
Abstract
Medical doctors in Nigeria have been faced with stiff resistance from other allied health professionals, standing toe-to-toe against them on account of their dominance in leadership in the health sector. Therefore, this study will be tailored towards (a) identifying the conflict in the Nigerian health sector leadership, (b) critically analysing the prerequisite of leadership, both in the hospital and in any health authority, and (c) discussing how the findings can be applicable to the Nigerian context, whilst giving recommendations on bringing a lasting solution to the healthcare leadership of the country. The effectiveness of the doctor versus the non-doctor leadership in health is debated, and it is concluded that a trained manager is the best fit to head the hospital and health authority. A framework is developed to map out a thorough process that will engineer the build-up of a leader specifically in healthcare, which is a stepladder mechanism that marries academic and professional competencies through some eligibility requirements that will qualify a person to be a leader in the hospital or local government health department, then a commissioner of health in a region and then the Minister of Health, the stepladder mechanism. This then should not only be implemented in Nigeria but may also be adopted by any low- and middle-income country to improve their health leadership effectiveness.
Keywords
Introduction
The decentralised healthcare system in Nigeria means that the health sector is in three divisions. The Federal Ministry of Health (FMOH) at the national level, which is the policymaking body, coordinating and supervising the activities at all levels whilst sustaining the provision of tertiary health services; the State Ministry of Health (SMOH), which is primarily responsible for the provision of secondary health services. And the local government health department (LGHD), which is responsible for the provision of primary healthcare at the rural level (World Bank, 2010). Apart from the LGHD, all hospital administrators, the Minister of Health at the FMOH level and states’ commissioners of health at the SMOH level have been predominantly ‘medical doctors’. This study, hence, will critically evaluate this issue of leadership, but beyond the scope of fairness and justice, as technical appropriateness and technocratic compatibility of whether the doctor is a better leader in the health sector than a trained manager, even if this manager is an allied health professional. Appropriate recommendations will then be adopted from the critical analysis.
Brief Background
The conflict between the doctors under the auspices of the Nigerian Medical Association (NMA) and the other health professionals under the umbrella body of the Joint Health Sector Union (JOHESU) is centrally placed on the struggle for supremacy in healthcare. The controversial issues surrounding this crisis are as follows: (a) the harmonisation of salaries with that of the doctors, using a single scale, (b) to also carry the title ‘consultants’ just like the doctors, and (c) leadership in health, which is not limited to the appointment of the Chief Medical Director of Public Health facilities and the Minister of Health, but also the Chairman of the Medical Advisory Committee in public hospitals and the commissioners of health in State Ministries of Health as well (Alubo & Hunduh, 2017). The eventual animosity created has reached boiling point to the degree where the unions of different non-physician health workers, including Nigerian Union of Allied Health Professionals; Non-Academic Staff Union; Nigerian Union of Nurses and Midwives; Senior Staff Association of Hospitals, Research Institutes and Associated Institutions; and Medical and Health Workers Union, all came together to draw collective strength to fight the doctors by forming the JOHESUs (Ogunbekun et al., 1999). This study will focus on the third issue alone, assessing the conflict arising from the leadership in the Nigerian health sector by comparing it with other climes as found in the international literature. A critical analysis of doctor-led and non-doctor-led healthcare leadership from the discussion will lead to the development of a framework that will enable a just, transparent, equitable and effective process of having leaders in healthcare in Nigeria.
Discussion
Doctor-led Leadership
The Doctors Over Other Health Professionals
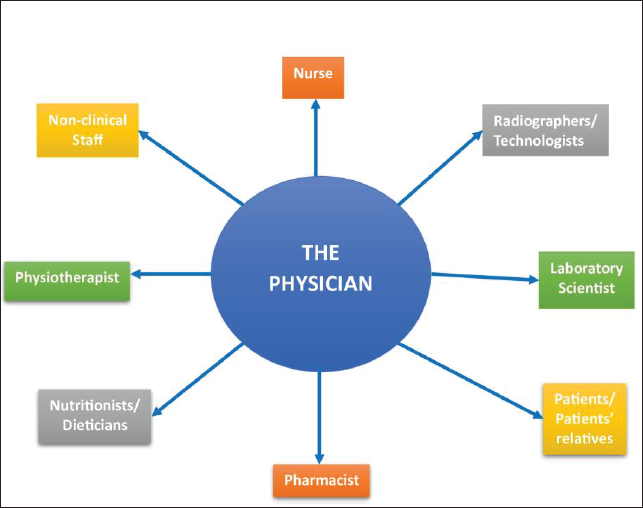
First, the doctor-leaders are better able to interact with other cadres than any other profession. No one relates to other health professionals more than the doctor. A nurse and a physiotherapist or a nutritionist and a pharmacist, for instance, can spend long periods without professionally having contact, but this is not the case with the doctor, as any patient who goes to these other professionals must be referred from, or passed through, the physician (Kenny & Adamson, 1992). Figure 1 illustrates the communication link the physician has with other stakeholders of the hospital system, which is more than any form of professional contact between the other health professionals, indicating the already established potential for effective communication with the others and their familiarity with their working environments and a network of tasks involving their expertise.
The Physician’s Contact Links with Stakeholders.
The physician is more robust in training, skills, professional experience and exposure than any other health professional, hence more eligible to manage the health system. Features, such as uniqueness and specificity of tasks performed and being the most accountable profession that can be sued for malpractice and negligence in cases of unsatisfactory treatment outcomes, solidify this claim. More features, such as stringent prerequisites to enter the profession; lengthiest duration of training programmes; possession of unique body of knowledge not acquired by other health professionals; a broad spectrum of knowledge, which covers a good degree of the other health professions, and making the most vital decisions and performing the most vital functions (Hazelton, 1990) also make this claim more credible. By default, doctors have the leadership, analytical and interpersonal skills required to become managers because their training shapes their mentality into taking charge, time management, not second-guessing, high motivation, relating with other professionals in the hospital space and deep thinking, especially when faced with emergency and life-threatening cases to solve. All these instinctively bring out the leader in physicians. In addition, they better understand the needs of patients than others, whether clinical or non-clinical. They therefore have the ontological and technical know, that is, how to design and manage health services as true technocrats whilst bringing highly relevant insights and timely and effective decision-making experience to their leadership (Moberly, 2014).
Moreover, a medical consultant in any field of medicine should have had plenty of years of experience, which is not only limited to one-on-one patient management but also some professional development in clinical governance, which develops their participative culture, academic research, quest for quality, the management of local resources, maintained relations with the public, frequent discussions at board level, excellent planning skills and effective assessment schemes (Paris & McKeown, 1999). This already sets the stage for the consultant to build on developing skills, such as risk management, human resource management, the creation of guidelines, healthcare service accreditation, regulatory tasks and audit-consumer feedback (Paris & McKeown, 1999). It is no wonder that experienced physicians with management skills evidently improve the quality of healthcare (Tasi et al., 2019). Another route is for doctors to be intentional in becoming consultants or specialists in public health, venturing into public health residency training after having clinical experience as junior doctors. This training usually takes 5–6 years, in the UK, for example, with a compulsory academic qualification in master’s in Public Health (Faculty of Public Health, n.d.; General Medical Council, 2023).
The Doctor Over Non-medical Managers
As for the non-medical managers, the doctor has an immense advantage over them. The World Health Organization created the framework for the improvement of health leadership competence on two components, that is, management and clinical services. The doctor, who is well-equipped for the latter, can easily go into additional training to fit into the former. The manager, on the other hand, will always be found short in the knowledge and skills for maintaining or improving clinical services, which are more rigorous to attain (Briggs et al., 2012; WHO, 2007). More scholars have stressed on this, affirming that doctor-led leadership in the hospital is a key factor in the success of health services and health improvement initiatives (Imison & Giordano, 2009).
Non-doctor-led Leadership
Management-Knowledge Gap by Doctor-Managers
There is evidence to back the failure of a health system led by medical doctors, which clearly shows their gap in managerial skills. In the 1990s and up until the mid-2000s, hospitals in Turkey were run by a physician-led leadership, and studies showed an abysmal output of hospital inefficiency and substantial waste of both human and financial resources (Sahin & Ozcan, 2000). The most unbelievable of all outcomes is the terrible financial management of the doctor-leadership, characterised by ineffective use of financial resources, inability to achieve debt collection and ineffective cash returns formula (Ozgulbas & Kisa, 2006). These staggering findings triggered more research to get to the root cause, and more findings show the physicians’ stretched capabilities to balance clinical roles, reaching roles, research responsibilities and management duties resulting to conflict in their roles, poor communication, immense stress, the lack of empirical methodology in executing highly technical tasks, exorbitant cost of management, poor service delivery and productivity, poor resource management and complicated strategy designs (Degeling et al., 2003). This here is evident that management is a full-time job and particularly in low- and middle-income countries, which will need rigorous training and massive experience as well. Therefore, any physician who is willing to go into management must give up their clinical roles and fully concentrate on tackling the enormous challenges to be faced (Leatt, 1994). In Europe, especially in Portugal and Sweden, doctor-managers have in the past shown orientation implications of their clinical background in management as they exhibit ‘custodial’ behaviour, protecting their collegial relations and practices more than playing their managerial roles (McGivern et al., 2015).
In countries like the Czech Republic, Hungary, Poland and Turkey, it is compulsory for healthcare managers to have a graduate education in business administration or healthcare management run by tertiary academic institutions in order to improve hospital performance and quality of healthcare delivery (Akbulut et al., 2010; Rechel et al., 2006). Furthermore, on a community and state level, managing the health of the public will need knowledge that encompasses biology, epidemiology, social sciences and environmental studies. A well-coordinated and sophisticated synergy is needed to effectively manage and even improve the health of people, hence a multidisciplinary approach. If a multidisciplinary approach will be needed in the processes of research, policymaking, interventions and training in managing the health of the public, why then should the chair be limited to only one discipline (Taylor & Coyle, 2001)?
Medical doctors in Nigeria are very few and nowhere enough (Okafor, 2009) and even from the few available, many doctors are migrating to greener pastures outside the country (Banke-Thomas, 2018). Having doctor-led managers will mean losing highly skilled professionals from clinical medicine to management. The risk is that clinical inputs are lost in return for a manager who has a general knowledge across the organisation, but cannot be an expert in everything. A great model will be to have a full-time manager who has a clinical lead, comprising professionals still in clinical practice, to advise this manager on clinical matters. This clinical lead will consist of doctors, nurses, pharmacists, laboratory scientists and others. They will help the manager make health management decisions.
Clinical Leadership, Not Just the Doctor-led Leadership, Has Proven Efficient
Having a clinical degree is key to management and leadership in the health sector, and this is where the other health professionals fit in. The leader must not necessarily be a doctor but should have good knowledge of clinical practice. A good number of the developed nations run their health systems under leaderships with ‘clinical degrees’, that is, 58% of such leadership in the UK, 64% in France, 71% in Germany, 74% in the USA and 93% in Sweden. These leaderships are not exclusive to physicians alone but are all-inclusive with other health professionals. The same research also found that only through clinical training will managers better understand care delivery processes and effectively communicate with clinical staff. It also states that clinical training gives managers more credibility to lead. This clinical training is not limited to medical doctors (Carter et al., 2011). Evidently, clinically trained managers improve hospital performance (Goodall, 2011), quality of management and mortality rate outcomes (Vize, 2015). Yet again, this is not limited to physicians or medical doctors.
Recommendations
Both sides of the debate on leadership are highly convincing, and it is difficult to pick which option is better suited for leadership in health, especially in a low- and middle-income country like Nigeria. More of this debate has been adequately elaborated in a similar study by the same authors (Makama et al., 2024). The way forward is to standardise leadership in health by creating a career that is independent but strongly related to both options through developing a framework on which any professional interested in having a career as a leader in health can work. Considering the contextual nature of the problem of leadership in health in Nigeria, which is the already established animosity between doctors and other health professionals, this framework completely excludes all health professionals for now. This is because the antagonism already established will make whoever is the head face resistance from the opposing side. For instance, if a nutritionist, being a member of JOHESU, becomes the Chief Medical Director of a hospital, they, most likely, will still face resistance from doctors who are members of NMA or may want to ‘revenge’ and/or ‘punish’ the doctors for all the years of dominance. This means that though there was a change in leadership, the problem remains.
It is also paramount to strategically inject the very important ‘elite status’ or ‘professional credibility’ and ‘respect’ into the health management profession to curb the issues of insubordination and low self-esteem when faced by health professionals and the clinical knowledge gap. Therefore, this framework will ensure that the health management profession must meet the following criteria: (a) an independent career and not an appendage of medicine or management, as already discussed; (b) the health manager will be a system engineer in the health system as a leader, hence, the need to extensively familiarise with the health system; (c) rigorous training with incredible skill acquisition, both in health sciences and in management, to command the loyalty and commitment of the health personnel that will be overseen by these health managers and (d) a projection of the health management career as a highly skilled occupation and an essential profession.
Academic Qualification
An undergraduate programme in health management should be developed. The aim of this programme will be to harness skills in business, economics, accounting, information technology, global health, management, finance, banking, human resources, computer science, data analysis, entrepreneurship, marketing and research in students to appropriately solve problems of health systems. Using templates from the Department of Business Management, University of Maiduguri, Nigeria (University of Maiduguri, 2015), the postgraduate syllabus of MSc Business Management from Aston University, Birmingham, UK (Aston University, 2023) and Global Health courses’ templates from e-Learning Centre (Global Health, n.d.), following the 6-year undergraduate study syllabus for BSc. Health management has been developed as illustrated in Table 1.
Recommended Courses for the 6-year BSc Health Management Programme.

Note that these courses are recommended as core courses, as other courses deemed fit for the student may be added. Each course shall be assessed independently, in accordance with the policy of the university or department, which should also include final examinations for every semester. Moreover, there are two semesters in an academic year, and so the courses may be arranged in any order and spread across the semesters.
After this 6-year training in health management, the student immediately continues with a 2-year dual postgraduate programme in a master’s in Public Health and Hospital Management. In the case of Nigeria, graduates go for a 1-year compulsory service to the nation. In this case, their posts of primary assignment shall either be a hospital or a SMOH, after which a 3,000-word report shall be written on two challenges encountered in the health institution or organisation during service and their recommended solutions as health managers. This report shall be submitted as a requirement to further postgraduate studies.
The postgraduate study will be a 3-year dual programme of MSc Hospital Management and master’s in Public Health as a combined guideline adopted from the Indian syllabus (Target Study, n.d.); the Nuffield Centre for International Health and Development, Leeds Institute of Health Sciences, University of Leeds (University of Leeds, 2022) and the study by Liang et al. (2013). The aim of this dual-postgraduate programme is to further develop more managerial competencies that are essential in managing a health system, such as evidence-based decision-making; interpersonal skills, communication qualities and relationship management; interventions; knowledge of healthcare environment and the organisation; leadership; leading and managing change; operations, administration and resource management; political awareness; professionalism, public, industrial relations and networking; and self-management and resilience both in the hospital and in the health system, as illustrated in Table 2.
Courses for Each of the Six Semesters Recommended for the Master of Public Health (MPH)/MSc Hospital Management Dual Programme.
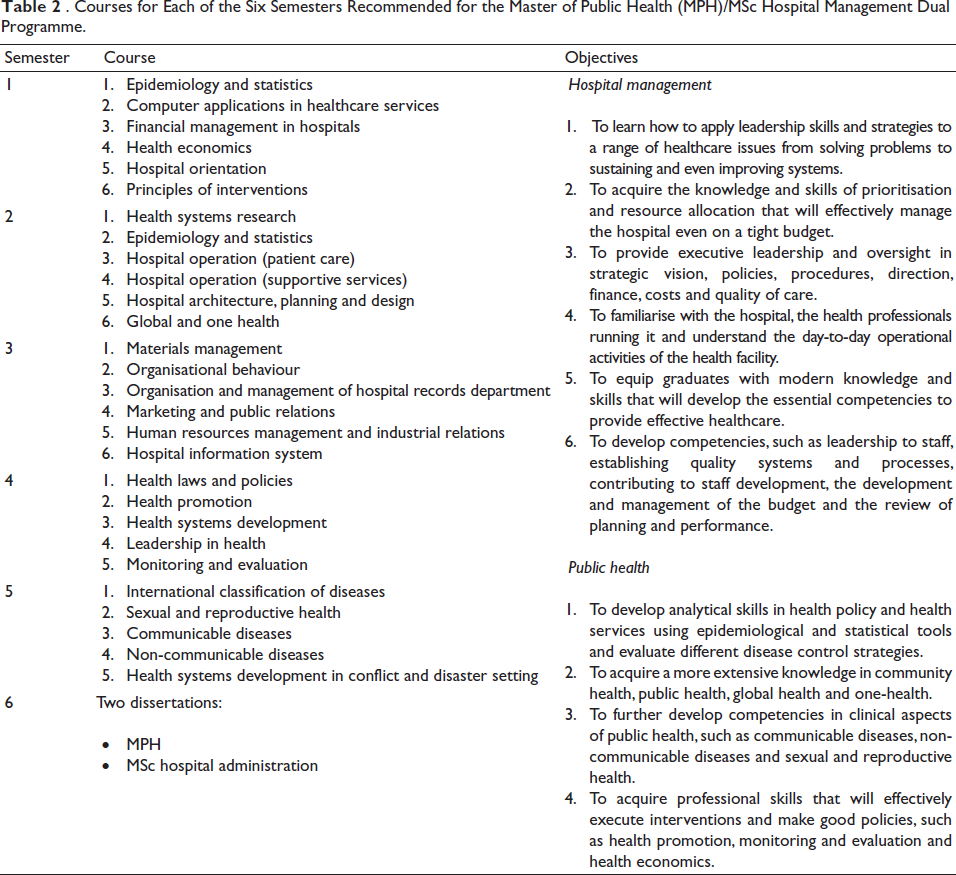
Therefore, the academic qualification to become a health manager is 6 years of undergraduate training in BSc Health Management and 3 years of postgraduate training in Master of Public Health (MPH)/MSc in Hospital Administration. This 6-3 system pathway should be compulsory.
Professional Competence
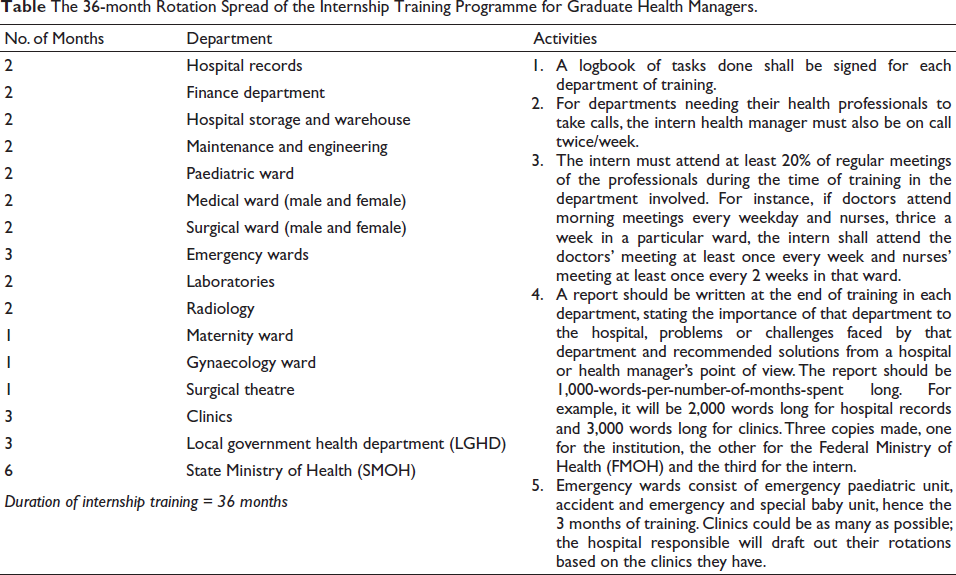
Immediately after academic training, a compulsory 36-month paid internship, done in either a tertiary hospital or ministry of health complex at the regional or federal level, is highly recommended. It should be a paid internship to make both the intern and the institution training for them to get serious about this process. The aim of this internship is to provide the necessary avenue for these 9 years of knowledge and skills to be converted into experience in 3 years. Table 3 summarises the proposed internship training programme of health managers.
The 36-month Rotation Spread of the Internship Training Programme for Graduate Health Managers.
By the end of the 6-3-3 system of training for health managers, as shown in Figure 2, this rigorous process will not only prove effective in building great managers in health but will also give credibility to their credentials, considering the length of time, extensive nature and associated experience and exposures that come with this combined training in management and clinical services. Due to the admission crisis in Nigerian Universities (Kanyip, 2013) and the academic resilience, typical of Nigerian students (Calvin et al., 2022), this 6-3-3 system will not be unattractive to prospective students in Nigeria. Hopefully, this should be the case with any low- and middle-income or even any high-income country adopting this policy.
Health Professional’s Pathway to Becoming Health Managers.
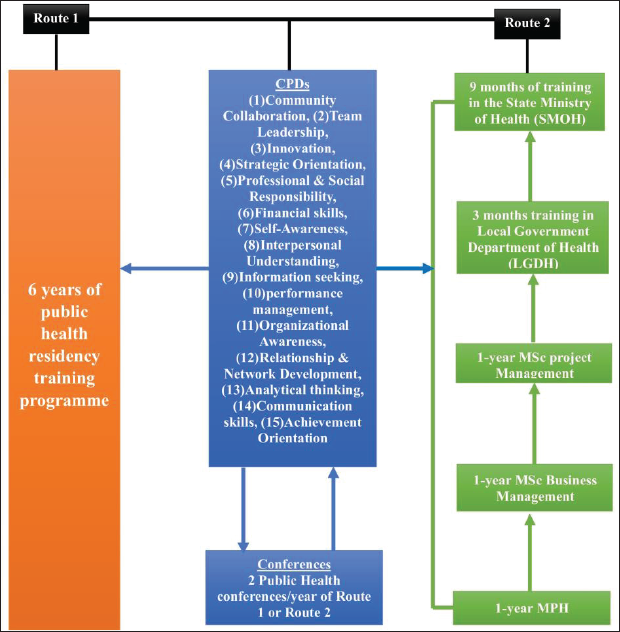
As for health professionals or trained managers who would like to go into management, the two pathways recommended, as shown in Figure 2, are as follows: (a) a 6-year-public-health residency training route that should also absorb an MPH programme, 15 Continuing Professional Development (CPD) programmes illustrated in Figure 2, as adopted from the MSc Health Administration syllabus of the University of Cincinnati (University of Cincinnati, 2023) and at least two public health conferences/year of the 6-year training programme. There will be no need for an internship programme, as all the needed experience and exposure will be acquired during the 6 years of training for health professionals only. (b) A full-time career development in Halth Management, which will include a 1-year MPH programme + 1-year MSc, Business Management programme + 1-year MSc Project Management programme + the completion of 15 CPD programmes, in Figure 2, within this 3-year period + at least two public health conferences/year of the 3-year period of training for both the manager and the health professional. After this, the candidate will be passed fit to go ahead for a 12-month paid internship in the LGHD and SMOH, as illustrated in Figure 2.
A health professional who wishes to use Route 2 will have to give up clinical service to go into full-time career development in health management. The outcome of these two routes is therefore a trained health manager or public health officer and not a physician with health management skills or a manager with skills in clinical services. For now, the Nigerian health professionals should not be allowed to pass through Route 2. After 40 years of the successful implementation of this framework, the FMOH may review this policy to either allow them, or not, if the animosity between health professionals in the hospital has significantly reduced or stopped to an observable degree. Other countries interested in adopting this policy need not apply this restriction, unless they share a similar context with Nigeria, which is the gross animosity between health professionals.
Stepladder Framework
With the academic qualifications and professional competencies well-defined, a pathway to leadership can now be set up, as illustrated in Figure 3. After an internship, the trained health managers can then become managers in local government departments of health (LGDH) for 4 years, of which one LGDH manages several primary healthcare centres in villages and townships under the local government; or the same years of experience in a population-based non-governmental organisation, local or international, but operating in Nigeria. After a minimum of 4 years of practice, they can then move on to head secondary (7 years minimum) or tertiary health facilities (5 years minimum). The next level is to head a department in either SMOH or FMOH for a minimum of 4 years. This then makes them eligible to head the Ministry of Health at Regional Level (SMOH), by becoming commissioners of health. After a minimum of 4 years of this experience, they are eligible to head the FMOH at the national level as the Minister of Health. Figure 3 summarises this approach.
Stepladder Approach to Health Leadership.
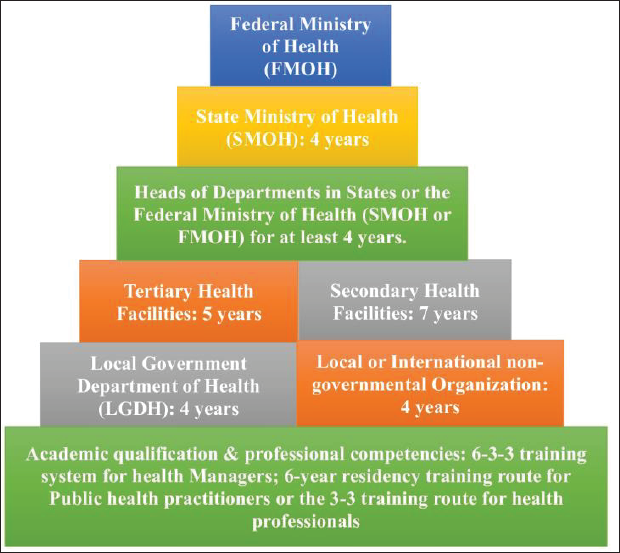
This is called the stepladder approach because a health manager must acquire their academic qualifications and then professional competencies via the internship programme before entering leadership. The second ladder to climb must be to head any of the LGDH or local- or international NGOs for a minimum of 4 years. Only those with this experience are eligible to become leaders in tertiary or secondary health facilities. In the same way, only those with a minimum of 5 years of heading a tertiary health facility or 7 years of heading a secondary health facility are eligible to become heads of departments in either the SMOH or FMOH. A minimum of 4 years of experience as a head of department in the Ministry of Health qualifies the manager to become a commissioner of health in the SMOH of the various states in Nigeria. Also, only those who were commissioners of health for a minimum of 4 years are eligible to become Ministers of Health of the country, Nigeria. In this case, no step can be shunted, en route to becoming the Minister of Health. Therefore, anyone eligible to be a minister must have followed this route of leadership experience, and even if the government is to appoint a commissioner of health (state level) or Minister of Health (national level) based on political partisanship, it will be restricted to a small pool of experienced health managers and in that way, put square pegs in square holes.
Finally, it is highly recommended that in the hospital, the manager will be supported by a board of directors, which will consist of representatives from every health profession in the hospital. That means, for instance, the board of directors will consist of a chief consultant, chief nurse, chief physiotherapist, chief nutritionist, chief pharmacist, chief laboratory scientist, chief radiographer and a non-clinical head (NCH). They will assist in helping the manager make crucial health management decisions, as well as help the manager to bridge the gap between management and front-line staff. With the manager’s knowledge and skill gained from the 36-month internship training, decision-making, deliberations and extensive progressive discussions will be coherent between the manager and these professionals. Therefore, the apex of administration for any other active hospital health worker would be to be a part of the hospital’s ‘board of directors’ or ‘governing council’, depending on how the hospital administration will name it.
Conclusion
To find a lasting solution to the protracted conflicts concerning the health leadership of Nigeria, two sides of the debate between the doctor-led leadership and the non-doctor-led leadership have been analysed. After considering the two sides of the debate, a framework has been created to establish a new career in health management, which is independent of both medicine and management but highly connected to the two disciplines. A 6-3-3 system of training has been recommended, which is 6 years of health management undergraduate studies; 3 years of the dual MPH-MSc Hospital Management programme and a 3-year internship training programme in the various departments in the hospital and the Ministry of Health, all stages being made compulsory. After this training, the newly trained health managers go into a stepladder system of leadership whereby the LGHD is in charge of several primary healthcare centres that are led. Another option at this level is to work in local or international NGOs for a minimum of 4 years. After which, a minimum of 7 years or 5 years of experience in secondary and tertiary healthcare facilities, respectively, is achieved. And then, a 4-year period in a department in either an FMOH or SMOH is headed. A 4-year period of leading an SMOH as a commissioner of health is the next step, and only through this stepladder process will a health manager become the Minister of Health in Nigeria.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.