
Abstract
India requires expanded efforts for reaching the healthcare needs of its vulnerable community. Due to a shortage of qualified health workforce, particularly in rural India, less-skilled health workers are selected and trained to mobilise these efforts. These community health workers (CHWs) are primarily women who work as an interface between the communities and the health system. These workers face several systemic challenges like high workloads, insufficient training and little or no feedback about performance. But apart from these, the CHWs also face several challenges that adversely impact their individual and family health and well-being, disrupting their work–life balance. Performing multiple roles results in strain in the balance, affecting their job and quality of life. The imbalance was noticeable in CHWs playing a pivotal role in fighting the recent pandemic in a less resilient health system. We explore these experiences of imbalance across the Indian sub-continent based on published literature and broadcasted stories from social networking platforms, investigate these work and family stressors and outline the reasons for their occurrence among female CHWs. Some stories revealed inequitable access to COVID-19 prevention kits, gender disparities, unpaid wages and lack of psychosocial support for their mental well-being. At the same time, they negotiate through the structural nuances of the Indian health system. This triple burden of dealing with employment, family and structures during these COVID times has amplified their daily struggles as CHWs and women. The article hypothesises that a balanced work–life interface for CHWs matters for improved organisational performance, gender equality and a better quality of life for their children. We performed a systematic review of CHW-related literature and a thematic analysis of stories from social media and print media from March 2020 to March 2021. The research findings attempt to inform the organisation policies responsible for ensuring that their employees are treated fairly and provided with their employment rights. The Indian public health system that supports these CHWs need to engage in ethical work practices that are legal, fair and ensure decent treatment of the workforce by providing conditions that do not harm the staff.
Keywords
Introduction
The past decade has witnessed an increased interest in the community health worker (CHWs) programmes at the national level (Schneider et al., 2016). The CHWs are paid or voluntary members from the community who are given basic training in order to improve the health of their communities. They are seen as an essential component that helps in overcoming the shortage of the health workforce at the global level (Maher & Cometto, 2016). However, there has been little discussion on the gendered nature of this programme.
Although no comprehensive data are available for the CHW programme, in most of the countries, it is female-oriented by design (Gilmore & McAuliffe, 2013). The CHWs face various social restrictions which limit their movement and are more vulnerable to criticism when they travel alone at odd hours or are seen speaking to men (van Ginneken et al., 2013). These dynamics of gender are not only seen at the social boundaries but also cut across at the individual, health system and community levels (Raphael et al., 2013). The CHWs act as a bridge to reach the poor and marginalised individuals and communities (Theobald et al., 2015). At the same time, it becomes essential to note that the health systems are not gender-neutral. Within the health system, gender power relations create inequitable access to resources, unequal distribution of labour and role, challenges with social norms, values and decision-making (Morgan et al., 2018).
The Indian health system is no different in its experiences with such inequities and challenges. Indeed, the challenges faced by the female health workforce have been in place since the inception of their profession. Nevertheless, the pandemic of COVID-19 has brought these struggles of health care professionals to surface. Apart from the regular health professionals, nearly 3.5 million female CHWs, comprising of 1 million accredited social health activists (ASHA), 2.6 million Anganwadi workers (AWWs) and the auxiliary nurse midwives (ANMs) have been leading the crusade against the pandemic in India since March 2020 (Rao & Chowdhary, 2020). During this period, the primary duty of these female health workers has been strengthening the primary health care and outreach programme and engaging with the community—a service lauded and recognised by World Health Organisation (WHO) (Dasgupta, 2021). Among them, ASHAs have been actively involved in connecting marginalised communities to the health care system since 2006. However, several incidents have been reported where their services were—undervalued and underpaid. Despite their protests during the first wave of the pandemic, these exploitations have gone unnoticed by the Indian government. These CHWs were not provided basic safety gears such as masks and sanitisers in the second wave of COVID-19, during which the virus penetrated rural India. This situation remains unchanged from the first wave, which witnessed many protests from this rung of workers. On the contrary to the government assuring them of duty incentives, these promises have not seen the light of the day (Gupta, 2021).
The CHWs are also placed in a socio-cultural and gendered context because of their personal and professional standing. The socially expected gender role restricts their potential to perform their professional role. By tradition, women cannot participate in decision-making processes on matters of the community. This challenges the ability of CHWs to engage in negotiations with the community proactively and undermines their role as health educators and service providers (Saprii et al., 2015), nothing of which changed during COVID-19. Our study aims to provide a pragmatic approach to the issues of one of the CHWs’ groups called ASHAs during COVID-19 in India and suggest solutions for an effective work–life balance.
ASHA Workers in India
In order to improve various health indicators under National Rural Health Mission (NRHM) in India in 2005, one of the critical elements was ‘communitisation’, which meant increasing the ownership of the public health system by the people (Gaitonde et al., 2017). Under one of its interventions for communitisation, ASHA were introduced to connect the marginalised communities to health care. They form the world’s largest community healthcare workforce and have been influential in improving maternal and child health and reducing the communicable disease burden in India (Rao & Chowdary, 2020).
ASHAs act as a bridge between government and people and work ‘for the nation’ in challenging times. Due to the dynamics associated with their job, they are playing multiple roles—of health care facilitators, health activists and service providers—putting their lives at risk (Bisht & Menon, 2020). Not only do ASHAs act as a bridge between the rural and vulnerable population within the health service centres, whereby they are trained and provided with a kit that includes commodities such as condoms, oral contraceptive pills, delivery kits and simple life-saving drugs, but they also create awareness on health and its social determinants. This is influential in mobilising the community towards local health planning and increased utilisation and accountability of the existing health services (Saprii et al., 2015).
Under the guidelines mentioned in NRHM, an ASHA must primarily be a woman resident of the village, married/widowed/divorced, preferably in 25–45 years of age. She should be a literate woman and qualified up to the eighth standard. However, these criteria in education are relaxed in case no suitable candidate is found in the field. One ASHA is responsible for health promotion activities for 1,000 people in the field for which they receive a monthly performance-based incentive (National Rural Health Mission [NRHM], 2013). Their employment, however, replicates patriarchal culture, which put down women’s employment to the perilous and informal dominion of economy, health systems being no different. This low-paid labour puts them at additional risks requiring them to perform duties separate from their designated role. In addition, their social positioning in low socio-economic backgrounds limits their professional role, and they are not able to leave this job for better career opportunities (Steege et al., 2017). Nevertheless, ASHA workers find themselves at the lowest level of hierarchy in the country’s health system.
Methodology
An observational research approach was used to collect videos from social media platforms. The online data collection tools involved no direct contact with any human participants. The videos from digital media platforms detailed the stories of the daily struggles of CHWs as women health workers in the time of COVID-19. Though it was challenging to directly engage with the subjects in this research because of restrictions of movements and complete and partial lockdown in the country, these videos served as vital raw data that recognised their struggles with the country’s health system and the accentuation of these struggles due to their gender. The information used in the current research was present on public platforms: YouTube, Twitter and webpages. Although the information available on social media platforms is identifiable and not private, the information gathering required no direct contact with those who posted it online and did not constitute the research on human subjects (Moreno et al., 2013). Therefore, this observational research met the criteria for exemption from institutional review boards.
Among social media, YouTube is the most common website that publishes content ranging from news to entertainment, with almost 5 billion videos watched every day. The research team used YouTube as a central social media platform to search videos related to the experiences of CHWs in India during the COVID-19 pandemic. Additionally, for a more targeted search, the team also included prominent Twitter handles that regularly shared content related to concerns of CHWs in India and their day-to-day struggles at the institutional and individual levels. A digital media platform for gender journalism was identified during this process since it flashed the underreported stories of women ‘at the intersection of data policy and law’ (Behan Box, 2021). The published stories, podcasts and other videos on the related topics were screened from this platform and included in the data.
The search for CHWs-related media content followed an inductive method, with the initial search using a broader keyword and gradually narrowing it down. Some keyword combinations of CHW and COVID or ANM and COVID or AWW and COVID or ASHA and COVID in India were used. More search operators were also utilised for an in-depth data-mining exercise. The study also aimed to explore whether there was any difference in the government’s approach towards them, even after the earlier protests of ASHA workers for nearly a year. Similar content was searched for the period of the second wave of COVID-19 to capture this data on earlier protests. The search exercise spanned for a year from 1 March 2020 to 31 May 2021. The mentioned period includes the critical phases of lockdown and unlock, which experienced the highest utilisation of the health care workforce in community engagement.
After the media content was collected, the stories were listened to and transcribed. Several stories were in English, while others were in some Indian languages, namely Hindi, Punjabi and Malayalam. The videos in other languages with subtitles were also included in the study. The videos were revisited and rewatched to extract themes emerging out of stories. These emergent themes were then categorised into broader categories of struggles individual level, community level and at levels of health systems. This thematic analysis of the experiences of CHWs was also complemented by reviewing selected literature and media releases in order to bring any new information.
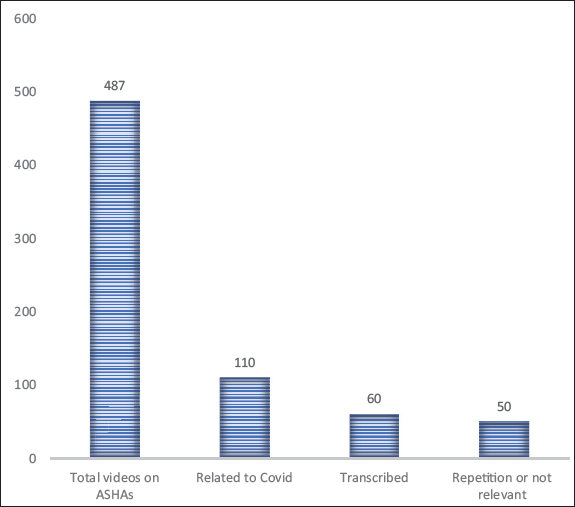
The search was conducted in June 2021. The keyword combinations delivered 110 videos out of 487 videos that were relevant to the research topic. Sixty of these 110 videos were included to collect the raw data, while 13 were excluded as the content was repetitive or too short to make any meaning out of it. Furthermore, seven videos were excluded as they lacked subtitles or transcripts, and the language was either non-comprehendible or the audio unclear. However, after searching these 60 videos, data saturation was achieved as no new themes emerged (Figure 1). As an output for searching for a digital media platform for gender journalism, several gender-sensitive journalism platforms were identified, and their contents were analysed. Behan Box was found as the prominent platform on Twitter that covered the unheard voices of ASHA workers from a gender-sensitive perspective, while the other few platforms were either having a more generalised outlook on the perspective or posted unvaried content.
Search Results for Related YouTube Videos.
Along with their Twitter handle, their web page and Facebook page were utilised to supplement information on the related issues. Emergent themes were collated and analysed for similarities and uniqueness. The various themes were categorised under subheadings which have been described in detail in the next section.
Results
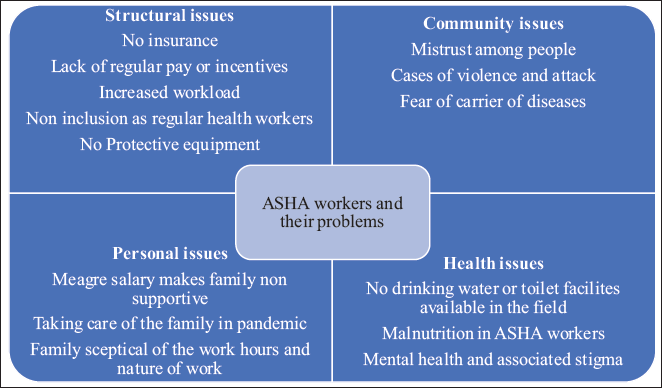
The various issues faced by the ASHA workers during COVID-19 have been classified under four major headings, namely structural, community, personal and health issues (Figure 2). These issues, which were in place even before the pandemic hit the globe, have resurfaced since the state machinery had neglected the voices of ASHA workers earlier. The various issues faced by ASHA workers are interrelated and are a result of their gender placed within a faulty health system. These issues are functional at the intersections of their personal and professional struggles as women health workers. The dominions set up by the social and health system architecture determine their position and placement in the society and health system.
Issues Faced by Accredited Social Health Activists (ASHA) Workers.
Structural Issues
The data analysis data show that ASHA workers felt ignored and alienated by the public health system of the country. As volunteers, the work hours of ASHAs remain flexible, and many ASHA workers prefer this part-time job as it lets them take care of their domestic responsibilities. However, in reality, their work hours extend way beyond the daily 2–3 hours suggested in the ASHA guidelines. During the time of COVID-19, they were reeling under an increased workload where they were spending more than 6 hours in the field. Apart from spreading awareness about COVID-19 and conducting related surveillance and surveys, their work also included keeping records of immunisation, family planning and nutrition. This posed them with a dual burden of carrying out their regular duties along with the duties for COVID-19. While the country shut for regular medical services in the first wave, the ASHA workers relentlessly carried out their regular duties. They were denied proper masks and protective equipment despite making regular appeals to the concerned authorities and officials. In the words of an ASHA worker,
Whenever we used to ask for mask and gloves, they used to say that the supplies are not coming.
1
(Mirror Now, 15.08.2020)
The ASHA workers also complained of non-payment of incentives and lack of regular pay, even during the pandemic period, when their workload increased two- to threefold. There had been pan-India protests by ASHAs in the pre-COVID period on releasing the backlog of their incentives and including them in the category of salaried workers. The delays in payment to ASHA workers during COVID-19 left many worried as their only source of income was this work-related incentive. Although the regular salaries of the other health workers were released, the ASHA workers felt alienated by the state machinery. They also reported that they noticed that the government disowned them despite applauding them for their efforts. In the words of an ASHA worker.
An ASHA worker tested positive she was not given any medicine or help by the government. But when other health workers come positive, they are treated with respect. 2 (Enquirer Today, 1.06.2021)
Community Issues
Apart from the health system failing to retain the workers at the forefront in this pandemic, the mistrust of the community towards the health system was also challenging for ASHA workers. In the initial period of the pandemic, the community members targeted ASHA workers for being the agents of the government. They were also accused of being the spreaders of infection since they spent considerable amount of time in the field for surveillance. Since the mobility of women workers is often a contested terrain, it gets defined and controlled as per social norms. Therefore, the mobile nature of the work of ASHAs constrained them in their social outreach. This patriarchal nature of the society acted as a significant structural force influencing power relations, thus creating a power imbalance, begetting violence towards them in the field. The ASHA workers were of the view that their contributions have been taken for granted by the community, an outcome of the social understanding of women’s labour and its invisible status. Since they were entrusted with conducting community surveillance, ASHA workers faced increased resistance from communities due to fear, mistrust, poor communication and the mobile nature of the work. They were seen as carriers of disease due to their work environment, and it became increasingly difficult for them to engage with dialogue with community members on COVID-19 and its spread.
Personal Issues
The data obtained highlight that socially expected gender roles limited the ability of ASHAs to carry out their duties effectively. As a woman, their family expected them to run the household and take care of the children and elderly. ASHAs complained that any failure to comply with the norms of womanhood at home would attract rebuke from her husband or elders. To justify their role as daughters-in-law, they had to serve their in-laws and perform household duties as well as other social obligations. Also, the meagre amount of money they received after strenuous and risky activities during COVID-19 made the families question their job status at the expense of leaving their household duties. In the interviews, they expressed concerns about being away from their families in these challenging times, especially their children. The resentment of no acknowledgement of their work in practice left them fatigued and more demotivated.
In the words of a few ASHA workers,
We have to answer our in-laws and husband now children too; then we have to answer administration. In some homes of ASHA workers, she is the only source of income. (Enquirer Today, 1.06.2021)
2
We have to take care of our children too, even at home we have to take calls. We are also wife, mother and daughter in law. (Enquirer Today, 1.06.2021)
2
Family says what do you get in this much money? You leave household work. You leave your kids and go out. What if anything happens to kids in Corona? (NDTV, n.d.)
3
Health Issues
This study corroborates the already established fact that ASHA workers feel burdened and stressed due to the nature of their job (Bisht & Menon, 2020), which has increased manifold in the current circumstances. The immensity of tasks carried out during COVID has impacted the physical and mental health of ASHA workers. They reported weight loss due to prolonged work hours with no availability of food and water in the field. Also, the fear of infection and the burden of debt that they carried to sustain their livelihoods, aggravated anxiety and stress levels, adversely impacting the mental health of ASHA.
There is a risk. I have my children and my mother with me, and if anything happens to me, they will be affected. (NDTV, n.d.)3
COVID work is unpaid labour for us. In the field, we have no toilet facilities and no water to drink. (Karnataka, Times Now, 29.07.2020) 4
The gender insensitivity of the health system to the labour of ASHA workers was costing these corona warriors their health. Also, there was no support system or counselling available to address the mental health issues of ASHA workers that were exaggerated due to their workload, unstable family support or environment and segregation by the community. The frontline workers who are responsible for taking care of health in the community were ignored by the system of the country.
Discussion
The CHWs are neither a panacea for a weak health system nor a cheap alternative for providing access to healthcare for marginalised communities (Lehmann & Sanders, 2007). In addition, a significant challenge with the CHWs is that their interaction is with the formal health system and community systems in context-specific and complex ways. Although seen as an essential component of the health system, approaching them from a systems perspective limits access to their problems and performance. Notably, the various health gains made in the community depend not only on the role of CHWs but also on the health system and the community itself (Schneider & Lehman, 2016). The issues faced by the ASHA workers during the period of COVID-19 have not been limited to those dealing with the health system as such but with the interaction of the health systems with the external environment, namely social, political and cultural. Understanding the socio-cultural-economic as well as the political context within which these workers function becomes essential for successful health interventions. However, the health systems present limitations and preconditions that limit the functionality and performance of these CHWs (Kok et al., 2015). The ASHA workers have been reporting the various structural or institutional barriers, namely limited supplies, overload of excessive paperwork and inadequate support from a rigid and hierarchical public health system (Sharma et al., 2014) even before the advent of COVID-19 in India.
Studies have shown that the hierarchical social structures and local leaders had a strong influence on the acceptability of CHWs (Prata et al., 2012). This has been experienced by the ASHA workers and seen an accentuation in the time of COVID-19. The CHWs operate within an ecosystem both formal and informal. In some contexts, CHWs like ASHA workers are explicit agents of downward accountability, which means that they are expected to improve the accountability of health systems to the community they serve. However, in other settings, they have an implicit downward accountability function meaning representing the concerns of the community to a local health facility or making the community aware of their rights (Standing & Chowdhury, 2008). Despite being committed to working for the betterment of health indexes in the population, the lack of regular remuneration undermines the morale and commitment to job duties (Schaaf et al., 2020). Studies have shown that CHWs with higher educational qualifications have opportunities for alternative employment and migrate from one job to another (Brown et al., 2006).
As far as India is concerned, till January 2021, as informed by a minister in the Indian Ministry of Health, forty-four ASHA workers had died in India due to COVID-19 (PTI, 2021). However, after the devastating second wave, there has been no update on this number. Not only the family members of ASHA workers been denied compensation for their on-duty deaths, but there is also a lack of data on the actual number of deaths in these frontline workers. With no PPE, gloves or masks, they are treated as disposables. (Madhav & Gurmat, 2021). A survey carried out by Oxfam India in four states of India (Uttar Pradesh, Bihar, Chhattisgarh and Odisha) revealed that only 23% of ASHA workers had received bodysuits. Out of 306 respondents, nearly 29% worked more than 8 hours a day, while 42% worked between 6 and 8 hours a day. Also, 33% of the respondents suffered from violence or discrimination while performing their duties. In a male-dominated health sector, ASHA workers are an example of exploitation by the establishment (Raina, 2020).
Furthermore, the socio-cultural norms and social geography restrict the females’ movement and their interaction with the opposite gender, which have been barriers for them to carry out their work efficiently (Haq & Hafeez, 2009; Mumtaz et al., 2013). Due to uncertainty associated with the spread of COVID-19, ASHA workers had to bear the brunt of the community. Their gender and social standing made them more vulnerable to attacks from the community. In fact, as a female, the ASHA workers are expected to be obedient to in-laws and spouses. They are also required to give priority to their household work and commitments over their professional work. If their spouse and in-laws belong to a relatively better socio-economic status, they are not allowed to go out and work in the community, resulting in fewer incentives for them and low social status (Sharma et al., 2014).
ASHA workers are also a perfect example of how the government devalues the labour of women workers, especially those involved in care work. The continued typecasting of women’s ability to comprehend the feelings of others, especially other women, makes them perfectly suitable to the job profile of community workers. However, in India, there is a refusal to recognise this ‘all women workforce’ as workers providing labour. They are denied minimum wages, leave and other work conditions and termed ‘honorary workers’. It is significant to note that the idea that women’s care and emotional labour does not fall within the boundaries of the ordinary world of markets. The authorities are often evoked to pay these overworked CHWs just an honorarium (Neetha, 2021). Researchers also note that the term voluntary is misleading for work done by female volunteers who often come from low socio-economic backgrounds (Banerjea, 2011). As outliers in the official medical staff hierarchy in the NRHM, they have little negotiating power with staff at primary health centres, hospitals and dispensaries (Rao & Chowdhary, 2020).
Conclusion
Findings attempt to inform the organisation policies responsible for ensuring that ASHA workers are treated fairly and provided with their employment rights. The Indian public health system needs to engage in ethical work practices that are legal, fair and ensure proper treatment of the workforce by providing conditions that do not harm ASHAs. The government should recognise ASHAs as public health workers and should give them at least minimum wages, social security coverage, standard service conditions and safety at work, including protection against violence. The process of policy should be inclusive, and their voices should be included in the process of decision-making. Policy development in health systems does not necessarily pay adequate attention to gender. In addition, policymakers often have inadequate capacity or knowledge about gender and gender inequities, limiting its recognition and inclusion within policy and practice. Importantly, gender relations and roles need to be considered within the health system to address gender inequalities (Morgan et al., 2018). Public acknowledgement and resolution of the gendered nature of the health workforce will be a significant step in ending the struggles of these CHWs. Lastly, the development of support systems for ensuring the physical and mental well-being of ASHAs is the need of the hour for this workforce to function for the better health of the community.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.