
Abstract
Nurses’ job of caring for critically ill patients requires demonstration of behaviour some of which may not be there in their job description. These voluntary behaviours without expectation of reward or favour are referred to as Organisational Citizenship Behaviour (OCB). Patient care is a teamwork, close and cooperative interaction for work within the team and with team leaders, that is, TMX (team-member exchange) and LMX (leader-member exchange), leads to a feeling of commitment known as team commitment and nurses are expected to display OCB to maintain their team membership. Job of nursing imbibes several factors that cause stress to the nurses; these stressors eventually lead to burnout. Stress and burnout harm patient care and particularly on their OCB.
In total, 506 nurses from 5 hospitals of Kolkata participated in the study. Result showed that LMX and TMX significantly relate to OCB and nurses’ role stress negatively relates to the OCB of nurses. Team commitments fully mediate effect of nurses’ role stress on OCB of nurses and partially mediates the relationship between LMX and TMX with OCB. This study may be helpful to Healthcare Managers to devise appropriate strategies to enhance the OCB of nurses. Shortcomings of the study and scope for further research discussed.
Keywords
Introduction
In hospitals, nurses manage the environment of care and spend maximum time with the patients than other health workers. Continuous delivery of care propels them to work on certain tasks that are not within their job description. This is a necessity, as while delivering care to seriously ill patients’ nurses need to undertake actions appropriate to the situation whether or not mentioned in their job role. Extra role behaviour which is also termed as Organisational Citizenship Behaviour (OCB) has been originally referred to as discretionary behaviour of employees that promotes the effective functioning of the organisation without expectation of favour or reward (Organ, 1988).
Nursing is considered a stressful profession. The stress of the nurses arises from the physical, psychological and social environment. Gray-Toft and Anderson (1981) described that nurses’ role stress is generated due to heavy workload, death and dying patients, inadequate preparation to deal with patients’ relations, unpredictable outcome of treatment, lack of support from other staff, and conflict with nurses and physicians. These findings have been supported by different research across the globe including India (e.g., Beh & Loo, 2012; Dasgupta, 2014; McVicar, 2003). Stress serves as a hindrance to extra-role behaviour as nurses need to devote more time to handle the stressful situation and recovering from psychological distress. Continuous exposure to stress leads to burnout which is characterised by emotional exhaustion, depersonalisation and cynicism. The nurse–population ratio in India is 2.1 per thousand population, according to WHO (2019), India is suffering from a shortage of 2 million nurses (Nikore, 2020). Shortage of nurses causes heavy workload for them in Indian hospitals.
Patient care is teamwork and nurses need to work as a team among themselves as well as other persons of the unit engaged in the treatment of the patients. Comfortable exchange with the team members and supervisors in the unit develops a feeling of identification with team members, which evokes their team commitments. Team commitments can be traced from social identity theory (Ashforth & Mael, 1989), which says about the identification of oneself with the group to which one can relate in terms of interest, goal, or other identity. Unit like ICU or inpatient ward is the place where nurses’ work together in collaboration with others and the common interest and goal here is patient care. A collaborative work environment with nurse leaders, colleagues and others of the unit develops positive emotions, which may neutralise the adverse impact of nurses’ role stress on their OCB.
Much of our current knowledge about OCB is based on studies in the West and the Far East. Farh et al. (1997, 2004) in their studies on OCB dimensions in Taiwanese and Chinese samples observed that some of the dimensions differ from that of the West. Ueda and Yoshimura (2011) in their research on Japanese employees observed some differences in dimensions of OCB from that of the study in the West, Taiwan and China. Chiaburu et al. (2015) in their meta-analysis found that culture causes variance in perceived organisational support (POS) and OCB. Though in general POS influence positively OCB, countries ranked high in collectivism, power-distance, uncertainty and feminism (Hofstede, 1980) showed greater influence of POS on OCB than those low in these dimensions.
Glazer and Gyurak (2008) in their study on nurses’ role stress of the USA, UK, Hungary, Israel and Italy reported that nurses of the UK felt poor skill set of staff as a source of stress whereas those of Hungary considered lack of resources as a source of stress. At the same time, nurses of all these countries felt workload, performing certain tasks and types of the patient as a major source of stress (Glazer & Gyurak, 2008). Baba et al. (2013) in their study on nurses’ stress following Job-Demand-Control-Support Model observed that interactive effect of high job demands, high job control and high supervisory support contributed to a lower level of stress in samples taken from China, Japan and Argentina whereas in Caribbean countries additive formulation holds.
On these facts, we may state that since national cultures display various cultural elements in the workplace, drawing a parallel from studies in countries of the West or that of Far-East countries is not appropriate. OCB of Indian employees is the subject of research of several scholars. Mohanty and Rath (2012) demonstrated a significant relationship between Organisational Culture and OCB. Basu et al. (2017) in a sample of Indian health workers observed that OCB significantly predicts job performance, and social capital mediates in the relationship.
The question that needs to be answered is as follows:
How nurses’ role stress relates to OCB? How team commitment is generated due to team member and leader-member exchange (LMX)? How does team commitment mediate in the relationship between nurses’ role stress and OCB? Hardly any study on Indian nurses’ has addressed these issues.
Organisational Citizenship Behaviour
A lot of research has been undertaken on OCB due to its beneficial effects on the organisation. Organ (1988, p. 4) defines OCB as
discretionary individual conduct, not directly or explicitly recognized by the formal system of compensation contributing to the general proper functioning of the organization that does not arise from the prescribed role or tasks of the job, in other words, the specific terms of a contract between employees and organizations; this behaviour arises rather from personal choices, such that its omission is not generally understood as punishable.
OCB develops through the voluntary efforts of employees in which they perform tasks over and above those mentioned in their job description. According to Organ (1990), cooperative and pro-social behaviour by employees is more crucial for certain types of organisations than for others. An example of such activity is ‘treating a patient’ (Organ, 1990). Lee (2001) suggests that though relevant skills of nurses can be standardised, the precise combination and sequence of skills to be used in specific circumstances cannot always be specified in advance, since the performance of a particular type of task depends by and large on situational requirements, that is, changing requirements arising from the conditions of patients (Lee, 2001). Lee (2001) opines that cooperative and voluntary actions instead of standardised rules and procedures are central to the day-to-day nursing operations. Cohen and Kol (2004) are of the view that nurses are expected to display sufficient OCB as they need to take care of patients and perform several jobs that are not within their job description. Altuntas and Baykal’s (2014) reason with their previous research saying that nurses should display high levels of OCB to provide efficient healthcare services. Jafarpanah and Rezaei (2020) observed patient safety culture is highly related to nurses’ OCB.
Nursing Role Stress
Demerouti et al. (2001) explained stressors as external factors that have the potential to exert a negative influence on most people in most situations. They described job demands as those physical, social and organisational aspects of jobs that require physical or mental efforts and are therefore associated with certain physiological and psychological costs (Demerouti et al., 2001). McVicar (2003) opined workload, management style and professional conflict, the emotional cost of caring, lack of reward and shift work serve as stressors for the nurses. Moustaka and Constantinidis (2010) viewed work overload, lack of power, role ambiguity, role conflict, threat to career development and achievement, threat of redundancy and unclear promotion prospects are major causes of nurses’ role stress. Beh and Loo (2012) in a study on nurses in Malaysia reported heavy workload, repetitive work, poor working environment, inequitable management practices, lack of recognition and conflict between different workgroups as stressors. Onasoga et al. (2013) in their study on Nigerian Nurses found handling a large number of patients, lack of incentives for hard work, non-conducive environment, unfriendly relationships with superiors and subordinates, lack of hospital equipment, lack of harmony among staffs and noisy environment serve as stressors for the nurses. Job demands resources theory indicates in the face of high job demands with fewer job resources to cope with the demands people seek some time to relax, which serves as coping resources. In such circumstances, nurses hardly find any time and energy to demonstrate extra-role behaviour or OCB.
It is hypothesised:
HI: Nursing role stress negatively relates to their OCB.
Leader-Member Exchange
The focus of the LMX Theory is the dyadic exchange between the supervisor and subordinates. Deluga (1995) opined LMX can also be understood in terms of social exchange theory and explained that lower quality of exchange is characterised by the exercise of formal organisational authority, whereas high-quality exchange is characterised by a friendly environment and healthy interpersonal relationship. Nurses are professionals (Cohen & Golan, 2007) who need to upgrade their knowledge and nurse leaders of the unit play an effective role in augmenting the practical skills of other nurses. High-quality LMX which encourages a strong dyadic relationship between nurse leader and nurses of the unit motivate these nurses to display greater OCB for retention of a good relationship with the team leader.
It can also be said that high-quality LMX creates a win-win situation for both the supervisor and subordinates as the subordinates get advantages of good performance ratings who in turn reciprocate by delivering better performance and displaying higher OCB. In low-quality LMX relationship operates within the formal structure where subordinates may stick to their official job description and might show no inclination to display OCB. Estiri et al. (2018) found a significant relationship between LMX and OCB:
H2: Positive LMX significantly relates to their organisational Citizenship behaviour.
Team-Member Exchange
Kozlowski et al. (1996) described the nature of a team as comprising of (a) multiple individuals; (b) formed to perform task-related functions; (c) who mutually interact; (d) exhibit task-interdependence; (e) possess one or more shared goals and (f) embedded in a broader organisational setting. Nurses in the ward and specialty units work together in shifts on a rotation basis and provide round-the-clock care to the patients. Considering the nature of work nurses remain interdependent and develop a collaborative relationship with each other working in the ward or other units. Social exchange theory (Blau, 1964) states people form relationships when the exchange is open and is followed by reciprocation. Patient care is interdisciplinary and nurses need to work in a team (Cohen & Golan, 2007). Healthy team-member exchange (TMX) and collaboration among the members of the unit create a safe environment in which nurses prefer to preserve and develop a sense of commitment to the goal of the team and a feeling of belongingness to other team members. All these may prompt the nurses to adhere to the norms of the team and extend helping relationships to each other to perform work, which is not within their job description. Bolino et al. (2015) observed that healthy TMX not only influence citizenship behaviour but also negatively impact the fatigue that may arise out of OCB.
It is hypothesised:
H3: Healthy TMX significantly relates to OCB of nurses.
Team Commitments
Voluntary effort to perform for others’ benefit emanates from a sense of commitment to the surrounding, which may include the organisation, unit of work, occupation and many others related to one-self. Ellemers et al. (1998) described the degree of commitment as the willingness to dedicate oneself to particular goals or values Bishop et al. (2000) equated team commitment with that of organisational commitment. Riketta and Van Dick (2005) in their meta-analysis observed that employees feel more committed to their workgroup than to the organisation as a whole and team commitments predict better performance than organisational commitments. Caricati et al. (2015) explained team commitments lead members, which include a small number of doctors, nurses and others in critical units to feel as if they are committed to the same superordinate goals and accordingly they perform jobs whatever is required for betterment of the unit.
Studies indicate that team commitments significantly relate to OCB (e.g., Mayer & Schoorman, 1992; Organ & Ryan, 1995), whereas some studies (e.g., Afolabi et al., 2009) did not find any relationship between these two in the context of a chemical factory in Nigeria. Afolabi et al. (2009) argued that when team members are in competition with each other and each of them performs only their designated portion of the job. This may not be the scene with nurses as patient care is teamwork and while working in the shift they need to supplement and complement each other’s work. In such a situation, one has to look for a cooperative working relationship and help each other at the time of need. The work team of the respective units starts identifying each other with the team and develops a sense of commitment towards the team and team members. To retain their affiliation with the team members they help each other and perform jobs that are not within the ambit of their work role from the feeling of commitments to other team members.
It is hypothesised:
H4: Team commitments significantly relate to OCB of the nurses.
Researchers like Bentein et al. (2002), Van der Vegt et al. (2003) found team commitments mediate in the relationship between different variables and OCB. Sheng et al. (2010) demonstrated team commitments as a result of perceived team support and trust in the other team members. A sense of trust in other team members serves as a confidence builder for the nurses in a stressful situation, which helps to mitigate the perceived stress. Moreover, trust in the other team members helps nurses to confide in others about the source of stressors, which serves as a coping resource as the feeling of sharing painful incidents to a person with empathy gives some relaxation. Eatough et al. (2011) in their meta-analysis stated that role stressors serve as a hindrance to work achievement as they elicit negative emotions that serve as a detriment to the performance of OCB. Eatough et al. (2011) citing Carlson et al. (1988) argued that positive emotions prompt one to resort to pro-social and cooperative behaviour, whereas negative emotions tend to evoke a lower likelihood of cooperation (De Cremer & Van Hiel, 2006).
Conservation of resources theory (Hobfoll, 1989) states that stress is less likely to occur when one has resources to deal with the stressors. Team commitment which arises as a result of healthy exchange with team leaders and team members serves as a resource in the stressful moments of the nurses and serves as a mediator between nursing role stress and their OCB. Team commitment serves as a sense of identity of the nurses with their team and unit where they are working. As per social identity theory, when people identify them with some group they accept norms of the group as their own (Ashforth & Mael, 1989), become friendly to it, and do not take into consideration difficulties in the environment. Displaying cooperative behaviour to members of the team and witnessing satisfaction among the team members evoke positive emotion, which serves as a deterrent on the negative relationship between nurses’ role stress and their OCB.
It is hypothesised:
H5: Team commitments mediate in the relationship between nurses’ role stress and their OCB.
In units of the hospital’s nurses set and maintain norms under the guidance of nurse leaders. High dyadic relationships in LMX may lead to greater team commitments due to several reasons, first, empowerment of nurses under the guidance of Nurse Leaders leads to a happy feeling among the nurses; second, due to the feeling of empowerment and autonomy under the caring guidance of nurse leader develops acceptance of team norms among the nurses with the view that ‘My Boss’ group is My group’ (van Dick & Schuh, 2010) and third nurses exert greater effort to maintain their membership of the group, which augments the performance of the nurses and also enable them to exert higher OCB. Team commitments also influence the relationship between LMX and OCB from the point of view of social exchange theory as nurses try to pay back the team leader through higher performance and OCB for the healthy dyadic relationship they enjoy with the boss.
It is hypothesised:
H6: Team commitments mediate in the relationship between LMX and OCB of nurses.
High-quality TMX among the team members of the unit develops a sense of belonging and commitment to the team. Commitments to the other team members prompt nurses to take up jobs that are not in the job description but to help other team members. Team commitment develops a form of linkage among the team members in which each of them volunteers to help the other so that the teamwork can be maintained. Effective task-related TMX gets support from team commitments to undertake extra-role behaviour of the nurses as nurses try to maintain their friendships with other members of the team. Li and Thatcher (2015) found that affective commitment towards the team moderates the relationship between trust of the teammates and OCB.
It is hypothesised:
H7: Team commitments mediate in the relationship between TMX and organisational citizenship of nurses.
The mediation effect of team commitments on the relationship between nurses’ role stress and their OCB has usually not been explored. Whereas most of the studies have concentrated on burnout of the nurses and their relation with OCB, nurses’ role stress which is an important cause of burnout of nurses and its influence on OCB needs more exploration as fatigue arising out of citizenship behaviour, which may escalate the process of burnout, can be moderated by the positive contribution provided by organisational support and healthy TMX (Bolino et al., 2015). Hence, the effect of team commitment which may arise from a high dyadic exchange with nurse leaders and the exchange of team members of nurses on the relationship between nursing role stress and OCB needs investigation as these might help the healthcare managers to concentrate on improving team commitments of the nurses.
The study has been undertaken to investigate the relationship between nursing role stress and their OCB and how do team commitments mediate in the relationship? How the LMX and TMX relate to OCB of nurses, team commitments and how do team commitments influence the relationship? The hypothetical model of the relationship is given in Figure 1.
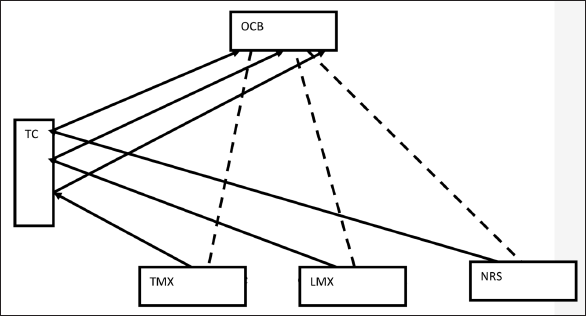
In the model, it has been proposed that healthy LMX and TMX generate both OCB and commitment towards the team. Team commitments in turn influence the process of generation of OCB by LMX and TMX. Nurses’ role stress adversely affects their generation of OCB and team commitments. Team commitments interfere in neutralising the negative impact of role stress in the display of OCB.
This study aims to add the following to the literature:
First, exploration of the negative effect of nurses’ role stress on the OCB of Indian nurses and find how their team commitments mediate on its adverse effects on display of OCB;
Second, team commitments described as a product of healthy LMX and TMX which interfere in the generation of OCB of nurses’ arising out of healthy exchange between leaders and team members is a revelation of the study.
Third, this study aims at providing a comprehensive model aimed at helping healthcare administrators to devise a frame where attempt needs to be made to encourage healthy exchange between leaders and team members in the unit level so that high team commitments may be generated and which would help in evolving and influencing positively OCB of the nurses.
Design and Sample
The study has been conducted among registered nurses in five hospitals of Kolkata after taking permission from the authorities, 550 questionnaires were circulated among the nurses. Care was taken to see that all the nurses were in confirmed employment and none of them were in the supervisory cadre. Considering the fact that the majority of the nurses are female, it was decided to include only female nurses so that no differences arise based on gender.
Ethical Considerations
This study was approved by the appropriate authorities of all the five hospitals of Kolkata where the study was undertaken. Nurses were selected at random from the hospitals keeping in view their age group, years of experience and unit of work. The objectives of the study were explained to them and were assured of confidentiality about their responses. Respondents were given the option of withdrawal in any step of filling the questionnaires if they found it uncomfortable.
Measures
The following instruments were used in the study:
Organisational Citizenship Behaviour
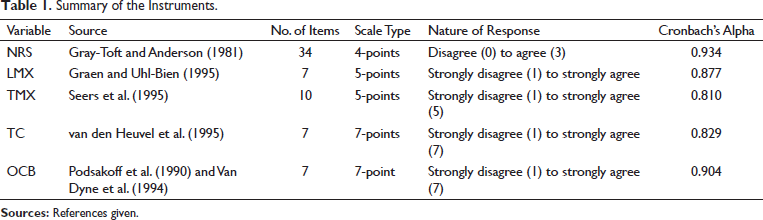
The OCB scale used in this research was developed by Podsakoff et al. (1990) and Van Dyne et al. (1994). The scale is comprised of 7-items, the responses need to be given on a 7-point Likert scale with 6 = always, 5 = very often, 4 = often, 3 = sometimes, 2 = rarely, 1 = almost never and 0 = never. Cronbach’s alpha of the sample has been found as 0.904. Items indicate statements such as ‘I volunteer to do things that are not specified in my job but that help contribute to the organisation’s objective’; ‘Part of my job is to think of better ways of doing my job’. Reliability analysis showed Cronbach’s alpha 0.904.
Nursing Role Stress
The researcher used 34 item Nursing Stress Scale of Gray-Toft and Anderson (1981), the scale comprises of 7 subscales: 6 items for workload, 7 items for death and dying of patients, 3 items for inadequate preparation, 3 items for lack of staff support, 5 items for uncertainty regarding treatment, 5 items for conflict with physicians and 5 items for conflict with other nurses. Each item of the scale describes a stressful situation. The following four response categories were provided for each item: never (0), occasionally (1), frequently (2) and very frequently (3). Some statements are ‘not enough time to provide emotional support to a patient’ indicative of workload; ‘death of a patient with whom you developed a close relationship’—death and dying; ‘being asked a question by a patient for which I do not have a satisfactory answer’—inadequate preparation; ‘lack of an opportunity to talk openly with other unit personnel about problems on the unit’—lack of staff support; ‘criticism by a physician’—conflict with physicians; ‘conflict with a supervisor’ or ‘difficulty in working with particular nurses in the unit’—conflict with other nurses. Since copyright is an issue for this scale, permission was taken from the author for using this scale for academic use. Overall Cronbach’s alpha of the sample has been found as 0.934.
Leader-Member Exchanges (LMX)
The satisfaction of nurses with the quality of their supervisor–subordinate relationship was measured using an adapted 7-item unidimensional scale (LMX-7), developed by Graen and Uhl-Bien (1995). Items are, ‘My supervisor understands my work problems and needs’; ‘I have a good working relationship with my supervisor’ and the like. The reliability analysis demonstrated a high level of internal consistency for the LMX measure with Cronbach’s alpha of 0.877
Team-Member Exchanges (TMX)
A 10-item TMX Quality Scale developed by Seers et al. (1995) was used to measure team members’ perceptions of the reciprocal exchange relationship between themselves and team members. In this measure, a 5-point scale starting from 1 (strongly disagree) to 5 (strongly agree) was used. Some sample items are ‘Other colleagues of my team recognise my potential’; ‘In busy situations, other team members often ask me to help out’. The alpha reliability of the scale was 0.810
Team Commitments
A 7-item scale (Ellemers et al., 1998) was used, it is a 7-point scale (1 = strongly disagree; 7 = strongly agree). Some of the items show feeling ‘I try to invest effort into a good atmosphere in my team’, ‘The team lies close to my heart’. Cronbach’s alpha of the sample found was 0.829. The summary of the measures is given in Table 1.
Summary of the Instruments.
Mediation Analysis
To test the effects of mediating variables, the researcher needs to follow the steps recommended by Baron and Kenny (1986). Baron and Kenny (1986) outlined the following four conditions that must be met to establish mediation:
The independent variable must affect significantly the mediator in the first equation;
The independent variable must affect significantly the dependent variable in the second equation;
The mediator must affect significantly the dependent variable in the third equation;
If these conditions meet, then the effect of the independent variable on the dependent variable must be less in the third equation than in the second.
In the case of perfect mediation, independent variable holds no effect on the dependent variable and mediating variable controls.
Analytic Strategy
This study used SPSS 20 version and Sobel test in the study for analysis of data, p < .05 was treated as statistically significant. SPSS was used to examine the demographic profiles and the relationship between different variables examined through correlation and regression analysis. Sobel test was applied to find whether the product of unstandardised regression coefficients of the regression analysis of independent, mediating and dependent variables are significant.
Results
Participant’s Characteristics
Out of 550 selected respondents, 506 nurses filled up all the questionnaires. These nurses were within the range of 21–31 years with an average age of 24.97. Respondents were within the experience of 1–5 years with an average experience of 2.5 years and half of the nurses were working in critical care, emergency, cath lab, operation theatres and half were from wards. Out of 506 nurses, 323 were diploma in nursing and 183 were graduate and postgraduate in nursing.
Independent sample t-test and ANOVA were conducted to find the differences based on age, experience, place of work and educational qualification of the sample on their OCB, nursing role stress, LMX, TMX and team commitments. The differences are insignificant, that is, no significant difference (p < .05) could be located.
Descriptive Statistics
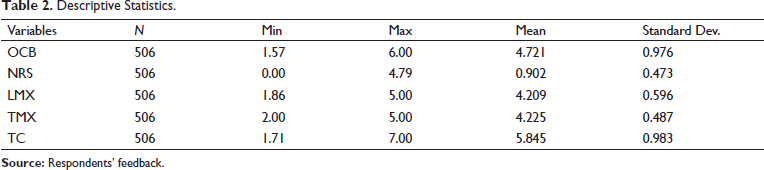
Analysis of the descriptive statistics showed LMX (mean 4.21, SD 0.6; range 1.86 to 5); TMX (mean 4.23, SD 0.49; range 2 to 5); nurses’ role stress (mean .90, SD 0.47; range 0 to 2.79); team commitments (mean 5.85, SD 0.98; range 1.71 to 7); and OCB (mean 4.72, SD 0.98; range 1.57 to 6). All these have been given in Table 2.
Descriptive Statistics.
Relationship of LMX, TMX, Nurses’ Role Stress with OCB and Team Commitments of Nurses
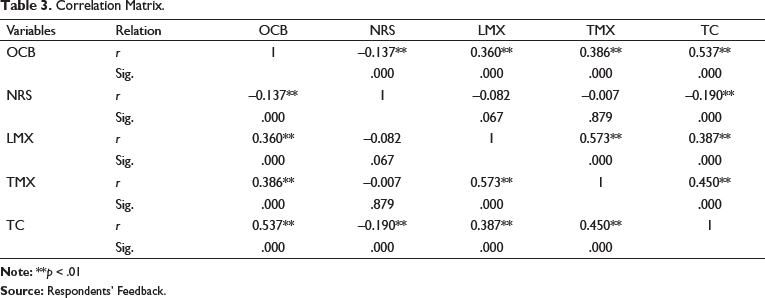
Correlation analysis indicated a significant relationship between LMX and OCB (r 0.360, p < .01); TMX and OCB (r 0.386, p < .01); team commitments and OCB (r 0.537, p < .01); and nurses’ role stress negatively relates to OCB (r –.137, p < .01).
Correlation analysis also showed a significant relationship between LMX and team commitments (r 0.387, p < .01); TMX and team commitments (r 0.450, p < .01); and a negative relationship between nurses’ role stress and team commitments (r –0.190, p < .01). All these have been given in Table 3.
Correlation Matrix.
To further analyse the impact of independent variables on OCB and the effect of mediation of team commitments, linear and multiple regression analyses were undertaken.
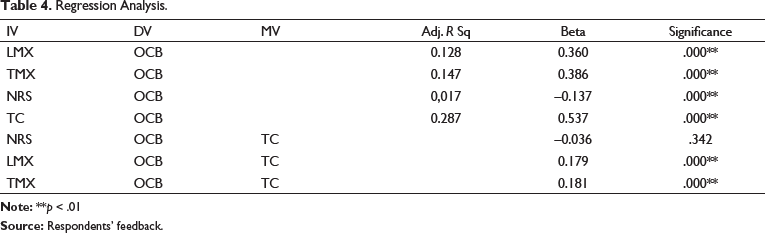
LMX was regressed on OCB and the following results were obtained:
Adjusted R Sq 128, beta 0.360, p < .01 show the significant relationship and LMX impacts OCB of the nurses;
TMX was regressed on OCB, where adjusted R Sq 0.147, beta 0.386, p < .01 show the significant relationship and TMX causes variance on OCB.
NRS was regressed on OCB, where adjusted R Sq 0.017, beta –0.137, p < .01 show a significant negative relationship and NRS negatively affects OCB.
To find out the mediation effect of team commitments on the relationship between NRS, LMX and TMX with OCB, multiple regressions were conducted based on the Principle of Baron and Kenny:
NRS was regressed on team commitments, where adjusted R Sq 0.034, beta –0.190, p < .01 show a negative significant relationship;
Team commitments were regressed on OCB, where adjusted R Sq 0.287, beta 0.537, p < .01 show a significant relationship;
NRS, which showed a negatively significant relationship with OCB, was regressed along with team commitments on OCB result, where beta –0.036, sig. 342, p > .05 show an insignificant relationship between NRS and OCB when intervened by team commitments. The relationship between NRS and OCB, which was negatively significant, has turned to be insignificant when mediated by team commitments; this indicates that team commitments fully mediated the relationship between NRS and OCB. Sobel test was undertaken where (Z = 3.03, p < .01) concluded the mediation result.
LMX was regressed on team commitments, adjusted R Sq 0.148, beta 0.387, p < .01.
LMX, which showed a significant relation with OCB, was regressed with team commitments. Results are beta 0.179, p < .001 and have maintained a significant relationship with OCB, the value of beta reduced from 0.360, p < .001 to 0.179, p < .01, which indicates partial mediation by team commitments. Sobel test result (Z = 7.83, p < .01) supports the mediation analysis.
TMX was regressed on team commitments, adjusted R Sq 0.201, beta 0.450, p < .01.
TMX, which showed a significant relationship with OCB, was regressed on it along with team commitments and showed beta 0.181, p < .01 indicates that the relationship has remained significant though the strength of the relationship reduced from beta 0.386 to 0.181. Sobel test conducted (Z = 8.92, p < .01) confirmed the exercise of mediation. It can be concluded that the relationship between TMX and OCB has been partially mediated by team commitments. All these have been compiled in Table 4.
Regression Analysis.
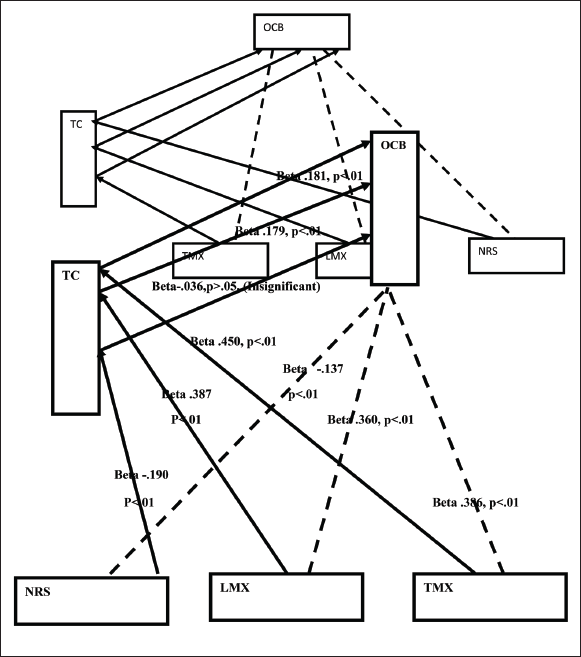
A summary of the tested model is given in Figure 2.
Discussion
This study investigated the effect of nurses’ role stress on their OCB and the mediation effect of team commitments on this effect. It has been found that team commitments fully mediate the influence of nurses’ role stress on the OCB of nurses. Significantly, the stress of the nurses which impacts their extra-role activities can be neutralised by team commitments.
Stress, which is implicit in the role of nurses, is the cause of burnout and burnout influences not only their on-job performance and extra-role behaviour but also their way of looking at the nursing profession and normal conduct. Nursing is listed as one of the most stressful occupations and even many nurses exit the profession due to burnout. This is particularly important as the presence of nurses is a requirement for society for rendering care to the sick and needy, moreover, stress and resultant burnout affects adversely patient care. This study showed that the effect of role stress can be neutralised by team commitments is important for nurse leaders and healthcare managers because if the stress emanating from the role of the nurses gets neutralised due to team commitments and they can display OCB which will benefit the patients. This will also improve nurses’ psychological health and reduce the propensity for burnout and turnover.
A reason that may be attributed to this finding is the collectivistic nature of Indian nurses. In the study of Hofstede (1980), Indian culture has been rated as high on collectivism, according to authors like Khandwalla (1990) based on the Indian value system some family members even forsake good career opportunities in order to stay at home for the sake of ailing parents. Thus, team commitments that arose among the colleagues and immediate supervisors may serve as a cushion between feelings arising out of implicit role stress and OCB of the nurses.
Team commitment, which has been described as arising out of trust between team members due to the positive interactions between the team members and leader of the team, is significantly related to TMX and LMX of the nurses. Comfortable interaction between the team members and leaders and the trusting relationship create an influence on extra-role behaviour of the nurses, in the study since team commitments have been found to partially mediate the relationship between TMX and OCB, LMX and OCB of the nurses. Thus, it has been found in the study that TMX and LMX not only influence in causing team commitments of nurses but also team commitments, in turn, impacts their exchanges in displaying the outward behaviour of OCB.
Another important fact that has evolved from the study is that the finding has been found to be common among the nurses who are not in any supervisory category irrespective of their place of work. Studies indicate that nurses engaged in critical care areas are more stressed, even, nurses working in cardiac ICU reported higher stress than that of surgical ICU (Alharbi & Alshehry, 2019), but no such revelation came up in the study as no significant distinction could be witnessed in the role stress between nurses of the sample, at the same time not between the different age group and years of experience, though it was within an age group of 21–31 years and experience of 1–6 years.
Limitations and Scope for Further Research
A striking observation of the study is the complete mediation on the effect of nursing role Stress on their OCB by team commitments. A point that may be attributed in this regard is the collectivistic nature of Indian Society. This study can be made among nurses in Far-East countries like Japan and Korea which are high in collectivism and also in West European countries and the USA, which are high in individualism to explore whether culture has any role in this phenomenon.
A fact that emanates from the study is that team commitments can neutralise the effect of role stress on nurses’ OCB; research can be extended to find whether it can neutralise the effect of stress on their performance and also on the psychological health of the nurses.
This study considered LMX and TMX as generators of team commitments and have not taken into account nurses’ positive interaction with organisational support mechanism like employee-friendly policies, family support, etc., whereas family support may not have much relevance to the development of team commitments, organisational support may have an impact as units are a part of the whole organisation. This study has taken up purely on informal social transactions like TMX and LMX and has not taken up that with formal structures like organisation as since the feeling of organisational support arises mainly due to formal and designed conduct of the organisation and its management.. However, this point opens up a scope of further study.
This study has been undertaken on self-assessment data received from respondents who are nurses and does not hold any supervisory position. In this context, it can be argued that the inclusion of supervisors’ views on the OCB of nurses of their respective units would have given a more comprehensive result. This argument may stem from the fact that OCB is a displayed behaviour and supervisors being monitoring authority would have been in a better position to narrate so. But, since all other variables are implicit within the self and all these drive OCB, it was necessary to collect it from the same person. This study is cross-sectional; if the study is extended to longitudinal one more interesting results can be obtained.
Conclusion
The study was undertaken to find out how the role stress of the nurses, their TMX, LMX affect nurses’ display of extra-role behaviour, which is essential for the improvement of patient care. This study was also made to explore how commitments to the team of the unit within which nurses function are shaped by their interaction with team members and immediate supervisors and how does their team commitments affect OCB and the stress implicit in the role of the nurses.
The study was undertaken in five private hospitals of Kolkata, and it has been found that both TMX and LMX play a significant role in forming team commitments, which partially mediates their role in delivering OCB. Nursing role stress seems to negatively influence OCB but team commitments through mediation can neutralise their impacts. This study may be useful for nurse leaders and healthcare managers so that they may take initiatives for enhancing team commitments of the nurses, which may help the nurses to display better OCB neutralising their role stress.
Footnotes
Acknowledgement
Author acknowledges with thanks to the management and nurses of hospitals who participated in the study.
Author’s Contribution
This research study is original work of the author who have conducted the study purely because of his academic interest, wherever information available in other sources used it has been referenced in the text.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Disclosure Statement
The author hereby declares that the work is completely his own and no conflict of interest with any person has occurred, author also informs that he has not approached any one for financial support in regard to the study and no one has rendered any financial support for the study.
It is further stated that it is the work of the author and the author himself is responsible in regard to this research study
Funding
The authors received no financial support for the research, authorship and/or publication of this article.