
Abstract
The growing number of older individuals with complex needs and chronic illnesses is a major challenge to the health sector. This has led to a transfer of responsibilities from specialist to the primary healthcare sector. The aim of the study was to explore how healthcare professionals experience setting up and operating a municipal acute bed unit (MAU) in primary healthcare. Three focus groups of health professionals were recruited through purposeful sampling in 2019, and the 10 participants came from different professions. The study has a qualitative design with a hermeneutic approach. The findings identified three themes: (a) Strategic planning and coordinated services, (b) collaborative practice and learning and (c) flexible and family-centred care. The healthcare personnel experienced strengthened quality in the health services, improved work processes and increased safety for patients with relevant diagnoses. The interplay between internal and external factors seems to have been a successful innovation in planning and implementing an MAU in a medical facility in Mid-Norway. We assessed that being prepared for challenges is an important part of innovation in health services. The presence of an ‘inherent capital’ to meet unforeseen challenges in the future should be a prerequisite for innovation.
Introduction
The growing number of older individuals with complex needs and chronic illnesses is a major challenge to the international health sector (Benner et al., 2010; Vos et al., 2015; World Health Organization, 2018). This has led to a transfer of responsibilities from the specialist to the primary healthcare sector. In Norway, the Coordination Reform was implemented in 2012 (Forskningsrådet, 2016), which entailed a range of legal, financial, professional and organisational policies (Helse-og omsorgsdepartementet, 2016). It was essentially targeted to transfer some of the responsibility for emergency care to the municipalities, as described in the Health and Care Services Act (Regjeringen, 2011).
The reform involves more qualified healthcare professionals providing emergency care at the municipal level (Hole et al., 2015). Admission to a municipal acute bed unit (MAU) is intended to reduce the need for hospital admissions. It may be considered for a variety of conditions, such as exacerbations of chronic obstructive pulmonary disease or heart failure, or acute conditions like pneumonia or urinary tract infection (Helse- og omsorgsdepartementet, 2016). The target patient group for this study consists of those with known somatic illnesses, mental health issues and substance abuse problems, who urgently require intervention of health services.
A Norwegian study exploring the collaborative practices in implementing MAU found that close collaboration between vocations was necessary for its development (Kvangarsnes et al., 2016). Close collaboration between physicians and nurses has been found to be crucial for ensuring patient safety. Research reflects that trust among professional groups is considered a necessity for providing quality care to the patients (Hole et al., 2015; Vatnøy et al., 2019). Professional environmental culture, supportive leadership and systemic factors seemed to be crucial to success (Vatnøy et al., 2019).
An evaluation by the Norwegian government indicates variation in how different municipalities choose to establish the MAU (Forskningsrådet, 2016; Grimsmo & Løhre, 2014; Helsedirektoratet, 2019; Skinner, 2015). Approximately 70% of the units were organised as intermunicipal services between either two or up to 12 municipalities (Forskningsrådet, 2016; Helsedirektoratet, 2020). Most of the units comprise only a few beds, which are placed in nursing homes, whereas larger units are situated in district medical centres (Helsedirektoratet, 2020). In 2019, the average duration of an admission to a MAU was 2.9 days, and the utilisation of the total bed capacity was only 42% (Helsedirektoratet, 2020). Since the MAU started, the most common diagnoses have been musculoskeletal conditions, airway diseases and general/unspecified ailments, with pain, infection and observation as the main reasons for admission (Helsedirektoratet, 2020). An evaluation shows that admission to an MAU with good access to medical services leads to around 2.5% fewer hospital admissions, especially for patients above 80 years in medical units (Forskningsrådet, 2016).
The Coordination Reform has also been evaluated, and as expected, the complexity of municipal healthcare has increased rapidly, with patients suffering from more severe illnesses and the consequential increasing administration tasks (Glette et al., 2018; Haukelien et al., 2015). The evaluation of the Coordination Reform highlights the fact that there is still more to be done before the goals of better user co-determination, prevention of diseases and sustainable development are achieved. This includes the ability of the municipalities to take responsibility and cooperate between specialist healthcare and primary healthcare services to ensure easier accessibility of their services (Forskningsrådet, 2016; Grimsmo, 2015). A study suggests further preventive measures to avoid hospitalisation among home-dwelling older patients. This also reveals the need for new solutions due to the increase in community care (Naess et al., 2017). Another study showed that collaboration and trust between professionals, involvement on all organisational levels and clear conversation with specialist healthcare were important for innovation (Kvangarsnes et al., 2016).
According to older patients in a randomised controlled trial in England, the services in a community hospital were seen as a better alternative than in a district general hospital. The participants in this study stated that they had a feeling of independence (Green et al., 2005).
An intermediate care unit is similar to an MAU and is a concept that offers alternatives to hospital care for older patients (Melis et al., 2004). Findings from a British study revealed that the patients were satisfied about the home-like atmosphere and the customised care (Regen et al., 2008). Another randomised controlled study that included a selected group of patients concluded that there were more health benefits in getting admitted to community hospitals as compared to general hospitals (Lappegard & Hjortdahl, 2014a). The patients were more satisfied with the care provided in the community hospitals than in general hospitals (Lappegaard & Hjortdahl, 2014b). They enjoyed the quiet and home-like atmosphere and the fact that the facility was in close proximity to their home. Similar findings were reported in post-acute treatment among older patients in community hospitals in England (Small et al., 2009).
Innovation
Innovation can be described as ‘the successful introduction of ideas, perceived as new, into a given social system’ (Bradford & Kent, 1977, p. 128). The use of concept innovation in health services is relatively new (Kvangarsnes et al., 2016), but it is frequently used. For instance, a strategy for innovation was developed in the Central Norway Hospital Trust for the period 2016–2020 (Helse Midt-Norge, 2015). Here, innovation was defined as ‘... development of new products, services or organisational forms that contribute to a strengthened health service, in the form of increased quality, improved work processes, increased safety for patients and employees, and thus, contribute to value creation’ (Helse Midt-Norge, 2015, p. 2). We find this definition appropriate for understanding the concepts used in this study. Although we do not have data that measure added value statistically, we do have data that express healthcare professionals’ assessments of an MAU as an innovation at an organisational and professional level, as well as at a team and an individual level. In the literature, innovation is presented as a consequence of a long process that includes many ‘interrelated innovations’ and changes along the way.
Organisational innovation, often seen as a continuous process, is linked to management and strategic choices. Strategic management can usher in new solutions by redefining and modifying existing structures (Lam, 2005). A combination of internal and external processes seems to be a prerequisite for innovation in organisations. Lam, in their research, highlights the importance of internal and organisational forces such as capacity for learning, values, interests and power to create organisational development and technological change (Lam, 2005).
The aim of the present study was to explore how healthcare professionals experienced setting up and operating an MAU in primary healthcare. Based on Lam’s study (Lam, 2005), we have analysed the empirical data from the patient, team and organisational level. This has served as a reference in the development of topics in the analysis.
Methods
Design
A qualitative design with a hermeneutic approach was chosen to obtain healthcare professionals’ experiences regarding establishing MAU in Mid-Norway (Gadamer, 2004; Howell, 2013). Focus group interviews with healthcare professionals working in emergency inpatient unit were conducted. Taking a hermeneutic approach implies that the text is interpreted with reference to a historical and cultural context. In this study, this context refers to MAUs as a part of the Coordination Reform implemented in Norway from 2012 (Forskningsrådet, 2016).
Participants and Recruitment
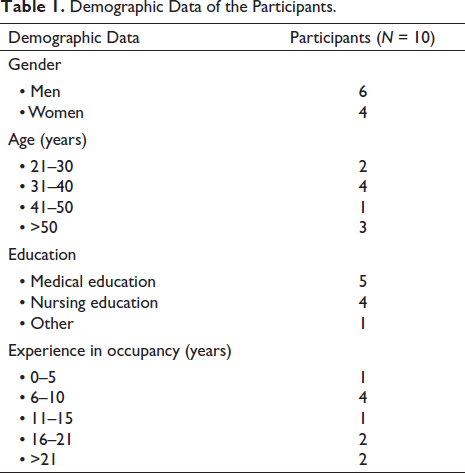
Three focus group interviews with health professionals were conducted in an MAU in Mid-Norway. For this study, participants having an experience of planning and operating an MAU were selected, and a purposive sampling was used. A contact person at the MAU recruited 10 participants who came from different professions (like physicians, registered nurses and leaders). Their experience as personnel in local health services ranged from a few months to more than 20 years (see Table 1). Some of them had experience in both planning and operating the MAU for years, while others had the experience for only a few months.
The MAU selected for this study is located in an urban municipality close to the hospital. It also houses an urgent treatment centre for the city and a nursing home with short-time stays. The participating municipality was part of an inter-municipal collaboration between several municipalities.
Demographic Data of the Participants.
Data Collection
Three focus group interviews were conducted between June and October 2019 (Krueger & Casey, 2015). Their interviews lasted for 90–100 minutes and were conducted in a meeting room in the same building as the worksite of the health personnel. No one besides the participants, the researchers and the observer was present during the interviews. Two of the groups had three participants, and one had four. The interview guide was developed based on earlier research and relevant health political documents. The main themes were experiences of innovation at the organisational, team and the patient level. The interviews were recorded on audiotape and transcribed verbatim. The researchers who conducted the interviews were experienced in focus group methodology. One or two researchers assisted during the interviews and took notes related to interactions in the groups (Krueger & Casey, 2015; Webb & Kevern, 2001). At the end, the interviews were summarised, and the participants were given an opportunity to comment on the content. The field notes were compared between the moderator and the observer accordingly (Krueger & Casey, 2015; Malterud, 2012).
Data Analysis
All the authors read the interviews to get a holistic impression of the data. The historical and social context of the Coordination Reform played a major role during the interpretation (Webb & Kevern, 2001). The data were coded at the organisational, team and patient levels. During analysis, the Mid-Norway Health Trust’s understanding of innovation in health services was also an important reference point (Helse Midt-Norge, 2015, p. 2).
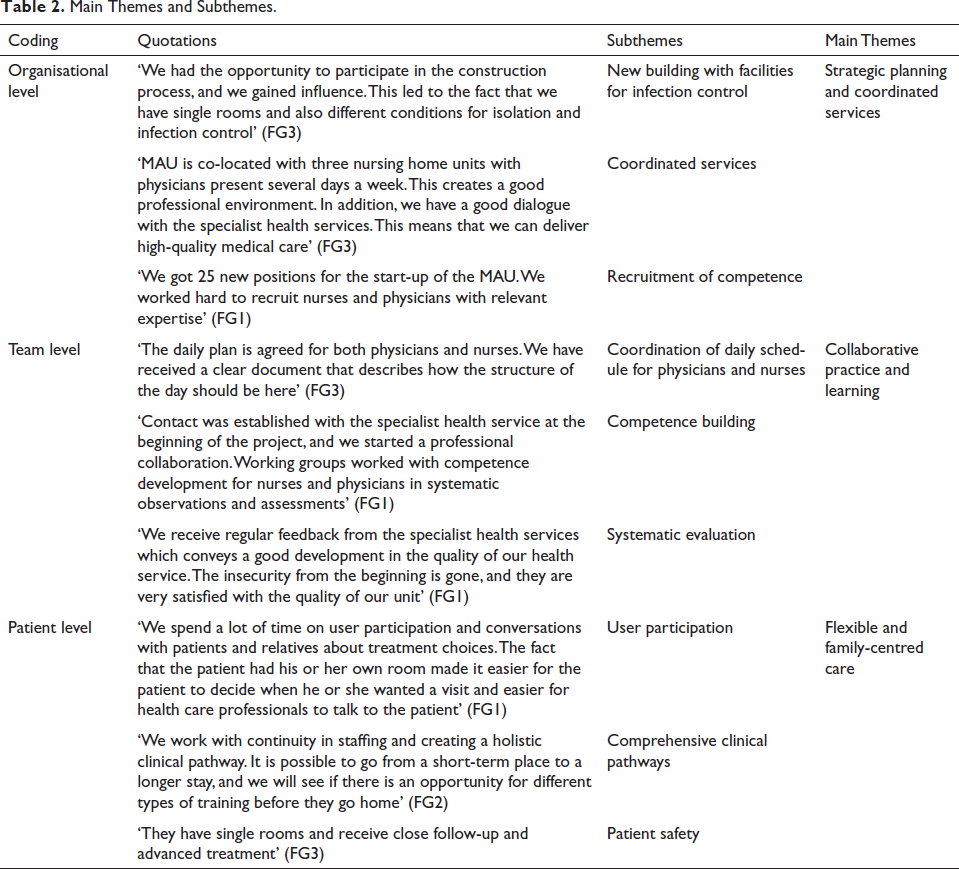
The analysis was both inductive and deductive as the starting point was from the raw data, thereafter abstracting meaningful units to sub-themes and themes. We then checked if all important data were covered by the themes. An alternating process working partially and as whole, and between understanding and pre-understanding, working towards dialogical intersubjectivity was implemented (Malterud, 2012). The researchers cooperated in analysing the data and validated the analyses, which revealed three main themes and several sub-themes presented in Table 2. The quotations represent the findings, as well as the themes.
The analysis was inspired by two hermeneutic circles: The one between the whole and the parts and the one between pre-understanding and understanding. This implies openness to multiple understandings (Howell, 2013).
Main Themes and Subthemes.
Rigor
The research process for this study was carefully planned. Purposive sampling was conducted, and the participants who had the best knowledge about setting up and operating an MAU, and those who were willing to set aside time and were interested in sharing their knowledge for this study, were chosen. The method is well described and is in accordance with the COREQ list (Tong et al., 2007). Saturation was assessed, and data were gathered until each category was rich and thick, and until data was replicated. This provided the researchers certainty and confidence about the strength of the analyses and validity of the conclusion (Morse & Richards, 2002, p. 174).
The theoretical framework about innovation is explicitly described in the background so that the reader can assess the credibility of the presentation. This will make it easier to assess the interpretation of the findings.
Findings
In the focus groups, health and administrative personnel expressed their experiences of innovation at the organisational, team and the patient levels in primary care in the MAU. Three themes were identified: (a) strategic planning and coordinated services, (b) collaborative practice and learning and (c) flexible and family-centred care.
Strategic Planning and Coordinated Services
A project group consisting of the municipal chief physician, physicians, nurses and administrative manager thoroughly planned for a year before opening the unit in 2016. A project management program was established where goals and a timeline of when various measures should be implemented were drawn up. This was followed till the launch of the MAU. The municipality had financed a new building, and the unit was planned to be co-located with the urgent treatment centre and nursing home units with short-term stays.
In the focus groups, the informants talked about early and advantageous collaboration with the specialist healthcare service. This meant that they received help to facilitate advanced treatment. The health personnel mentioned that it had taken some time to develop a common understanding with other health services in the municipality about how the clinical pathway was meant to be and the role that MAU should have.
At first, the feedback was a bit varied, but this changed. They now experienced that they received good evaluation from partners, colleagues, patients and relatives. The work environment was described as good, and they worked with stable and committed employees. Co-location with the urgent treatment centre and the nursing home units also provided good preconditions for coordinated services.
It was also expressed that those in the planning process of the MAU worked intensely to get new positions in place, which ensured access to doctors and covered areas of competence that they needed, among other things. Nurses with advanced clinical training and various medical specialists were considered important in addition to general practitioners.
Collaborative Practice and Learning
The focus groups talked about close and good cooperation between physicians and nurses in the planning and operational phases. The agenda for the nurses and physicians had been coordinated, comprising both joint meetings and time for the physicians and nurses to work on their profession-specific tasks. This coordination contributed to a good flow of work. The health personnel expressed that the establishment of the unit had strengthened the collaboration between the professions. It was also mentioned that a culture characterised by unity and cooperation was developed. Working together with good coordination and cooperation was emphasised, indicating that there was no room for ‘solo players’ in treating patients.
The skills of the health personnel had been continuously developed according to systematic observation and assessment of patients. They had developed courses offered to other units and collaborating institutions, which was seen as part of the work on patient safety. This was a point emphasised in the focus groups. A regular course for physicians and nurses was considered important for developing a common frame of reference in communication and collaboration about patients.
The health personnel considered it important to continuously evaluate their own work. They informed about regular inter-professional meetings and doctors’ meetings, where they evaluated their own work, both internally and externally. Efforts were made to improve routines and the quality of services. In the beginning, the new health service was met with some scepticism, mainly from general practitioners and the specialist health service. However, it gradually disappeared, and the utilisation of the beds was one of the highest in the country in 2019. The health personnel appreciated the collaboration with the specialist health service through planned meetings. The regular meetings with the specialist health service were considered valuable for the MAU’s progress in accordance with future needs for coordinated services and holistic clinical pathways.
Flexible and Family-Centred Care
The interviewees conveyed that a new building where the patients had single rooms provided good framework conditions for delivering patient-centred treatment and ensuring user participation. Respect, equality and trust were emphasised as important elements in individualised treatment.
The implementation of systematic work to facilitate holistic clinical pathways was also discussed. Rehabilitation in the nursing home unit was another example of facilitating comprehensive clinical pathways. Close collaboration with patients, relatives and health personnel in the municipality was considered important for providing a comprehensive clinical pathway.
The health personnel conveyed that especially those with various ailments and repeated admissions found that the service at the MAU was better than in the specialist health service. The health personnel had competence in systematic observation and assessment and good access to monitoring equipment. They had good collaboration with the urgent treatment centre in the same building and the specialist health service at the general hospital close by for diagnostics and treatment. From 2017, they also received patients with intoxication and mental disorders. These patients were admitted for observation in a separate unit that had three observation beds together with the urgent treatment centre. Healthcare professionals saw it as important to shield the intoxicated or agitated patients from other patients.
Those in the focus groups told the researchers how they emphasised on meeting a patient as a person with their own life story and individual needs. Arrangements were made for relatives to be present with the patient during the stay. This contributed to the patient experiencing security in the treatment situation.
Discussion
This study was aimed at investigating how health professionals had experienced the establishment of an MAU as an innovation in primary healthcare. The informants clearly stated that this relatively new health service led to innovation at the organisational, team and patient levels. A professional group spent a long time planning the unit in a new building, where they had a great influence on the design of the MAU. They started a unit with private rooms, good diagnostic and monitoring equipment and good conditions for various types of infection control. In strategic planning, the health services were coordinated, and collaborative practice and learning were implemented. The health personnel conveyed that they provided patient-centred care, strengthening user participation, comprehensive clinical pathways and patient safety.
The organisational structure of the planning process was important for innovation on macro, meso and micro levels. A group of well-qualified health personnel shaped a network when planning, establishing and implementing the MAU. The ability of an organisation to innovate is a prerequisite for successful utilisation of assigned financial resources (Lam, 2005). The planning group established, early in the process, a close cooperation with specialist healthcare services for receiving guidance from them on the challenges of implementing advanced treatment in the MAU.
A collaboration was established on diagnostics and treatment between the MAU, the urgent treatment centre next door and the specialist health services. Cooperation between the MAU and the urgent treatment centre was considered crucial for patients with intoxication or mental disorders. Three observation beds were established for such patients, which allowed their isolation from other patients. An evaluation from 2016 suggested that contacts between the specialist healthcare and the MAU were nearly absent when it came to collaboration and following up with the MAU (Forskningsrådet, 2016). In our study, the informants mentioned that they had regular meetings with the specialist health services. They acknowledged this as crucial for the MAU’s development.
The network was interprofessional and consisted of administrative personnel as well as physicians and nurses. This was in coherence with the Coordination Reform that states that many health and care tasks will at all times lie in the borderland between the municipal and specialist health services and must be solved on the basis of local conditions where necessary professional competence is one of the keys (Norwegian Ministry of Health and Care Services, 2008).
Building competence and collective learning were planned at the organisational level. In our study, the new problem is transition of advanced treatment for patients with somatic or mental illness to the municipalities. The purpose of the MAU is to avoid admissions to the specialist health service when not desirable or necessary, based on a comprehensive medical and psychosocial assessment. The establishment of the MAU for people with mental health and/or substance abuse problems provides a greater opportunity to seek medical interventions earlier and, if possible, avoid the need for admission to the specialist health service (Helse- og omsorgsdepartementet, 2016). Our results showed how the project group planned for collective learning in systematic observation and assessment for nurses and physicians. This led to collective knowledge stored in rules, routines and shared norms on how to handle different treatment challenges. The MAU carried out a systematic evaluation of the ‘community of practice’ (Lave & Wenger, 1991; Wenger, 1998), which means that the members constructed their shared identities and perspectives through their shared experiences to facilitate knowledge sharing and transfer. Collective learning seems to be a prerequisite for maintaining innovation and the quality of the MAU. The healthcare personnel experienced strengthened quality in the health services, improved work processes and increased safety for patients with relevant diagnoses in the MAU. This is in accordance with the Mid-Norway Health Trust’s definition of an innovation that contributes to value creation in primary care (Helse Midt-Norge, 2015).
As per the informants, the MAU located in a new and customised building provided good facilities for individual care, collaboration with relatives and facilitated user participation. This result is in accordance with earlier research, which showed that local municipal hospitals facilitated user participation and patient satisfaction (Green et al., 2005; Hole et al., 2015). Health personnel gained influence in designing the premises that provided conditions for workflow and well-being for patients and relatives. The design of the premises contributes to an efficient functioning of the MAU in the future.
The health personnel highlighted patient safety that was ensured by systematically planning all levels in the MAU to create a safe health service. However, the non-participation of patients in the planning stage can be seen as a weakness.
Conclusion
The interplay between internal and external factors seems to have been a successful innovation in planning and implementing the MAU in a small town in Mid-Norway. The MAU was started keeping in mind the Coordination Reform of 2012. A highly qualified, interprofessional and interdisciplinary project group worked for a long time to plan the unit in detail. They planned the work at organisational, team and patient level, making a great effort to obtain knowledge from similar establishments of MAUs both in Norway and abroad. The thorough planning and collective learning in the collaboration with affiliated institutions led to knowledge creation that facilitated them to meet future challenges. Thus, being prepared for challenges is an important part of an innovation in health services.
It seems that the intention of the Coordination Reform, that the MAU should provide better health services, was largely fulfilled (Helse- og omsorgsdepartementet, 2016; Helsedirektoratet, 2019; Norwegian Ministry of Health and Care Services, 2008). The MAU could offer various options for isolation of patients with serious infections. Thus, they were in a position to meet future epidemics and pandemics.
Footnotes
Acknowledgment
The authors would like to thank the healthcare professionals who participated for sharing their valuable experiences.
Availability of Data and Materials
The data set generated and/or analysed during the current study is not publicly available due to confidentiality. It can be obtained from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Considerations
The study was approved by the Data Protection Officer at Møre og Romsdal Hospital Trust (No 2020/186). Prior to the interviews, the participants received both oral and written information and provided a written consent. They were informed that they could withdraw from the study without providing any reason.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.