of the study is to explain the topographical position of CC in relation to the brain in the South Indian population, contributing to the reference values of measurements of CC, which helps in planning surgical interventions. Also, the reference values help in cross-referencing with other populations and ethnic group.
Methods:
In the study, 40 formalin fixed, full brain specimens were cut in midsagittal plane and CC was measured along with its relation to the brain. The major diameters considered were longitudinal dimension of corpus callosum (LC), distance of CC from frontal pole to genu (AS), distance of CC occipital pole to splenium (PS), and longitudinal dimension of brain (LB) from frontal pole to occipital pole.
Results:
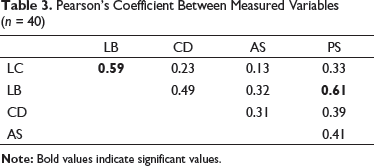
Pearson’s ratio showed a positive correlation between LB and PS (0.61), and also between LB and LC (0.59). The ratio of LC/LB was 0.45 and LC/CD was 0.69, which are stable in all brains studied.
Conclusion:
The study concludes that CC maintains a stable proportion with its parts (genu, rostrum, body, and splenium) and with the horizontal dimension of the brain. Further, measured values help in cross-referencing with other population.
Introduction
The corpus callosum (CC) has the most association fibers, containing 200 to 250 million axonal fibers, connecting the two cerebral hemispheres. The fibers of CC have a topographic distribution and radiate into the white matter core of each hemisphere. CC has influence on the affective behavior, nonliteral language and bilateral functional connection in both motor and sensory cortices.1, 2
There are many studies on morphometric changes related to age,3, 4 sexual dimorphism3–6 and pathological variations. 7 9 The first study was done by R. B. Bean in 1906, and it said that “exceptional size of CC may mean exceptional intellectual activity.” 10
CC helps in coordination of sensory information and execution of bimanual motor activity. Some researchers have reported that the change in size or shape of CC may be associated with pathologies such as Alzheimer’s disease, 7 bipolar disorders, 8 Williams syndrome, 9 and downs syndrome. 11 As CC connects the two cerebral hemispheres, any seizure impulses originating in one half of the hemisphere are transferred to other hemisphere. 12 In patients with uncontrollable seizures, not responding to therapeutic treatment, the second line of treatment is corpus callosotomy, which is quite effective in reducing the seizure frequency in patients having generalized epilepsy with drop attacks. 13
Existing studies on CC were done on Europeans (Caucasian population), Asians, and a few on Indians. There are very few studies reported from South India. In a study by Gupta et al., in the North East Indian population, it was reported that the values were more in Caucasians and less in Japanese when compared to Indian population. 14
Methods
The present study is a cross-sectional descriptive study on 40 freshly autopsied, formalin fixed brain specimens in the age group of 20 years to 60 years, over a period of two years. Ethical approval for the study was obtained from ethical committee. Division of the sample based on gender was not possible in this study. After removal of the brain from cranial vault, during autopsy, they are fixed in a 10% formalin solution (10% formalin has dissolved formaldehyde 3.7%–4%) in basilar suspension for four weeks. All brains with intracranial pathologies, injuries, and neurological abnormalities were excluded, and brains without any injury or abnormality were included in the study. An incision was given in a midsagittal plane, with a cut passing through the median longitudinal fissure, body of CC, third ventricle, and aqueduct. Various callosal distances in relation to the brain were taken with Vernier calipers (least count of 0.01 mm) in a straight-line method.
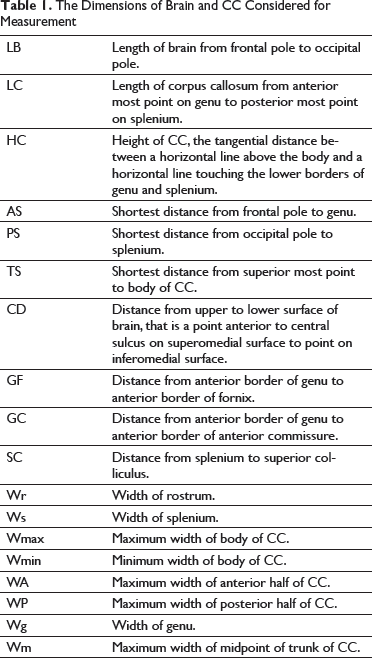
The Dimensions of Brain and CC Considered for Measurement
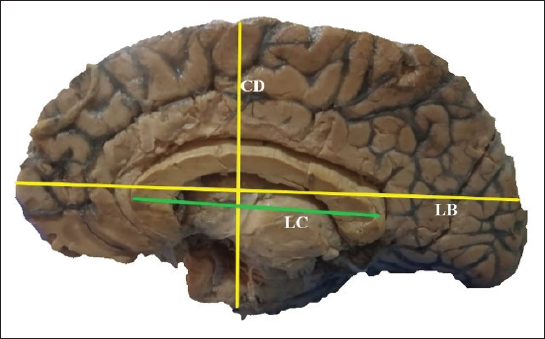
Midsagittal View of Brain Specimen on Medial Aspect Showing Length of Brain (LB), Distance of Brain from Upper to Lower Surface (CD) and Length of Corpus Callosum (LC).
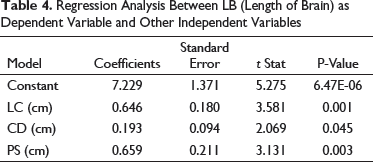
The statistical analysis was done with mean, standard deviation, 95% CI, and the range for each quantitative variable. The mean value was represented as mean ± standard deviation. For all correlations, P-value less than 0.05 was taken as significant. Evaluation of relation was done using Pearson coefficient between dimensions of brain and dimensions of CC. Multivariate linear regression analysis was done to correlate between LB as dependent variable and LC, CD, and PS as independent variables.
Results
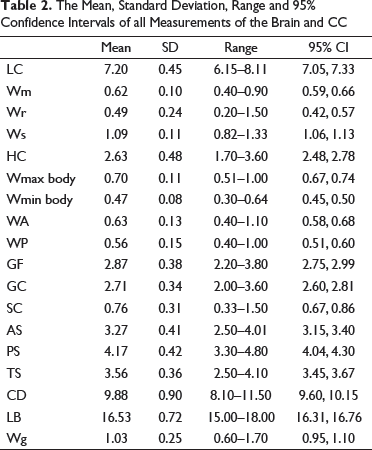
The mean value for longitudinal dimensions of brain (LB) was 16.53 ± 0.72cm (95% CI [16.31, 16.76]), and the mean value for longitudinal dimension of CC (LC) was 7.20 ± 0.45cm (95% CI [7.05, 7.33]); the ratio between them is greater than 2:1.
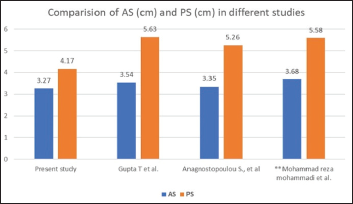
The mean value for shortest distance between frontal pole and genu (AS) and shortest distance between occipital pole and splenium (PS) was 3.27 ± 0.41 cm (95% CI [3.15, 3.40]) and 4.17 ± 0.42 cm (95% CI [4.04, 4.30]), respectively, with the ratio between them being 1:1.3.
The Mean, Standard Deviation, Range and 95% Confidence Intervals of all Measurements of the Brain and CC
In our study, new parameters were also considered and measured, along with the parameters considered in other studies, which helps in increasing the reference index values.
Pearson’s Coefficient Between Measured Variables (n = 40)
Regression Analysis Between LB (Length of Brain) as Dependent Variable and Other Independent Variables
Further, the documented values of CC and brain were compared with values obtained from other studies from North India, Greece, and Iran (Figure 2, Figure 3, Figure 4, and Figure 5).
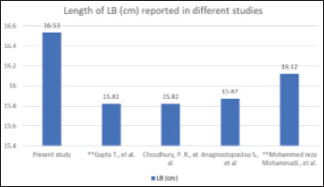
Comparison of LB (cm) from Present Study with Values Reported from Other Studies (** Indicates MRI Study).14, 22, 18, 23
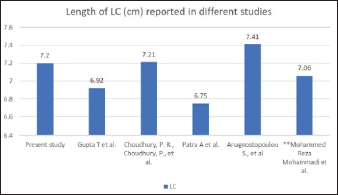
Comparison of LC (cm) from Present Study and Values Reported from Other Studies (** Indicates MRI Study).14, 22, 17, 18, 23
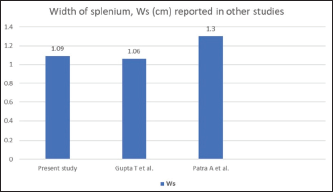
Comparison of Ws (cm) from Present Study and Values Reported from Other Studies (** Indicates MRI Study). 14, 17
Comparison of AS (cm) and PS (cm) from Present Study and Values Reported from Other Studies (** Indicates MRI Study).14, 18, 22
Discussion
If there are any morphological changes related to the structure or position of CC, they should be identified and related to the pathology. Hence, there is a need to explain the position of CC in relation to the brain, and normal reference values should be documented and referred to before planning a surgery. Studies documenting reference values in South India are few and, with the present study, we try to add to the literature. In a study by Teipel et al., 11 they reported that there was a reduction in overall area of CC by roughly 7.7% per year in Alzheimer disease when compared to 0.9% in normal controls. Further, they proposed that longitudinal measurement of CC can act as a marker of progressive neocortical neuronal degeneration in patients of Alzheimer disease along with CC area. In another study on subcortical ischemic vascular dementia (SIVD) (subtype of dementia), it was reported that thickness of genu, anterior third, middle and posterior third of body, and splenium of CC were smaller in SICD patients as compared to healthy subjects. 16
In our study, the measurements taken were all in a particular range, and the proportion of CC, in relation to the brain, was similar in all the brains studied, showing that CC maintains a stable position. There is a positive correlation between the horizontal length of brain (LB) and the vertical length of brain (CD), which shows that any change in dimension of LB will also cause a change in CD.
The other parameters, that is, length of CC (LC), have a positive correlation with the horizontal length of brain, which is in accordance with studies by Patra et al. 17 and Anagnostopoulou et al. 18
The distance between AS and PS has a positive linear correlation with each other and with the length of the brain (LB).
The length of the brain (LB) has a positive linear correlation with all the parameters of the brain, that is, CD, LC, AS, and PS, with a strong correlation with PS (distance between splenium and occipital pole), which is in accordance with the studies by Anagnostopoulou et al. 18 and Patra et al., 17 which explains the increased development and distribution of visual cortical fibers to the occipital pole.
The findings in this study showed that there is a significant correlation between LB and LC but not between CD and LC, so any increase in length of the brain will cause an increase in the length of CC, but changes in CD doesn’t affect LC, and these findings are in agreement with those by Anagnostopoulou et al.
The ratios LC/LB = 0.45 and LC/CD = 0.69 showed a stable significant finding present in all the brain specimens studied. The ratios can be considered as reference values before any surgical procedure. Also, a study by Patra et al. 17 reported similar ratios of LC/LB (0.43) and LC/CD (0.73), though slightly different when compared to the current study.
The aforementioned findings show that horizontal dimensions of the brain have a statistically significant positive relation with the size of CC, which is consistent with the findings of other studies on cadaveric brain specimens. In the late 1960s, callosal transection was introduced as treatment for intractable epilepsy and laid the foundation for studies on CC.19, 20 Oguni et al. reported that anterior two-third callosotomy has excellent outcome when compared to anterior half. 21 Depending on the type of seizures and epileptogenic focus, the part of CC to be removed is planned. Patients with epileptogenic focus in the frontal lobe benefit from anterior callosotomy. Total or subtotal callosotomy is followed by neuropsychological sequels, which can be reduced if some of CC can be preserved.
Recent advances are more focused on MRI-guided stereotactic laser ablation of specific callosal tissues. The anatomical values and ratios can be applied on MRI films, and individual parts of CC can be defined. This helps in more targeted callosotomy and reduces the neuropsychological sequel after callosotomy.
Furthermore, the measured length of brain and CC from the present study were compared with similar studies done from other regions and countries. The value of LB and LC recorded was more in the present study when compared with studies from North India. 14 The value of PS recorded from South India was less when compared to North India, 14 and the value of CD recorded was more in a study from north Iran. 22 The values of LB, LC, Ws, AS, and PS from other studies were compared with the present study and presented in charts (insert Figure 2, Figure 3, Figure 4, and Figure 5).
Conclusion
This study concludes that the brain maintains symmetry along its horizontal and vertical dimensions, and the position of CC is stable in relation to the horizontal dimension of the brain. The normal measurements and the ratios of brain and CC from the South Indian population add to the existing literature. Also, any abnormalities in dimensions of CC can be identified with the help of reference values from the current study and can be correlated to pathologies. Further, during any surgical intervention related to CC, the aforementioned values can be used as a reference to prevent any unwanted outcomes. They can be also be used to compare with other population and ethnic groups.
Footnotes
Acknowledgments
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind’s overall knowledge, which then improves the patient care. Therefore, these donors and their families deserve our highest gratitude.
Authors’ Contribution
S.R.P and L.V conceptualized the procedure while S.R.P and L.D.J have collected the data. A.K and S.R.P have done the statistical analysis, M.C revised it for critical intellectual content. Manuscript was prepared by S.R.P under the supervision of M.C.
Statement of Ethics
Before initiating the study necessary approval was taken from the Institutional ethical committee.
Declaration of Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.