
Abstract
Introduction: The objective of this study was to find the immediate as well as short-term effect on pelvic alignment and forward arm reach distance in sitting among stroke patients following thoracic spine and abdominal muscles taping along with conventional therapy.
Methods: Thirty subjects with stroke attending the physiotherapy programme at Department of Physiotherapy at a tertiary care hospital underwent this randomized controlled experimental study. Subjects in the experimental group received taping, along with conventional physiotherapy treatment, for restricting thoracic kyphosis and facilitating abdominal muscles. Subjects in the control group received only conventional physiotherapy treatment. To assess the change in pelvic alignment and forward arm reach distance while sitting, Palpation MeterTM (PALMTM) and sit and reach test were used, respectively.
Results: In the experimental group, pelvic obliquity was corrected (4.1 ± 0.94) and anterior pelvic tilt revealed improvement (4.9 ± 2.1, p value < 0.001). In the control group, no improvement in pelvic alignment was recorded. Improvement in forward arm reach distance was similar in both groups (p value = 0.804).
Conclusion: Taping as an adjunctive treatment method to physiotherapy can cause immediate as well as short-term improvement of pelvic alignment in sitting, following stroke. It also, immediately improves the sit and reach distance in the same population.
Introduction
Stroke, one of the major causes of disability, results in sensory and motor impairment which influences postural control, balance and postural symmetry.1, 2 Stroke survivors often adapt compensatory strategies to maintain balance which leads to poor sitting ability.3, 4 Sitting, being a skill that is critical to independent living, is one of the useful prognostic indicators of functional outcome for stroke population. Re-establishment of control in sitting for function is an important early goal in stroke rehabilitation. 5
In sitting, postural control depends on trunk alignment, 6 particularly the position of pelvis.7, 8 Due to disturbed postural symmetry, stroke subjects sit with flexed thoracic spine and often show lateropulsion, characterized by elevation of pelvis on the unaffected side, lateropulsion probably results from compensation of weak bilateral trunk lateral flexors and rotators.7, 9 Postural asymmetry following stroke may limit the ability to independently perform reach-out activities. 3 Earlier literatures10–12 have used Palpation Meter (PALMTM) and sit and reach test (SRT) 13 to objectively assess the pelvic asymmetry and forward reaching distance, respectively.
Considerable amount of work has been done in training the postural symmetry for stroke subjects, in standing and gait using treatment techniques including Bobath’s, motor learning, task-related training and feedback approach.3, 4, 14 Among chronic stroke subjects, during ambulation, for immediate correction of postural asymmetry, taping has been used. Hypoallergic sports tape helps to align the joint and enhance muscle retraining by balancing the tissue length–tension relationship, thus assisting neuromuscular control and postural re-education. Taping may also improve joint proprioception and effective loading of the affected extremity and may minimize thoracic kyphosis and facilitate abdominal muscles.15–17 Studies related to immediate and short-term effect of taping on pelvic alignment and forward arm reach distance among stroke subjects are limited. The purpose of this study was to find the immediate and the short-term (three-day) effect of taping thoracic spine and abdominal muscles to improve pelvic alignment and forward arm reach distance in sitting.
Methods
Design
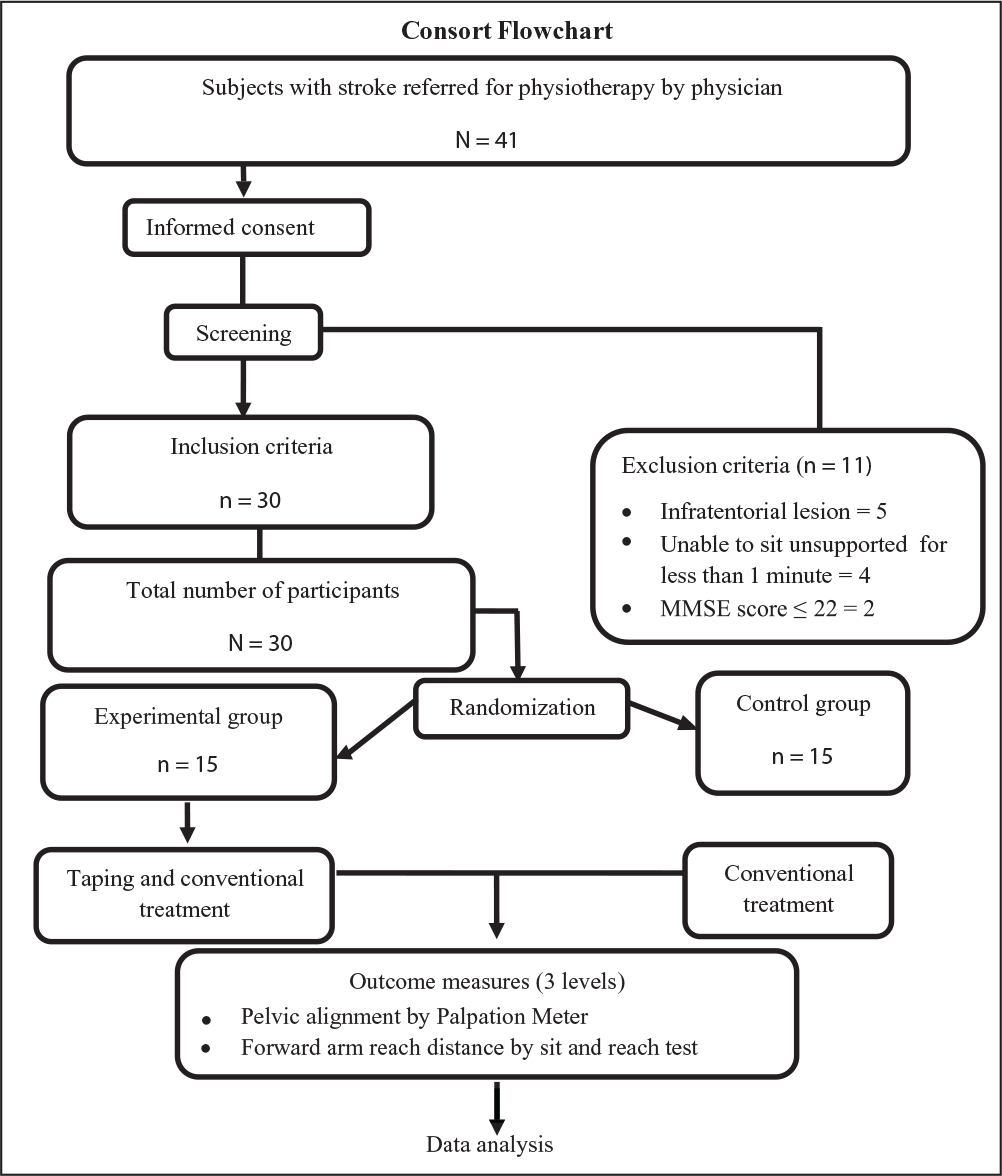
Following approval from the Institutional Ethics Committee (IEC), Kasturba Medical College, Mangalore, Karnataka, India, a pilot study was performed on five stroke subjects to calculate the sample size, feasibility and flaws in the methodology. During the study period (March 2011–February 2012), informed consent was obtained from each subject referred by the neurologists. A total of 41 interested stroke participants (excluding the five stroke subjects who participated for the pilot study) were screened for the inclusion and exclusion criteria and 30 subjects who met the inclusion criteria were enrolled for this study. Eligible subjects were assigned to the study groups by block randomization. Block size of 6 was used in the trial to allocate the participants to two study groups; each block consisted of three experimental and three control interventions. The allocation concealment was done using sealed opaque envelopes which were sequentially arranged. Post allocation of subjects into experimental (n = 15) and control (n = 15) groups, baseline data and demographic data of the eligible participants were taken. Both the groups received three days of conventional physiotherapy and the experimental group received taping as an adjunct. The outcomes were assessed by a blinded independent assessor at three levels. Level 1 (baseline data) was one day before the commencement of the treatment session, level 2 was immediately after the first treatment session and level 3 was immediately at the end of the third treatment session.
Participants, Therapists, Centres
The study was conducted at the Department of Physiotherapy, in the study institute. Following screening for the inclusion and exclusion criteria, 24 hours before the commencement of the study, patch tests were performed to check whether eligible participants were allergic to tape.
First episode of unilateral supratentorial stroke diagnosed by the neurologist Sitting unsupported on a stable surface for more than 1 minute MMSE score of ≥23.
Any known disease other than stroke that could influence the sitting balance Pusher syndrome or other perceptual deficits Loss of skin integrity or hypersensitive skin in the part where taping needs to be applied.
Both the principle investigator and the independent blinded observer were qualified physiotherapists of the Department of Physiotherapy.
Intervention
Both groups received conventional physiotherapy focussing on the length of muscle, normalization of tone, motor control improvement, strengthening for hemiplegic side extremities and trunk, and balance training. Each treatment session lasted for approximately an hour. The distribution of time spent and the number of repetitions given for each component of conventional therapy was uniform for all the participants.
The experimental group received taping along with conventional physiotherapy. The skin area where taping was applied was cleaned with medical spirit. Prior to the application of the tape, to remove skin hair, the area was shaved. For providing and maintaining proper alignment, first Fixomull® (BSN Medical, Hamburg, Deutschland) stretch tape, which is an underwrap to avoid skin damage, was applied prior to the application of a 2 inch width rigid Leukotape® (BSN Medical, Hamburg, Deutschland). Based on the previous literature,17, 18 to restrict and correct the thoracic kyphosis, each participant was made to sit with erect spine with or without assistance and tapes were applied diagonally across the upper back starting from the anterior aspect of shoulder towards inferio-medial aspect of the scapula. Similarly, to facilitate the oblique muscles on either side, each of the participants was positioned supine with hips flexed to approximately 45° to place the pelvis in neutral position and shoulders flexed over head to elongate the trunk musculature. The length of the tapes were measured from participants’ anterior superior iliac spine (ASIS) to the opposite 10th rib, following which the tapes were anchored at the ASIS and applied towards the participants’ 10th rib stretching across the umbilicus. Figures 1 and 2 depict the post-application appearance of tapes for restricting thoracic kyphosis and facilitation of abdominal muscles, respectively. All the participants were able to tolerate the taping protocol until it was removed on the third day following the completion of the trial. The flowchart of the study is given in Figure 3.


Outcome Measures
To evaluate the pelvic alignment and forward arm reach distance, the PALMTM and SRT were used respectively. For pelvic alignment, each participant was made to sit on a plinth with no back support, with thighs fully supported on plinth, hips, knees and ankles at 90° of flexion, and feet positioned flat on the floor in the same line with the knees. Commands like ‘sit as tall as possible’ or ‘sit tall’ were given after positioning. Pelvic obliquity was measured in the frontal plane and the anterior pelvic tilt was measured in the sagittal plane. Pelvic obliquity was measured in degrees, with the lever arms of the PALMTM placed on the left and right ASIS (Figure 4). The direction of obliquity (i.e., the left or right side lower) was noted based on the earlier literature. 10 Anterior pelvic tilt on the hemiparetic side was measured with the lever arms of the PALMTM placed on the ASIS and posterior superior iliac spine (PSIS) of the hemiparetic side (Figure 5). Three test trials of pelvic obliquity and anterior pelvic tilt were performed, and the mean reading was used for analysis. Standard procedure was used for measuring the forward arm reach distance using SRT. 13
Data Analysis
The collected data were analysed using IBM SPSS for Windows, Version 25.0 (IBM Corp, Armonk, NY). Normality of the outcome measures was statistically verified using the Kolmogorov–Smirnov Z test. For between group comparison, Student’s t test was used. For within group comparison, paired t test was used. Chi square test was used for descriptive statistics. A p value of less than 0.05 was considered as statistically significant.
Result
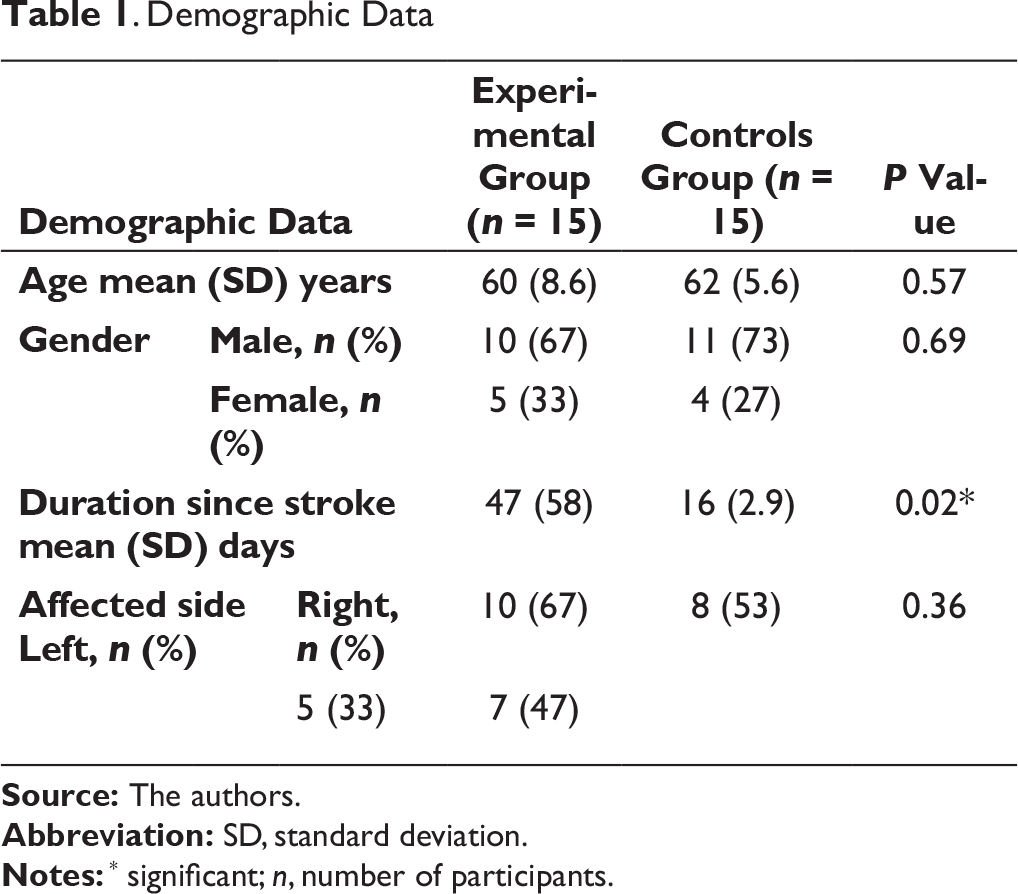
Baseline characteristics of experimental and control groups are depicted in Table 1. Except the duration since stroke (p = 0.02), all the variables were similar between the groups. In order to find the immediate effect of taping, level 1 and level 2 data within the experimental group were compared and to find the short-term effect, level 1 and level 3 data for either group were compared.


Demographic Data
Pelvic Alignment
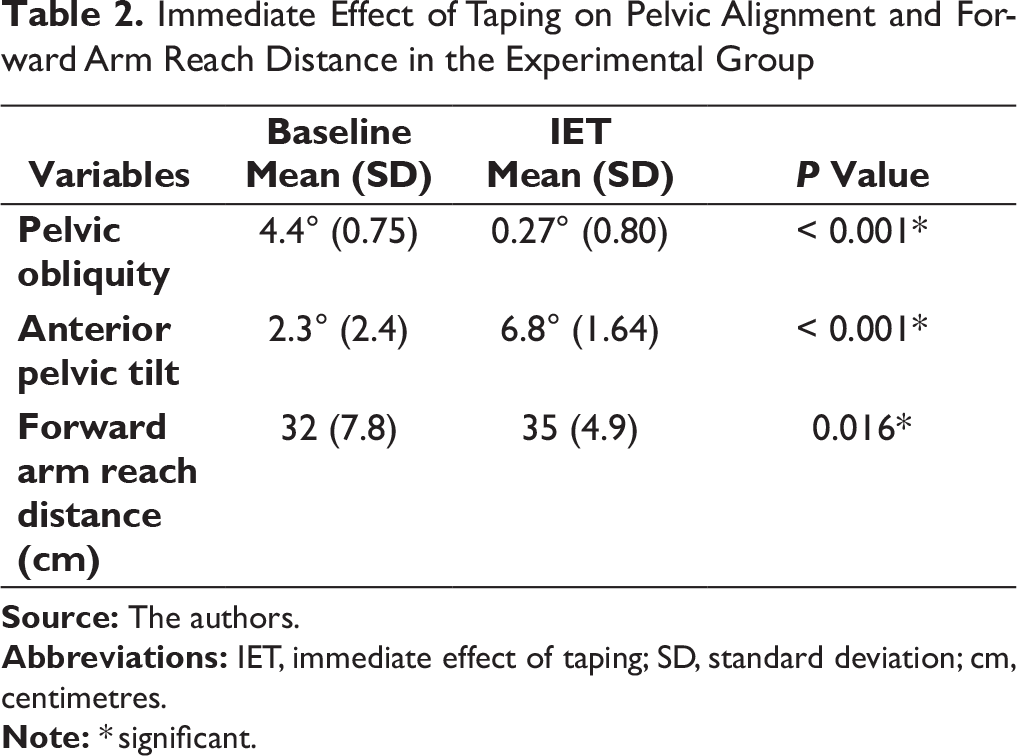
Taping had shown statistically significant improvement in pelvic obliquity and anterior pelvic tilt in the experimental group. As shown in Table 2, pelvic obliquity improved and reached closer towards neutral and anterior pelvic tilt improved by 4.5°.
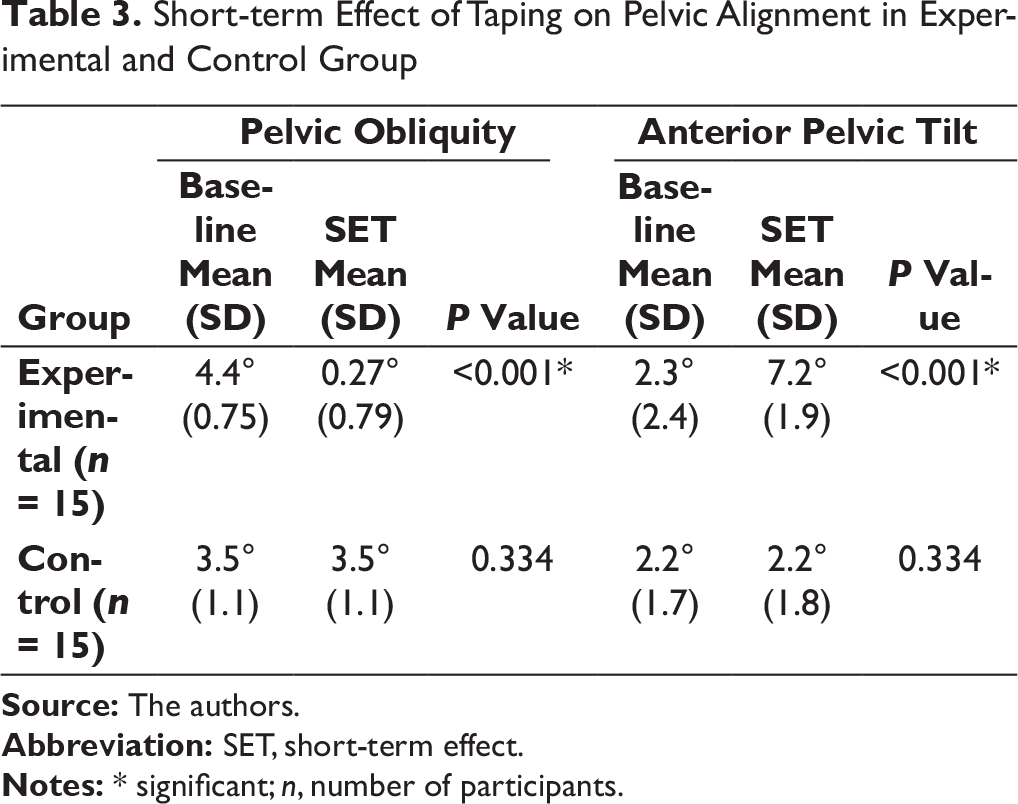
There was significant short-term improvement in the pelvic alignment within the experimental group. Pelvic obliquity improved towards neutral and anterior pelvic tilt improved by 4.9°. On the contrary, within the control group, pelvic obliquity remained the same and anterior pelvic tilt increased marginally to 0.07° which was statistically not significant (Table 3).
Forward Arm Reach Distance
Immediate Effect of Taping on Pelvic Alignment and Forward Arm Reach Distance in the Experimental Group
Short-term Effect of Taping on Pelvic Alignment in Experimental and Control Group
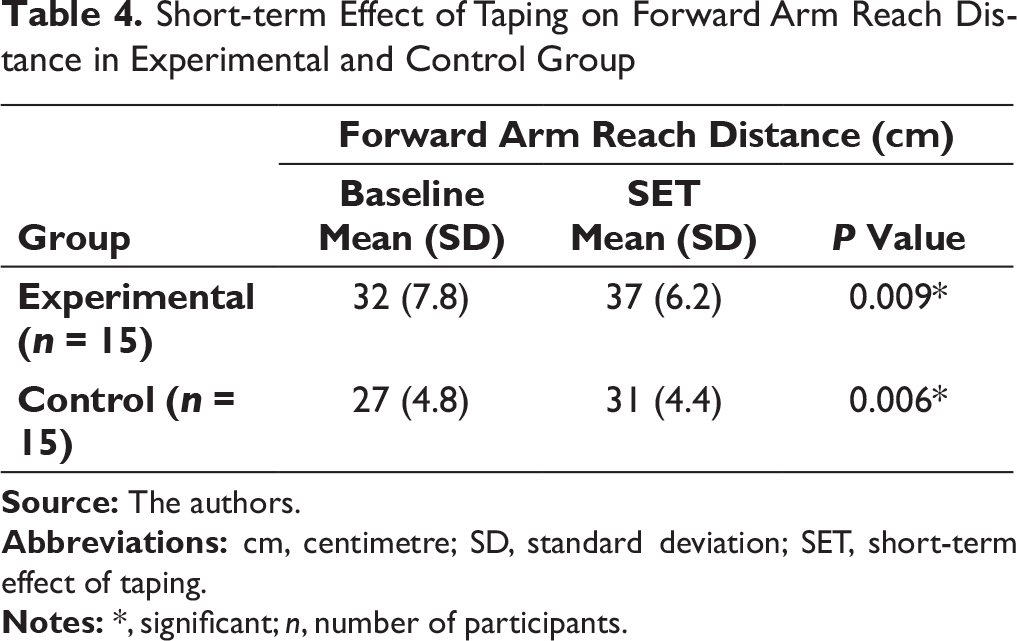
Short-term Effect of Taping on Forward Arm Reach Distance in Experimental and Control Group
Change Scores of Pelvic Alignment and Forward Arm Reach Distance in Experimental and Control Group
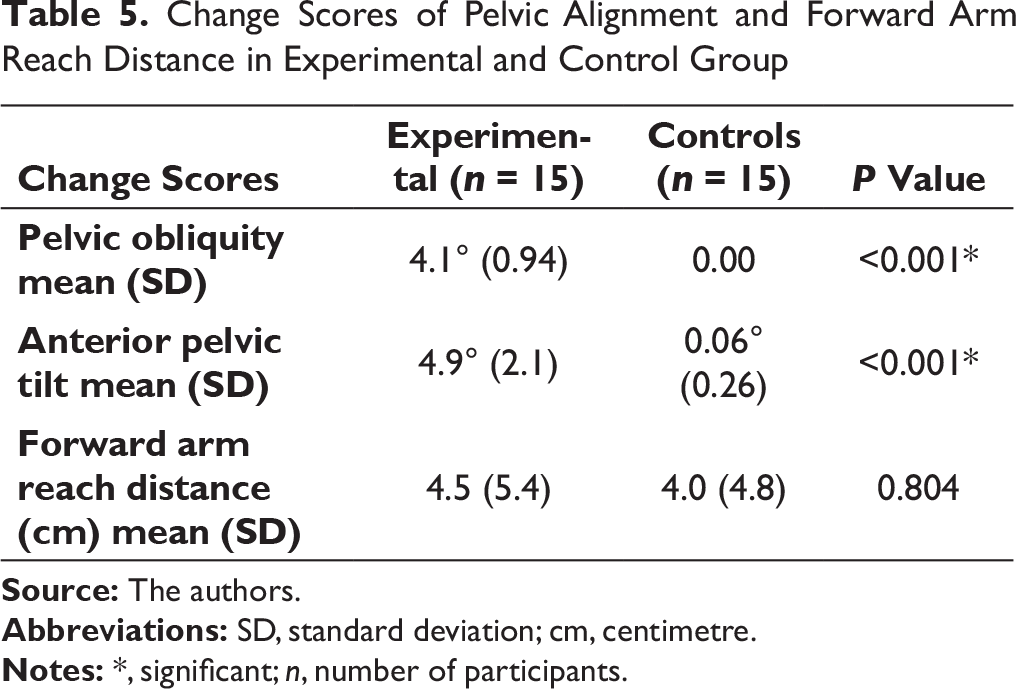
Table 5 depicts the change scores (pre to post intervention difference) of pelvic alignments and forward arm reach distance across the experimental and the control groups. Except for the forward arm reach distance, the experimental group showed statistically significant improvement in postural alignment when compared to the control group.
Discussion
To the best of our knowledge, this is a preliminary study to examine the immediate and the short-term effect of taping as an adjunct to conventional physiotherapy in improvising sitting postural control. In this study, we assumed that taping of the thoracic spine and abdominal muscles may improve the pelvic alignment and forward reach among stroke patients.
Descriptive statistics of demographic data revealed significant difference in post-stroke duration in experimental and control groups (Table 1). Inclusion of three participants with post-stroke duration of more than three months under the experimental group made the post-stroke data skewed; otherwise, all the rest of the parameters were comparable between the groups.
Thirteen out of fifteen participants in the experimental group were able to achieve neutral horizontal alignment. Remaining two subjects achieved near-neutral alignment. In addition to the above, the participants also exhibited increased anterior pelvic tilt. Furthermore, this improvement was maintained for three days. Present study findings reveal that the improvement in pelvic alignment could be the result of taping, as conventional treatment was common for both the experimental and the control groups.
Efficient stabilization of spine required for the static and dynamic normal posture is produced by the passive osteoligamentous system, active musculotendinous system and neural control system. 19 In stroke, impairment of the latter two systems leads to altered alignment and disturbed postural symmetry. 20 The results of this study suggest that taping may have improved the active musculotendinous and the neural control component of the stabilizing system of the spine leading to improvement in the pelvic alignment, that is, taping prevented thoracic kyphosis by positioning the pelvis in neutral, thus, promoting better recruitment of obliques. The current findings are reinforced by earlier works of Maguire et al and Kilbreath et al.15, 16
Hemiparesis results in pronounced weakness of the affected side trunk muscles, 21 with more weight bearing on the unaffected side, elevation of pelvis on the affected side and with impaired sitting balance.9, 22 Though the forward reach in sitting improved in either group, visual inspection of change scores (4.5 cm for experimental group and 4.0 cm for control group) reveals a better result for the experimental group, indicating that the improvement could have been the result of improved postural symmetry and enhanced recruitment of trunk muscles.
Repeated practice might have improved perceptual processes involved in coordinated movement and execution of task 23 and the same would have been responsible for improvement in the forward reach for either group. Besides, subjects in both the groups had relatively normal balance at the beginning of the study as represented by their baseline value for forward arm reach distance, resulting in an almost parallel improvement in sitting balance.
The current study had paid attention to check the immediate and short-term effect of taping on postural control, and not the carry-over or long-term effect of taping. Care is to be taken while generalizing the effect as the current study used a smaller sample size. Future studies are required to see the effect of taping on other functional activities. Incorporation of objective outcome measures for quantitative analysis of the improvement, such as kinematic analysis of reaching and forced platform analysis of postural symmetry in sitting, may provide additional information including true motor improvement and the plausible compensations.
Conclusion
The result of this study indicates that taping as a treatment adjunct can result in immediate as well as short-term improvement of pelvic alignment while sitting. It may also result in immediate improvement of sitting balance among stroke patients and may prevent adverse effect of postural asymmetry in sitting following stroke.
Footnotes
Acknowledgements
We would like to thank Manipal Academy of Higher Education, Manipal, India, and all the participants of the study for all the support.
Author Contributions
Megha Mehta was the principal investigator for this study. Conceptualization of the study was by Abraham M. Joshua. Supervision of the trial and data collection was done by Suruliraj Karthikbabu. The study was designed and the data analysis was executed by Bhaskaran Unnikrishnan and Prasanna Mithra. Zulkifli K Misri and Akshatha Nayak provided critical inputs and aided with data management. Authors of this study had equally contributed in preparation and editing of this manuscript.
Ethical Statement
The Institutional Ethical Committee (IEC), Kasturba Medical College, Mangalore, Karnataka, India, approved this study. All participants gave written informed consent before data collection began.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was partially funded by, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, India.