
Abstract
The cranio-cerebral trauma following gunshot injuries has high mortality and morbidity, with 66% to 90% victims dying before reaching hospital and only half of those treated in hospital surviving. However, in case of most salvageable patients, the question which poses dilemma to treating physicians is the decision as to when and why remove the retained missile.
A 21-year-old man was observing a gunfight in the street from his balcony. Suddenly something struck his forehead and there was a small amount of bleeding toward the medial end of his left eyebrow. He had moderate headache and dizziness. Because of nonresolution of headache over seven days he was hospitalized and underwent X ray of the skull and CT of the head, which showed a retained metallic bullet in left inferior parieto-occipital region without any significant hemorrhage. As there was no neurological deficit or meningeal signs, he was managed conservatively. His symptoms improved gradually within next week and he was discharged home. His most recent follow-up was 28 months since injury and imaging showed migration of the bullet to the right inferior temporal region. As he was completely asymptomatic throughout, no intervention was offered. However, long-term follow-up for potential complications of migration, hydrocephalus, and abscess formation is advisable.
Introduction
The cranio-cerebral trauma following gunshot injuries has high mortality and morbidity, with 66% to 90% victims dying before reaching hospital and only half of those treated in hospital surviving. 1 However, in case of most salvageable patients, the question which poses dilemma to treating physicians is the decision that when and why remove the retained missile? 2 Patients can present in good neurological status and may continue to do well on long-term basis.
Case History
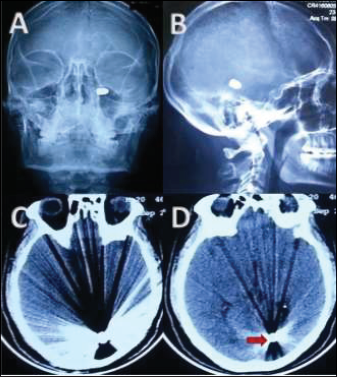
A 21-year-old man was standing in his first floor’s balcony while observing a gunfight in the street below. Suddenly something struck on his forehead with a small amount of bleeding over medial end of his left eyebrow. He remained symptomatic for about seven days with moderate headache and dizziness and was then hospitalized. Because of nonresolution of headache over days he underwent cranial radiology in the form of CT of the head and X ray of the skull (Figure 1) which showed a retained metallic bullet in left inferior parieto-occipital region without any significant hemorrhage. As there was no neurological deficit or meningeal sign, he was managed conservatively. His symptoms improved gradually within next week and he was discharged home. He returned for follow-up after around 20 months and repeat radiology showed that the retained bullet had migrated to the right temporal region (Figure 2). As he was completely asymptomatic throughout, no intervention was offered. His most recent follow-up was 28 months since injury, which revealed the same position of the bullet at right inferior temporal region (Figure 3). He presently shows no symptoms or deficit.
(A, B) AP and Lateral X Ray Skull; (C, D) Axial CT of Brain Demonstrated the Retained Bullet in Left Parieto-Occipital Region, Seven Days Following Injury.
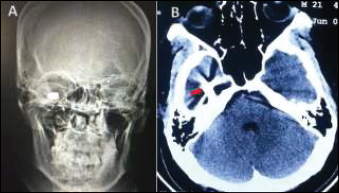
(A) X-Ray Skull, (B) Axial CT Brain, at 20 Months Post Injury Revealing Migration of Retained Bullet to Right Temporal Horn.
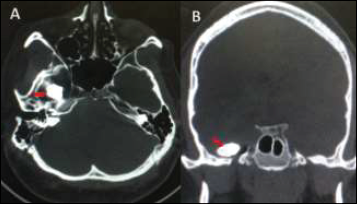
(A, B) Axial and Coronal CT Images During Last Follow-up at 28 Months Since Injury (Bone Windows With Metal Artefact Reduction and Reconstructions) Showing Same Position of Bullet as in the Previous Scan.
Images of Last Follow-up (A) 3D Reconstruction of Skull Showed the Bullet Entry Point. (B) Tiny Scar Mark Above the Medial End of the Left Eyebrow Showing the Bullet Entry Point.

Discussion
The current indications for removal of an intracranial retained bullet(s), although controversial, may be summarized as follows:3, 4, 5 (a) patients who undergo surgery for the evacuation of hematoma or significant cerebral swelling and bullet/fragments are easily accessible or superficial, (b) if bullet fragments cause development of an abscess, (c) when the retained bullet causes neurological deterioration because of its migration, (d) bullets within the ventricular system because of their propensity of causing hydrocephalus, (e) heavy metal toxicity, and (f) if bullet is reasonably accessible and can be removed without causing additional neurological deficit.
The above person was probably having bullet into the occipital horn of left lateral ventricle that later migrated to the right temporal horn which is a more anatomically dependent position, followed by its marginalization stopping its further migration as indicated in the last two follow-ups. However, long-term follow-up for potential complications of migration, hydrocephalus and abscess formation is advisable. A brain abscess has been known to occur as late as 30 years after injury in relation to a deep-seated retained metallic fragment. 6 This should underscore the importance of adequate follow-up in such souvenir bullets.
Footnotes
Author Contributions
Concept, patient recruitment, data acquisition, analysis and manuscript preparation was performed by Rajnish Kumar Arora. Patient recruitment, data acquisition, analysis and manuscript preparation was performed by Srikant Kumar Swain. Concept and the intellectual content, Manuscript edited and reviewed by Dr RadheyShyam Mittal.
Declaration of Conflicting Interests
Ethical Statement
An informed patient consent was obtained for publication of photographs and details.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.