
Abstract
This study aims to assess the performance of World Health Organization European Region nations in achieving their Health 2020 targets using multi-criteria decision-making approaches and the core indicators defined in Health 2020. These assessments were conducted in two periods based on 2010 and 2019 data, and the relative success of the countries in meeting the targets was compared. The CRiteria Importance Through Inter-criteria Correlation (CRITIC), COmbinative Distance-based ASsessment (CODAS), Evaluation based on Distance from Average Solution (EDAS), and Technique for Order Preference by Similarity to Ideal Solution (TOPSIS), which are part of the Multi-Criteria Decision-Making (MCDM) family, as well as the Borda count approach, are used to show the country’s performance based on a set of core indicators. Norway and Iceland were the best-performing countries in both years, according to the Borda ranking, which incorporates the results of three independent approaches. Armenia, Moldova and Kyrgyzstan, on the other hand, did not make any improvement throughout any year and ended up as the poorest countries. Belarus, Estonia and Ireland were among the countries that made the most progress. Cross-country comparisons can be used as a basis for proper policy creation by decision-makers and policymakers in the countries studied.
Introduction
The World Health Organization (WHO) regional office for Europe and the 53 European member countries developed and agreed on ‘Health 2020: A European Policy Framework and Strategy for the twenty-first century’, which aims to improve community health and well-being, reduce health inequalities and ensure sustainable people-centred health systems in Europe. Member nations require WHO support in determining and developing policies to address and resolve regional health challenges encountered in the WHO European region, which includes 53 of the WHO’s 194 member countries and affects a population of over 900 million people. The Health 2020 framework emphasises that excellent health benefits everyone and that countries may achieve the highest health standards by working together across government boundaries. For all countries, this policy framework is adaptable and practical (WHO Regional Office for Europe, 2013).
For many years, policymakers and decision-makers have placed a premium on the development of health systems. Furthermore, actions aimed at improving the performance of health systems have received a lot of traction. Reforms are carried out in a variety of areas for this purpose, including reimbursement systems, health insurance and public and private sector laws, to name a few. Another issue that policymakers are concerned about is the success of these reforms. The outcomes of all reforms have been the subject of several studies. Simultaneously, investigations examining the findings have continued. Some indicators, however, are required to track these outcomes (Evans et al., 2001). Pandemics, migration, ageing, chronic diseases and other issues have been addressed by health systems, but conditions continue to pose a challenge. Many countries are focused on their own healthcare systems, yet global issues affect all countries (World Health Organization, 2007).
The health policies established by the countries vary, particularly in terms of disease prevention programmes. Different health strategies show that countries can learn a lot from one another (Rosso et al., 2015). Many studies concentrated on high-income countries. In comparative health systems research, low- and middle-income nations have been put in the background, resulting in an information gap. Furthermore, just a few indicators of nations’ comparative health systems should be included in the study, such as social concerns, technical and clinical variables and methodological concerns (Healy et al., 2018).
Using the basic indicators defined in the Health 2020 document, this study attempts to assess the success of the WHO European Region countries in achieving their Health 2020 targets. Multi-criteria decision-making (MCDM) strategies are utilised for this aim.
Health 2020 Policy Framework
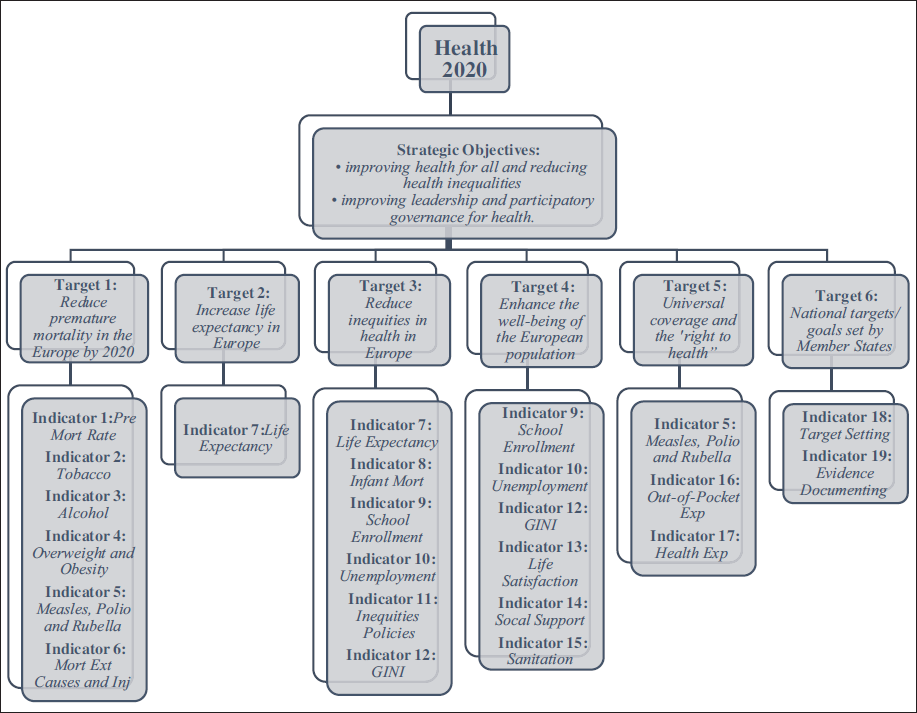
Health 2020 highlights the health challenges faced by countries across the European Region as a whole. While the pattern may differ from country to country, the key overarching issues apply to all. However, Health 2020 focuses on identifying problems as well as potential solutions and areas where evidence suggests that positive action can have important effects (WHO Regional Office for Europe, 2013). As part of the policy framework developed to guide member countries, WHO Regional Office for Europe’s expert team identified 19 core and 18 additional indicators to be followed in achieving two strategic objectives and six targets. Some of these indicators are used in conjunction with more than one target. Health 2020 strategic objectives, targets and core indicators determined are shown in Figure 1 (WHO Regional Office for Europe, 2016).
Health 2020 Strategic Objectives, Targets and Core Indicators.
Related Works
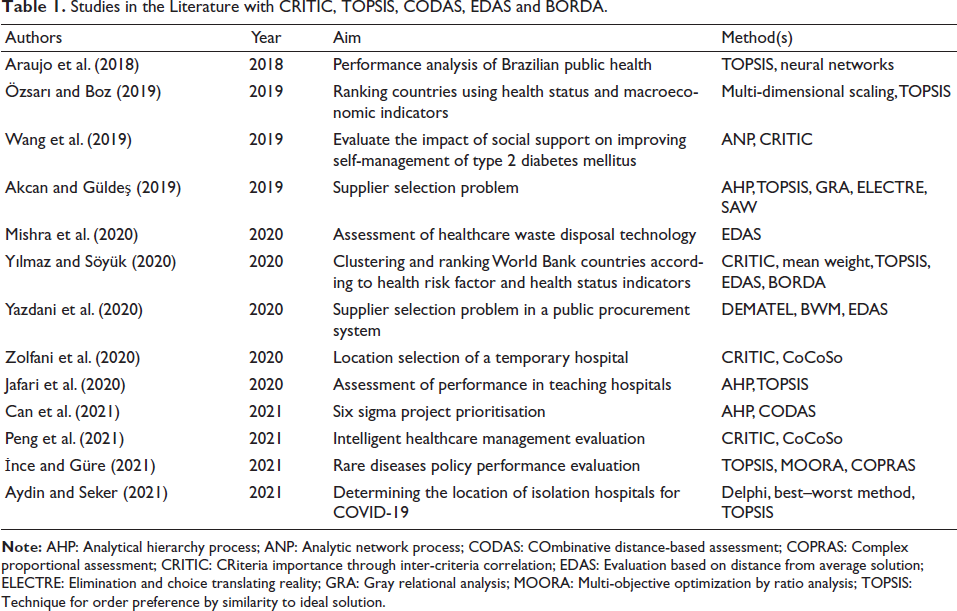
Studies in the Literature with CRITIC, TOPSIS, CODAS, EDAS and BORDA.
Data
In this research, it is aimed to evaluate the performance of the WHO European Region countries in reaching their Health 2020 targets, using the core indicators determined in the Health 2020, with MCDM methods. These evaluations were made for two separate time periods based on the data from 2010 and 2019, and the relative performance of the countries in reaching the targets has been compared.
Selected Health 2020 Core Indicators.
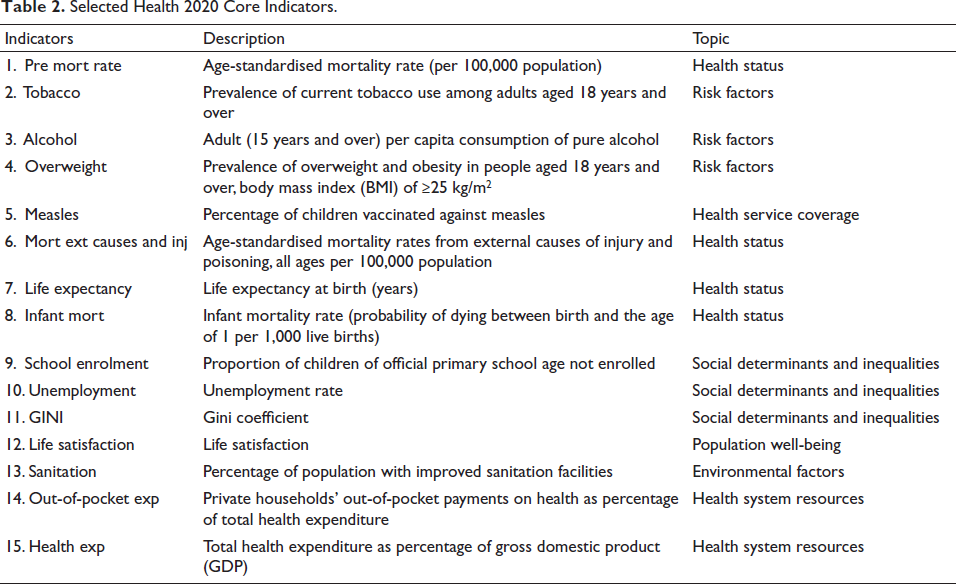
Accordingly, 42 countries whose indicator data in Table 2 were available from 53 countries in the WHO European Region were included in the analysis.
Methods
In this study, the CRITIC method, one of the objective weighting methods, has been used to calculate the weights without the intervention of the decision maker in the weighting of the 15 indicators. In this section, CRITIC, CODAS, EDAS and TOPSIS methods that enable the evaluation and ranking of the alternatives and the Borda Count method for merging the initial rankings to obtain the final ranking are described.
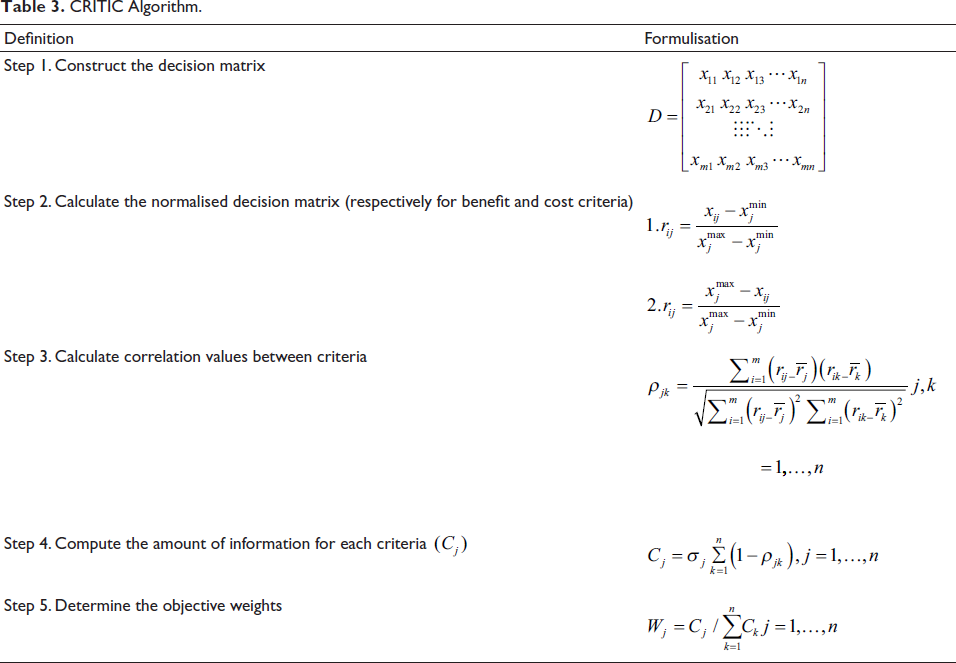
CRITIC Method
CRITIC Algorithm.
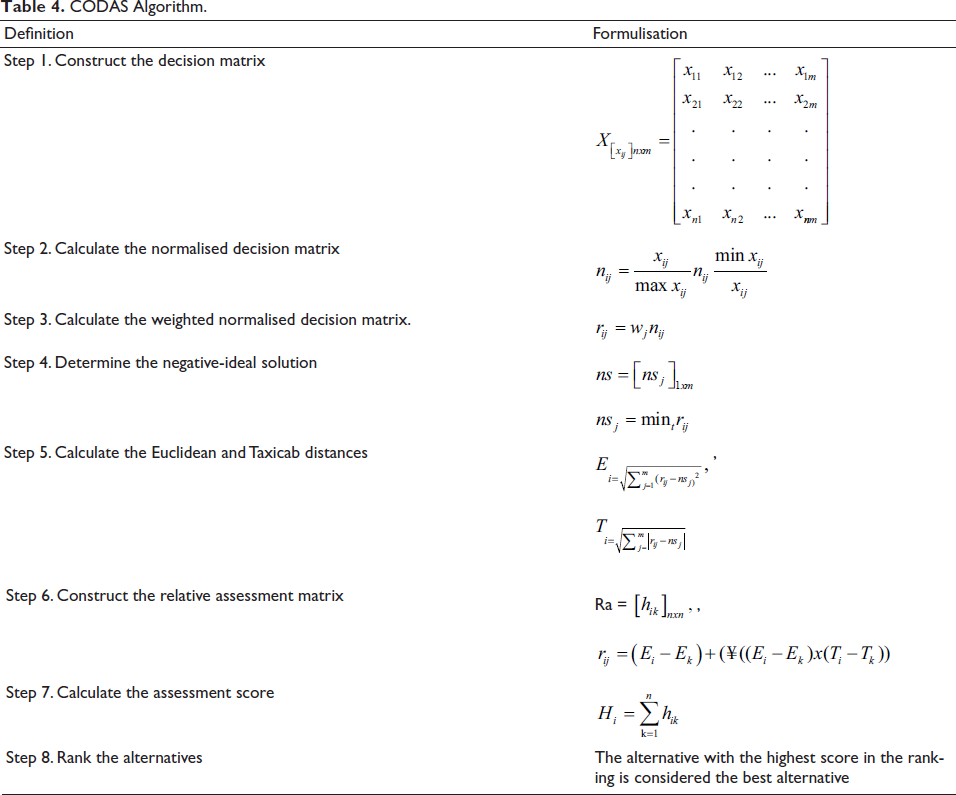
CODAS Method
CODAS Algorithm.
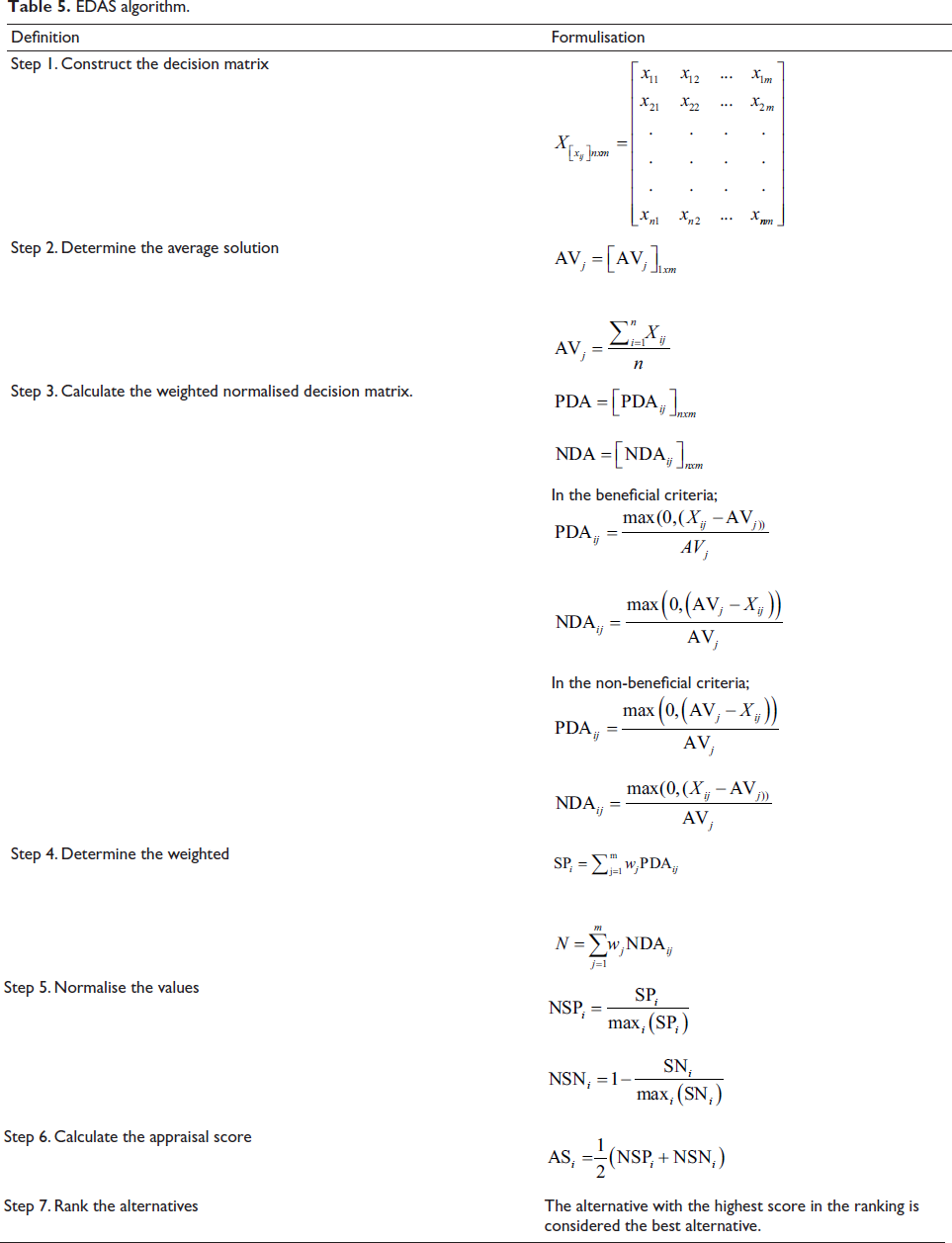
EDAS Method
EDAS algorithm.
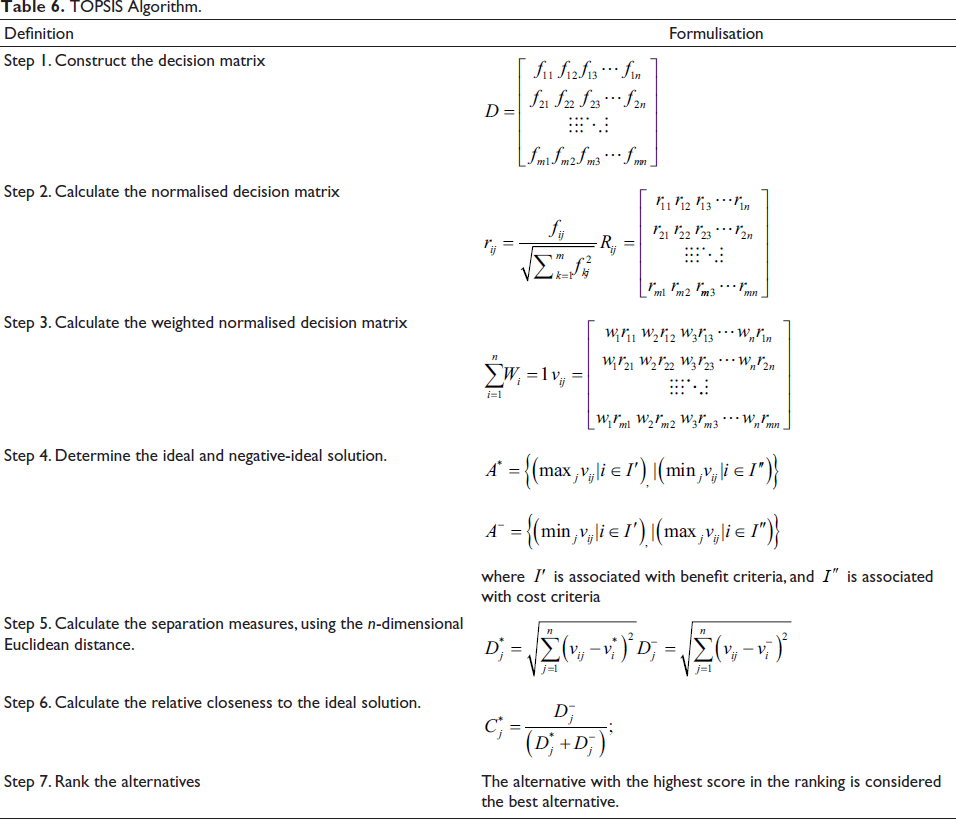
TOPSIS Method
TOPSIS Algorithm.
Borda Count Method
Many MCDM techniques are used together in solving sequencing problems. One of these methods does not have a definite advantage over the other, and generally close results are obtained. Determining the best alternative with these methods is considered an efficiency criterion. The Borda count method is a data integration technique used to combine ordered lists in these cases (Kim et al., 2006). In the Borda count method, each ranking is of equal importance. In this method, zero points are assigned to the least preferred alternative, 1 point for the next alternative and (n − 1) point for the most preferred (n is the number of alternatives). Accordingly, the values assigned for the alternatives in all classes are summed, the total Borda score is calculated and the final ranking is obtained from this score (Wu, 2011).
In order to enhance ranking trustworthiness, this article suggests a hybrid solution based on multiple ranking methods. The proposed solution procedure is shown in Figure 2.
The Proposed Solution Procedure.

Results
CRITIC Weights of Indicators.

According to Table 7, while the indicator with the highest importance was overweight, the indicators with the lowest importance were improved sanitation facilities and out-of-pocket expenditures. The importance weights of indicators obtained by the CRITIC method were used in the CODAS, EDAS and TOPSIS methods, and the performance of 42 countries was evaluated for 2010 and 2019. The method steps for Tables 4–6 were respectively used for this process. Finally, to merge different methods’ rankings, the Borda count methodology was used. Performance rankings for 2010 and 2019 were calculated separately. In this study, since it is aimed to determine the relative improvement levels of the performances of the countries based on the years 2010 and 2019, the change in the rankings by the years is also calculated. The findings obtained as a result of these analyses are shown in Table 8.
Comparison of the Health 2010 and 2019 Rankings.
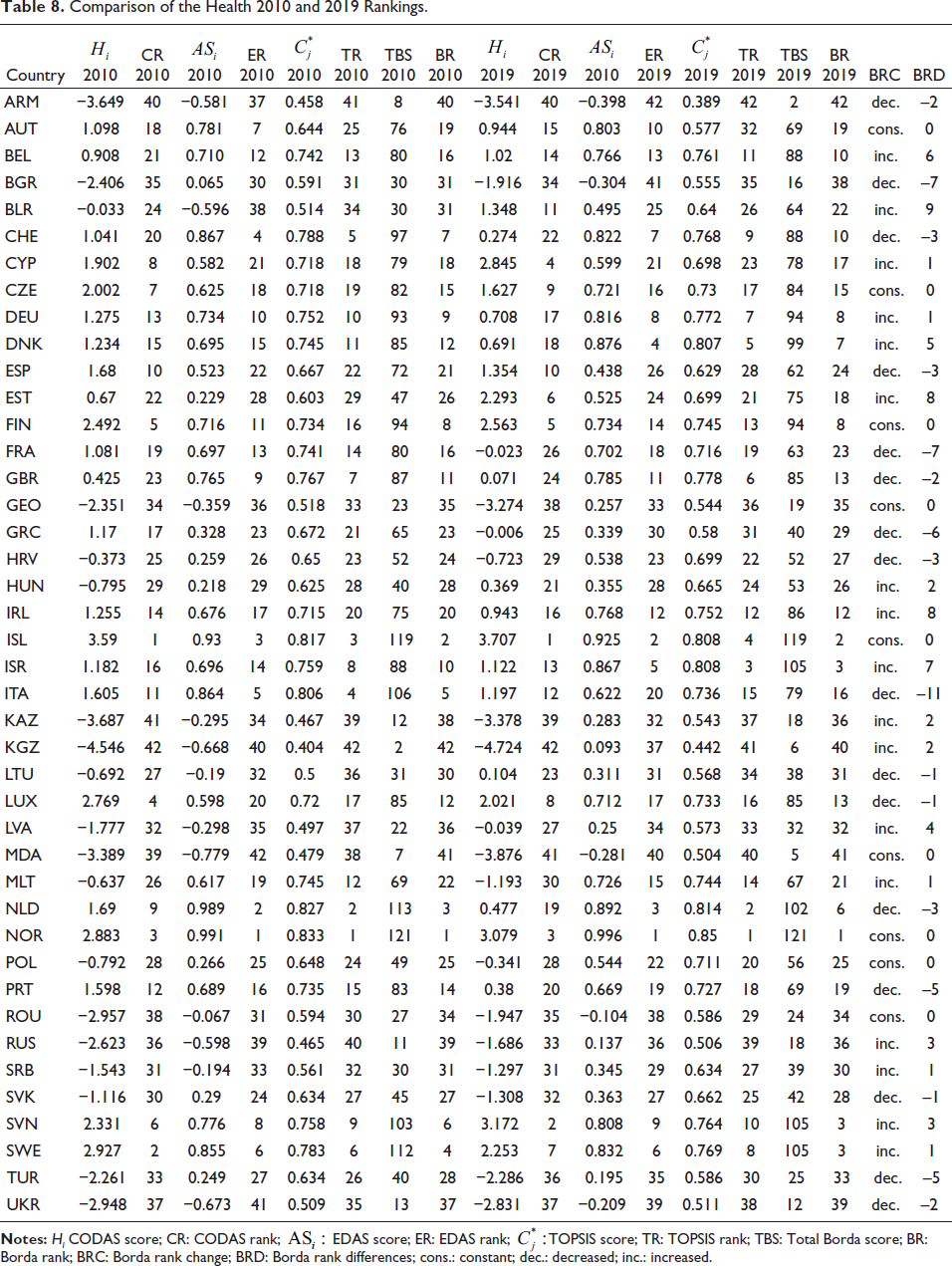
According to the Health 2010 rankings, in the EDAS and TOPSIS methods, the top three countries were Norway, the Netherlands and Iceland, while Sweden was in the top three instead of the Netherlands in the CODAS ranking. Kyrgyzstan was the only country that appeared at the bottom of all three rankings. According to the Borda ranking obtained by combining these three rankings, Norway, Iceland and the Netherlands are in the top three, respectively, while Kyrgyzstan, Moldova and Armenia are at the bottom of the list.
According to the Health 2019 rankings, Norway was the only common country at the top three of EDAS, CODAS and TOPSIS rankings. Moldova and Armenia were the common countries in the last three places according to the three rankings. According to the Borda ranking, respectively, Norway and Iceland are in the top two, similar to the 2010 Borda ranking. Israel, Slovenia and Sweden shared third place with the same Borda score. Finally, the last three countries were Kyrgyzstan, Moldova and Armenia, similar to the 2010 Borda ranking.
According to the CODAS ranking, the countries that fell the most were the Netherlands, Greece and Portugal, respectively, while the countries that rose the most were Estonia, Belarus and Hungary. According to the EDAS ranking, the countries that fell the most were Italy, Bulgaria and Turkey, respectively, while the countries that rose the most were Belarus, Denmark and Israel. According to the TOPSIS ranking, the countries that fell the most were Italy, Bulgaria and France, respectively, while the countries that rose the most were Belarus, Estonia and Ireland. According to the Borda ranking obtained by the combination of these three rankings, the countries that fell the most were Italy, France and Bulgaria, respectively, while the countries that rose the most were Belarus, Estonia and Ireland. According to these four rankings, Belarus is the only country with the highest rise, while Estonia is among the countries with the highest rise in three rankings. Italy and Bulgaria, on the other hand, were among the countries that fell the most according to the three rankings.
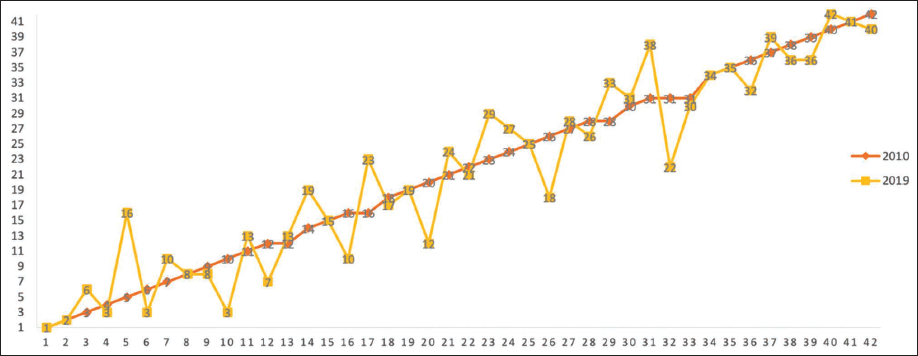
When the indicators that cause this result are examined, indicators 3, 4, 9, 10, 11, 14 and 15 for Italy showed negative changes. For Bulgaria, especially indicators 3, 4, 5, 9 and 11 showed negative changes. Belarus, on the other hand, has achieved a remarkable improvement over the base year, especially in indicators 1, 2, 3, 6, 7, 8, 9, 10, 11 and 14. The 2010 and 2019 Borda ranking changes for the countries are also shown in Figure 3.
The Change in Borda Health 2010 and 2019 Rankings.
Discussion
In recent years, important developments in health and well-being have been recorded throughout the world, but the inequalities among countries make health, social and economic challenges inevitable. The Health 2020 policy framework addresses these challenges by developing leadership that engages governments in achieving the goal of health for all. This study aims to obtain an empirical finding for the policy framework determined by the WHO. For this purpose, the relative level of achievement of 42 countries was evaluated by taking into account the indicators determined by the WHO European Region within the scope of the Health 2020 targets. In this context, it is important to emphasise that the results of the research are limited to the countries covered, as the assessment of the level of achievement is made on the basis of the countries included in the analysis. In addition, since the methodologies of the MCDM techniques used in the research are decisive in determining the level of achievement, it should be taken into account that the research results are limited to the methodology of the methods used. Accordingly, in the Borda ranking, which combines the rankings obtained by three different methods, Norway and Iceland were the countries in the best condition in 2 separate years. Armenia, Moldova and Kyrgyzstan, on the other hand, failed to make any progress in either period and remained the countries with the worst conditions.
Another aim of the study is to compare the ranking changes of the countries of the WHO European Region. In this context, as a result of the analysis, Belarus, Estonia and Ireland were the countries that showed the best progress. It is possible to say that Belarus and Estonia are below average in terms of many indicators, especially in the year they progressed. Although these countries have values below the average, it is clear that they have made significant improvements compared to the initial year. According to the ranking changes, the worst performing countries are Italy, Bulgaria and France. Although Italy and France are in good condition compared to other countries in terms of many indicators, it can be interpreted that they did not achieve the desired progress according to the base year. Bulgaria, on the other hand, was one of the worst-performing countries in both years, in regard to baseline and change.
Özsarı and Boz (2019) analysed the performance of countries with indicators in both health status and macroeconomics. The country performances were ranked separately from the analysis of the indicators. Ireland ranked first in the ranking obtained by the TOPSIS method using macroeconomic indicators. It was followed by Luxembourg, Switzerland, Norway and the Netherlands. Japan ranked first in the analysis obtained by the TOPSIS method, where health status indicators were used. Finland, Sweden, Iceland and France were followed by Japan. In this study, indicators such as macroeconomic, health status and health risk indicators were analysed together in accordance with the framework determined by the WHO. Yılmaz and Söyük (2020) aimed to classify the member countries of the World Bank according to health risk factors and to rank the countries according to health status indicators. Mean weight, CRITIC, TOPSIS and EDAS methods were used for ranking in the study. At the end of the study, countries were classified and ranked to achieve homogeneity. The ranking was obtained by using different weighting methods among homogeneous groups. Norway ranked first in the Borda count ranking obtained using the mean weight. This country has been followed by Australia, Luxembourg, Sweden, Japan and Switzerland, respectively. Kyrgyzstan ranked 76th, Moldova 68th, Armenia 64th, Russia 57th and Kazakhstan 58th in the cluster of 84 countries. The difference of this study in this respect is that it is an empirical study for a specific region for the WHO European Region countries, without the need for cluster analysis to ensure homogeneity in cross-country comparisons. In the meantime, this study includes the ranking changes of countries on a yearly basis. In this study, Norway ranked first in the evaluations for 2010 and 2019. In addition, the ranking of Kazakhstan, Russia, Armenia, Moldova and Kyrgyzstan, which are in the last, shows similarity in both studies. Zuidberg et al. (2020) aimed to analyse the progress of 50 member countries in the WHO European Region according to the Health 2020 indicators between 2005, 2010 and 2015. In the study, an index called the Health 2020 Index was obtained. The ranking was determined according to this index score. The top five countries in the ranking were Sweden, Norway, Iceland, Switzerland and the Netherlands, respectively. The last five countries were shared by Turkmenistan, Georgia, Ukraine, Russia and Bulgaria. Kyrgyzstan ranked 21st, Moldova 44th, Armenia 41st and Russia 47th among 50 countries. Although some of the results are similar on the basis of country rankings, this study summarises many different methods, comparing the findings and showing how the countries progressed in reaching the determined targets by monitoring the changes in the rankings with more actual data.
Conclusion
Since the scope of the research includes relatively homogeneous countries located in a specific region, the findings obtained by cross-country comparisons are important. For decision makers and policymakers in the countries included in the analysis, cross-country comparisons can be used as a basis for appropriate policy development. The active involvement of governments at all levels, international, national and local, is required in tackling these health challenges. In this respect, it is important for countries to provide various improvements with action plans and control programmes for issues such as a tobacco control programme, an alcohol policy, an obesity policy, a vaccination programme, a health insurance scheme, and to periodically evaluate their current situation in terms of indicators determined under the leadership of WHO. It should be designed by considering all dimensions, such as intrasectoral, inter-sectoral and multisectoral dimensions. It is important for the countries of the WHO European Region to cooperate in order to achieve better health and well-being by developing appropriate policies.
In future studies, different methods can be used to weight the criteria. It can be used for weighing from qualitative and quantitative methods. Different methods can be used for ranking in subsequent studies. In addition, qualitative objectives that are not included in this study can be used in further studies. Also, countries that cannot be included in this study due to a lack of data and data access problems may be included in future studies. It is quite clear that comparative analyses are needed for best practices. For this reason, the analysis of health systems should be studied more comprehensively with different methods and by considering the intrasectoral, inter-sectoral and multi-sectoral dimensions in future studies.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.