
Abstract
The adolescent period is a time of many upswings and downsides which requires constant support and guidance from parents, guardians and society. Moreover, adolescent girls face more psychosocial problems in contrast to boys, especially in India due to its different social and cultural environment. The psychosocial problems can have an adverse effect on the health of adolescent girls. Thus, social investment in adolescents is important not only for their well-being but also for society as a whole. The Integrated Child Development Services (ICDS) is one of the social investment programmes in India which seeks to address such problems in girls. The present research study has been carried out to explore the psychosocial issues of adolescent girl beneficiaries’ of the ICDS programme in Central Kashmir. Furthermore, the role of demographic and socio-economic factors in relation to psychosocial issues has also been examined. The research was both explorative and descriptive, and the data were analysed with quantitative techniques involving ANOVA in SPSS. The results obtained provide interesting insights into the research problems which can be beneficial for many stakeholders. The study results revealed that most of the beneficiaries had psychosocial issues such as somatic complications, adjustment problems, sleep problems, attention problems and sleep problems. However, these problems varied in relation to different demographic variables such as age, gender, education, district, economic status, etc. The research also provides interesting and valuable suggestions to different stakeholders regarding their role in solving the problems of adolescent girls.
Introduction
Adolescence is a progression from youth to adulthood accompanied by numerous developmental changes which can affect adulthood functioning in the later stages of life (Tayebi et al., 2020). Adolescence is characterised by maximum physiological changes and psychosocial developments (McDade et al., 2011). It is also a phase in which adolescents face many psychosocial issues and problems (Dwivedi & Rastogi, 2019). These psychosocial problems can greatly affect one’s life, one’s work, family and one’s domestic life (Brown, 1987). Those with a psychosocial problem possess several distinct features including disturbances in self-image, inability to have successful interpersonal relationship, inappropriateness of a range of emotions and ways of perceiving themselves, others and the world, and also possess improper impulse control. It has been observed that women face more psychosocial problems now because of their changing roles and dual responsibilities, in both family and outside their homes (Aradhya, 2013). Various psychosocial problems such as anxiety, frustration, mental illness, distress, depression, stress, anger, phobias and various social and emotional distresses are likely to affect the female population. A careful and sensitive investigation into the mind and psyche of women reveals that their fears, anxieties, stress and strains diminish their morale, discourage and also delay their progress and glory (Aradhya, 2013).
A majority of adolescents belong to low- and middle-income nations where they suffer from many adversities such as child labour, abuse, early marriage and pregnancy and poverty (Kieling et al., 2011), which negatively influences their mental health (Green et al., 2010). The global scenario shows that girls are at a higher risk in comparison to their male counterparts for several psychosomatic disorders (Kessler, 2003; Nolen-Hoeksema, 2001). Along with some biological factors, both psychological and societal factors (lacking in authority or control) account for such differences (Nolen-Hoeksema, 2001; Nolen-Hoeksema & Hilt, 2009). Adolescent girls from developing nations are likely to face more risk and hard times than boys, such as gender prejudices, violence, premature discontinuation of education and adolescent trafficking. In India, girls often face discrimination right from the moment they are born and in some cases even before they are born. They are likely to be breastfed for a shorter time, given less nutritious food and provided with less health care. During childhood, those girls who are able to attend school may drop out to help with household tasks, looking after younger children, fetching water and firewood, and preparing meals. The heavy loads combined with poor nutrition take a heavy toll on their bodies (Thangamuthu & Rasi, 2002). They also suffer from many psychosocial problems such as depression, anxiety, stuttering, bulimia nervosa and other psychosomatic symptoms (Aradhya, 2013). Somatic complications such as poor health, weakness, inability to do physical work and personality disorders affect both genders, but it affects adolescent girls more than adolescent boys. These problems also make it difficult for them to adjust in society and make it difficult to cope up with day-to-day activities. It leads to emotional problems and can be extremely distressing to many adolescent girls (Aradhya, 2013; Newman & Newman, 2015). Therefore, meeting the needs of such vulnerable groups and overcoming existing shortcomings in the delivery of tailored primary preventative measures would significantly improve their survival and general health conditions, nutritional status, and sexual and reproductive health of the future Indian adult population. In order to overcome the vulnerabilities of adolescents, the government of India has made important interventions with its ambitious welfare scheme which is the integrated child development services. Many researchers have, however, noted that adolescents living under institutional care have high emotional problems, poor health, difficulty in social interactions and poor adjustment levels as compared to those who live with their families (Padmaja et al., 2014). Intervention schemes by the states concerning the well-being of adolescent girls have been limited, but some studies suggest that such interventions might alleviate some of sufferings of the adolescent girls. Even in other developing regions like Africa, such studies have shown mixed results in terms of the efficacy of such government-run schemes.
This research analyses the various psychosocial issues faced by adolescent girls enrolled in Integrated Child Development Services (ICDS) centres. It is important to study such issues amongst girls because if these concerns are addressed, the country can have a healthier female population who can add to the growth of the nation. It is also important to address these issues as the growth and affluence of any nation depend a lot on the status and development of women (Razzak et al., 2017).
Literature Review
Somatic Complications, Social Withdrawal, Adjustment Problems, Attention and Sleep Problems of Adolescent Girls
Kekkonen et al. (2015) studied school-going adolescent girls in Finland aged between 13 and 18 years. A total of 288 girls were taken as the sample for the study and the results showed that in total, they had made 1,411 visits to the healthcare facilities. The data suggest that adolescents frequently visit the healthcare centres as they suffer from psychosocial problems. Research by Ilana and Jeanne (1989) suggests that many adolescent girls suffer from eating disorders which are caused by their concern for body image, physical growth and personality development. Another study by Caspi et al. (1995) revealed that temperament and behavioural problems such as lack of control and sluggishness were witnessed in adolescent girls. Tiwari and Ruhela (2012) did research on 300 adolescents with an aim of investigating the relationship between ‘social isolation’ with ‘depression’ among adolescents. The sample consisted of 150 adolescent boys and 150 adolescent girls. The results revealed a significant correlation between social isolation and depression. As compared to the boys, scores for girls were higher on the association between social isolation and depression. Adolescents also tend to limit their social interaction which can be caused by anxiety and depression. Rubin et al. (2010) suggest that peer relationships are correlated with social competence among children. A study by Erath et al. (2007) suggests that social skill deficits and improper coping strategies are two major factors that lead to anxiety and depression amongst women which gradually leads to social withdrawal and isolation. Adolescents also suffer from insomnia which affects both physical as well as mental health. The recommended sleep in adolescents is more than which is required in other phases of human life . It is reported by many researchers and surveys that adolescents sleep less than the recommended sleeping hours for them which is about 8–10 hours each day.
Review of Literature on Adolescent Girls with Reference to Socio-economic Status
There is ample evidence in the literature which implies that socio-demographic factors such as age, race, ethnicity, language, socio-economic status and education, influence health and nutritional outcomes. Joshi et al. (2019) conducted a study on socio-demographic factors and its correlation with the morbidity among 224 adolescent girls in a slum area of Pune and found that the majority of the adolescent girls (96.4%) were studying in school and were malnourished. Out of the 41.07% malnourished girls, 84.78% were suffering from anaemia. A majority of the girls (48.2%) belonged to class III of socio-economic status. In class III of socio-economic status group, mild, moderate and severe anaemia was reported in 50.45%, 41.51% and 36.36% cases, respectively. Moreover, adolescent girls belonged to lower-middle or upper-lower-class households. These girls reported common morbidities including anaemia, malnutrition (underweight, thinness and stunting), pediculosis, dental caries, helminthiasis, dysmenorrhoea and skin disorders. The common factors responsible for these morbidities included lower socio-economic status and overcrowding in their societies. A study conducted by De K (2017) on the effects of socio-economic status on the nutritional status of adolescent girls found that the outcomes of poor socio-economic status on families during the childhood phase lead to poor income in young adulthood with poor health conditions, inclination towards riskier and hazardous behaviours, and low educational achievements and poor career outcomes, in contrast to the higher socio-economic status people. Family income is also intensely associated with educational opportunities. A study carried out by Andrabi (2016) on the ‘assessment of socio-economic status among tribal and non-tribal adolescents of Kashmir’ found that both tribal and non-tribal teenagers differ significantly in socio-economic status. Further, the study revealed that there is no significant difference between the tribal male/female and non-tribal male/female students with respect to the socio-economic status in Kashmir.
Studies in Jammu and Kashmir
A study on aggression amongst Kashmir’s adolescents acquires particular significance in the context of a high level of aggression found among adolescents in general. Aggressive behaviour can be both appropriate, but alternatively, it can also be used as destruction to self and others. Occasionally, it may also lead to self-damaging acts like suicide (Ferris & Grisso, 1996). A retrospective study on suicide conducted by Shoib et al. (2012) in Kashmir recorded an increase of over 250% in the number of suicide attempts between 1994 and 2012. Khushresta (2016) conducted research on incidences of suicidal attempts and the occurrence of suicide in Kashmir. The study showed that one adolescent in Kashmir commits suicide every day. The study also found that 24,000 men and women, typically young, have attempted suicide in the last 17 years in Kashmir. Out of them, about 3,000 have been successful and the majority among them were between 16 and 21 years of age. It also showed that Kashmir has a much higher suicide rate than other states of India like Uttar Pradesh and Bihar. Shah (2018) conducted research on the prevalence of suicidal ideation and attempts among the youth in the Srinagar district of Jammu and Kashmir. The results showed that 28.3% have suicidal ideation and 7.7% of the respondents have attempted suicide.
Moreover, Jammu and Kashmir has been witnessing armed conflict for the last three decades which is mostly confined to Kashmir. Exposure to armed conflict leads to an increase in defiance, hostility and violent behaviour, risk-taking behaviour and other externalising problems (Baker, 1990). Armed conflict has a negative impact on the overall well-being of children and adolescents. Adolescents are the worst affected by the conflict as indefinite curfews and other restrictions have hampered their growth both academically and psychologically. They do not have any way of channelising their energy and, thus, they become the victims of psychological issues. Thus, from this perspective context, it is also important to study the psychosocial problems of adolescent girls in ICDS centres.
Rationale of the Study
Various studies have revealed the prevalence of psychosocial issues amongst adolescent girls worldwide, which makes it essential to examine the psychological problems amongst them (Crichton et al., 2013). Moreover, most of such research has been limited to developing countries (Crichton et al., 2013). A vast majority of developmental studies in recent times concern the psychosomatic development amongst adolescents, but some aspects remain unexplored (Dwivedi & Rastogi, 2019). In India, there has been a growing apprehension concerning adolescents’ psychological health (WHO, 2005). The data and other relevant statistics concerning adolescents’ health seem to be missing or inadequate (Bhola & Kapur, 2003). But, many studies have shown the incidence of psychological issues amongst young adults in India (Bhasin et al., 2010; Mohanraj & Subbaiah, 2010), especially amongst girls (Bhasin et al., 2010. According to Steinberg and Morris (2001), the psychosocial problems of adolescents are temporary in nature and are resolved during adulthood as their ability to think and problem-solving increases. Therefore, meeting the needs of such vulnerable groups and overcoming existing shortcomings in the delivery of tailored primary preventative measures would significantly improve their survival and general health conditions, nutritional status, and sexual and reproductive health of the future Indian adult population (Datta & Majumder, 2012). ICDS is one of the schemes of the government of India that caters to the nutritional, health and socio-economic development of adolescent girls (Gragnolati et al., 2006). However, the research into the role of ICDS in alleviating the problems of adolescent girls in India has shown mixed. Therefore, more research needs to be conducted in this domain, especially in those geographical regions where less research has been conducted.
Objectives of the Study
The purpose of this research work was to assess the socio-economic status of adolescent girls enrolled in the ICDS programme. Another study objective was to highlight and analyse the psychosocial issues of adolescent girls enrolled in the ICDS programme.
Hypotheses of the Study
H1: The adolescent girl beneficiaries of the ICDS programme in Kashmir are facing psychosocial problems of varied nature.
H2: The presence of psychosocial problems among adolescent girl beneficiaries of the ICDS programme is due to low-economic profile.
Methodology
The research approach adopted in this study is both explorative (exploring the research problem) and descriptive in character. The study aims to explore the socio-economic conditions and psychosocial problems of adolescent girls who were enrolled in selected ICDS centres in three districts (Srinagar, Budgam and Ganderbal) of Central Kashmir. A survey was used for collecting the data and quantitative analysis helped interpret the results in order to decipher the problem at hand.
Instrument Design
The scale comprised 30 items and represented five variables such as somatic complication, social withdrawal, adjustment problems, attention problems and sleep problems. For the socio-economic variables, community, district, type of ration card, age, type of family, place of living, education status and annual family income have been included as a part of the instrument.
Research Sampling
The sample in this work consisted of adolescent girls in selected ICDS centres in three districts from Central Kashmir. The adolescent girls who were finally selected in the sample belonged to the age group of 11–18 years. The method of sampling adopted was proportionate stratified sampling and selection was done by using random sampling method.
Sample Size
415 respondents were finally selected for the main study. This sample size adequately represents the population.
Data Cleaning
Data cleaning is a must before further analysis and, therefore, only 400 functional responses remained after removing outliers or deficient questionnaires from the 415 collected questionnaires. The data have also been checked for normality before conducting the final analysis. The values of skewness and kurtosis were within the acceptable values (±1.96) which signifies the data’s normality.
Pilot Study
Before proceeding for final data collection, a pilot survey has been suggested by previous researchers (Hair et al., 2010). Thus, for the present study, it was decided to collect data from a sample comprising 30 respondents. The sample for the pilot survey was collected from adolescent girls from the district of Srinagar using research controlled sampling technique. The AGMs’ psychosocial problems scale was subjected to scale refinement.
Exploratory Factor Analysis (EFA)
EFA revealed no cross-loadings amongst factors and all factor loadings were above 0.50. The KMO value for the scale items was found to be 0.947, which is above the suggested value of 0.6 (Kaiser, 1974). The scale also showed an acceptable value of Bartlett’s test of sphericity which was less than the suggested significance value of 0.05 and the total variance was 86%.
Reliability
The overall reliability of scale was 0.912, which was well above the threshold value of 0.6. The reliability of all the factors was found to be in the range of 0.941–0.982, which was well above the threshold value of 0.6 (Hair et al., 2010).
Analysis of the Data
The ANOVA test, Levene test, Hochberg test, Welch statistic/Brown–Forsythe statistics and equality of means test were used for testing the study hypotheses, which are discussed below.
Psychosocial Problems Among Adolescent Girls Enrolled in ICDS Centres
It is evident from Table 1 that Levene’s test is insignificant for somatic complication, social withdrawal, adjustment problems, attention problems and sleep problems. These results clearly indicate that the variance within the three groups is not statistically different. This is an assumption for the ANOVA test which should be checked before going for further analysis. Table 1 further shows that Levene’s test is significant for overall psychosocial problems. Consequently, homogeneity of variance cannot be assumed within the groups. Welch statistic/Brown–Forsythe statistic should be used in these cases as they are considered as most authentic measures in the case when homogeneity of variance is not present within the groups.
Psychosocial Problems in Relation to Age.

In Table 2, the significance value was checked, and it was revealed that social withdrawal and attention problems had significance values of 0.254 and 0.354, respectively, which are greater than the 0.05 value. Furthermore, the Hochberg test was selected as post hoc test to investigate the effect. This test is considered very productive when the sample size of the groups is unequal as we have the same case in our study, that is, 20, 61, 96 and 223. For somatic complication, adjustment problems and sleep problems, there was a significant change as the age of adolescent girls changed from 11–12 years to 13–14 years. There was no significant difference as the age of adolescent girls changed from 12–13 years to 13–14 years, 14–15 years and 15–16 years. Therefore, it is clear from the mean scores given in Table 2, that the somatic complication (M = 16.35), adjustment problems (M = 18.90) and sleep problems (M = 10.60) are more in adolescent girls falling in the age group of 11–12 years, compared to the adolescent girls of 13–14 years, 14–15 years and 15–16 years.
Psychosocial Problems in Relation to Age Using ANOVA.
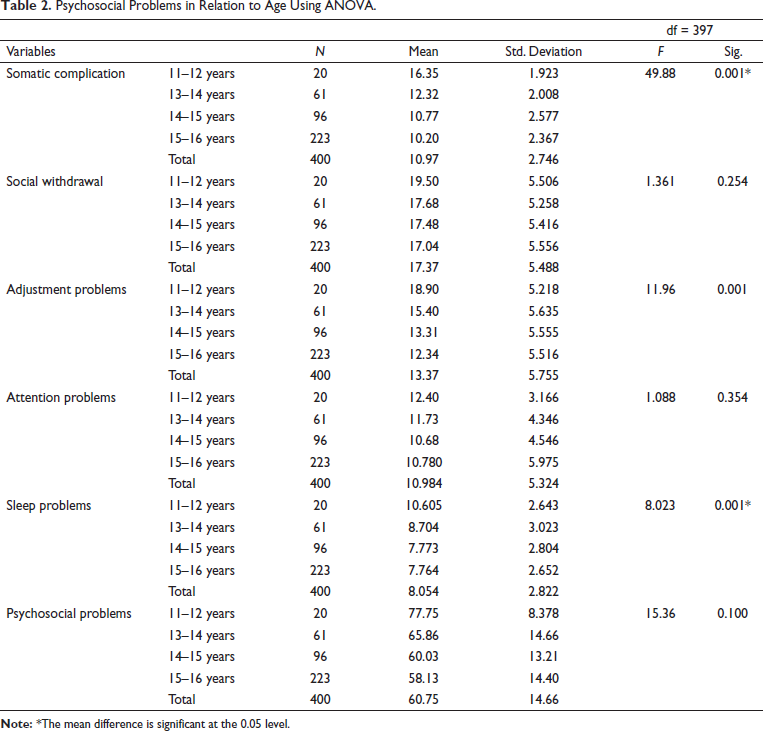
From Table 3, the values of Welch statistic and Brown–Forsythe were found statistically significant for overall psychosocial problems as p values were 0.001 and 0.001, which are below 0.05. In the case of overall psychosocial problems, the Games Howell post hoc test was carried out as it is considered best even when the assumption of homogeneity of variance is not met. The results reveal that there is a significant change in the overall psychosocial problems of adolescent girls as their age changes from 11–12 years to 13–14 years, 14–15 years and 15–16 years. Table 2 further reveals a drastic change in overall psychosocial problems when the age of adolescent girls changes from 13–14 years to 14–15 years and 15–16 years. However, there is no significant change in overall psychosocial problems when the age changes from 14–15 years to 15–16 years in adolescent girls.
Psychosocial Problems in Relation to Age (Equality of Means Test).

Districts
It is evident from Table 4 that Levene’s test is insignificant for adjustment problems, attention problems, sleep problems and overall psychosocial problems. These values evidently state that the variance within these three groups is not statistically different. However, Levene’s test is significant for somatic complication (p = 0.000) and social withdrawal (p = 0.007), which violate the assumption of homogeneity of variance for the ANOVA test.
Psychosocial Problems in Relation to Districts (Test of Homogeneity of Variance).
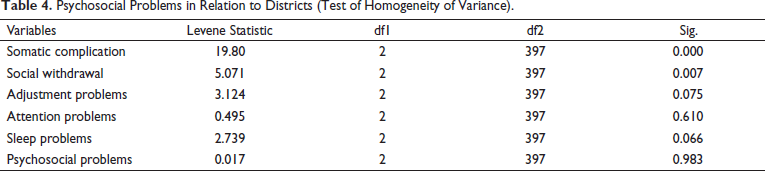
Table 5 reveals that the p values of adjustment problems (p = 0.001), attention problems (p = 0.041), sleep problems (p = 0.001) and overall psychosocial problems (p = 0.001) are statistically significant, as these are below the 0.05 level of significance. For attention problems and sleep problems, there was a significant change among adolescent girls as the district changed from Srinagar to Budgam and Ganderbal. There was no significant difference as the district changed from the Budgam and Ganderbal. However, there was a significant change among adolescent girls’ adjustment problems and overall psychosocial problems as the district changed from Srinagar to Budgam and Ganderbal and from Budgam to Ganderbal (Table 5).
Psychosocial Problems in Relation to Districts (ANOVA).
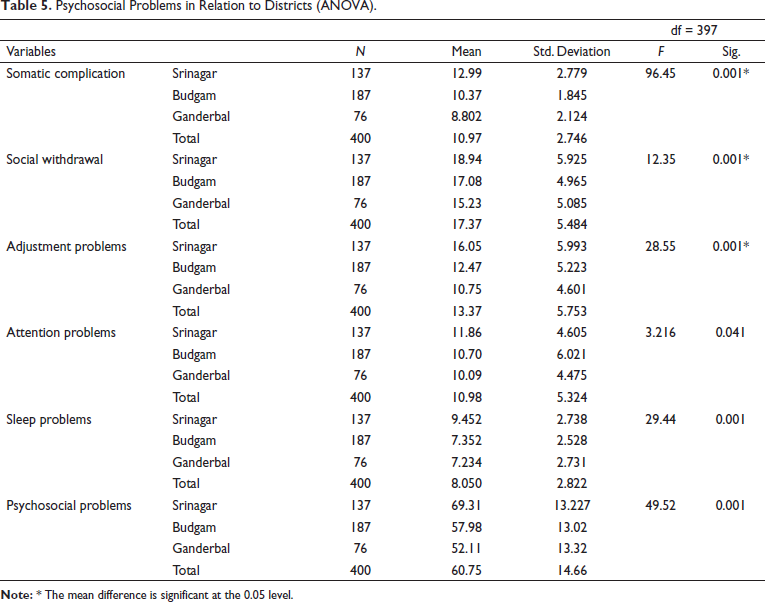
From Table 6, the values of Welch statistic and Brown–Forsythe were found statistically significant for somatic complication and social withdrawal as p values were less than 0.05. The results reveal that there is a significant change in both somatic complication and social withdrawal of adolescent girls as their district changes from Srinagar to Budgam and Ganderbal and from Budgam to Ganderbal. It is evident from the mean scores that the adolescent girls of district Srinagar experience more somatic complications and social withdrawal problems compared to the adolescent girls of district Budgam and Ganderbal. Similarly, the adolescent girls of district Budgam also experience significantly higher somatic complication and social withdrawal problems compared to the girls of district Ganderbal.
Psychosocial Problems in Relation to Districts (Equality of Means).

Area of Living
Table 7 reveals that Levene’s test is insignificant for somatic complication, social withdrawal, adjustment problems, attention problems, sleep problems and overall psychosocial problems.
Psychosocial Problems in Relation to Area of Living (Test of Homogeneity of Variance).
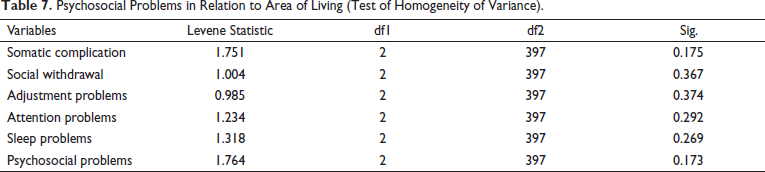
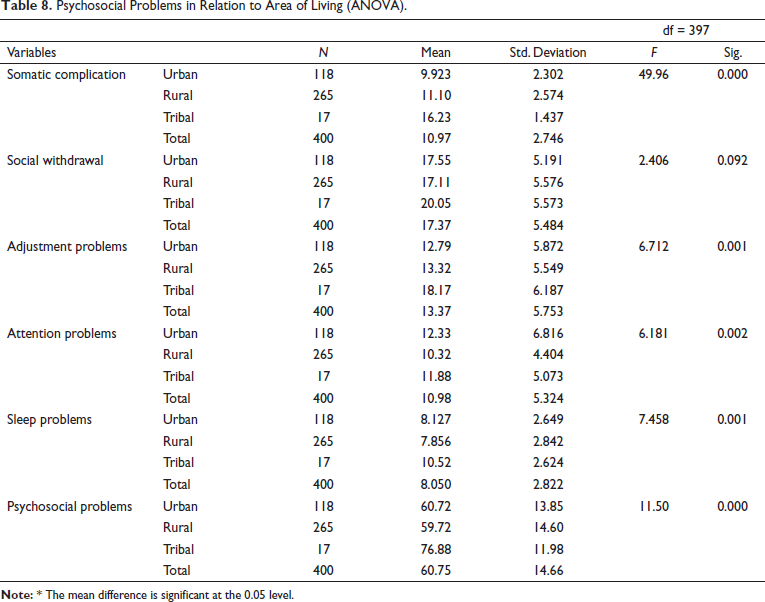
However, it was found that somatic complication, adjustment problems, attention problems, sleep problems and psychosocial problems had significance values of 0.001, 0.001, 0.002, 0.001 and 0.001, respectively, which are less than the significance value of 0.05 (Table 8). For somatic complication, adjustment problems, sleep problems and overall psychosocial problems, there was a significant change as the area of adolescent girls changed from tribal to rural and urban areas (Table 8). However, there was no significant difference as the area changed from rural to urban areas among adolescent girls. In the case of attention problems, there was a drastic change as the area of the adolescent girls changed from urban to rural and tribal areas. However, no significant change was found among the adolescent girls on attention problems as the area changed from rural to tribal areas. Table 8 further reveals that the significance value of social withdrawal was found to be 0.92 which is greater than the (0.05) level of significance. Therefore, it is evident that there is no significant difference in social withdrawal among adolescent girls with respect to the area of their residence.
Psychosocial Problems in Relation to Area of Living (ANOVA).
Difference of Ration Card Holders on Psychosocial Problems
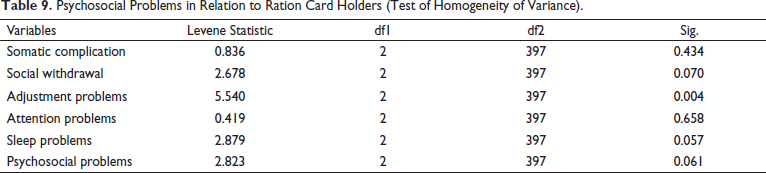
Table 9 reveals that Levene’s test is insignificant for the somatic complication, social withdrawal, attention problems, sleep problems and overall psychosocial problems. However, Levene’s test is significant for adjustment problems (p = 0.004), which violates the assumption of homogeneity of variance for the ANOVA test.
Psychosocial Problems in Relation to Ration Card Holders (Test of Homogeneity of Variance).
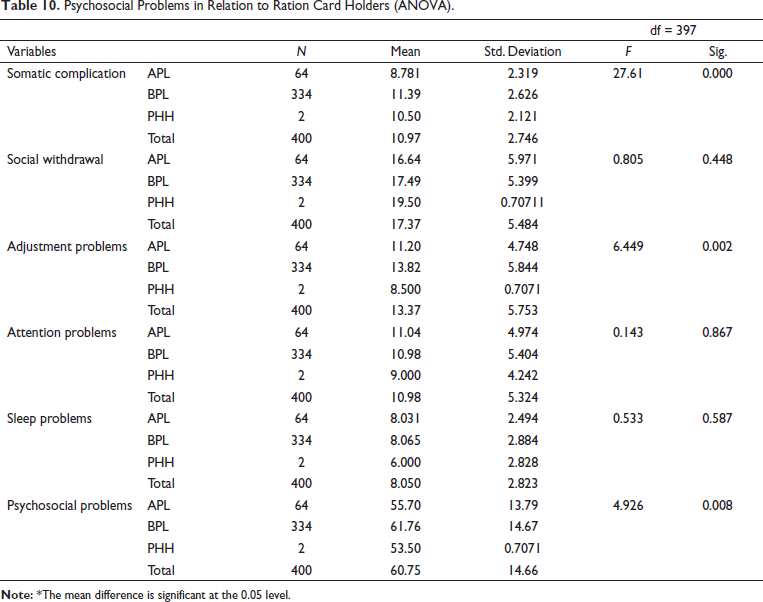
In Table 10, the significance value was checked, and it was revealed that social withdrawal, attention problems and sleep problems had a significance value of 0.448, 0.867 and 0.587, respectively, which are greater than 0.05 value. It clearly indicates that there is no significant difference in adolescent girls with respect to social withdrawal, attention problems and sleep problems with respect to the ration cards of their families. However, it was detected that somatic problems, adjustment problems and overall psychosocial problems had significance values less than 0.05. For somatic Problems, adjustment problems and overall psychosocial problems, there was a significant change as ration cards changed from BPL to APL and PHH (Table 10). It is evident from these results that the adolescent girls belonging to BPL families experience more somatic problems and overall psychosocial problems compared to the adolescent girls belonging to APL and PHH families.
Psychosocial Problems in Relation to Ration Card Holders (ANOVA).
From Table 11, the value of Welch and Brown–Forsythe statistic was found significant for adjustment problems, which indicates there is a statistically significant difference. It is evident from Table 10 that there is a significant change in adjustment problems of the adolescent girls as ration cards changed from BPL to APL and PHH as well as when the ration card changed from PHH to BPL and APL. The mean scores clearly indicate that the adjustment problems of adolescent girls belonging to BPL families experience more adjustment problems compared to girls belonging to APL and PHH families. Moreover, the girls belonging to APL families also experience more adjustment problems compared to the girls of PHH families.
Difference of Ration Card Holders on Adjustment Problems (Equality of Means).

Difference Across Different Education Groups
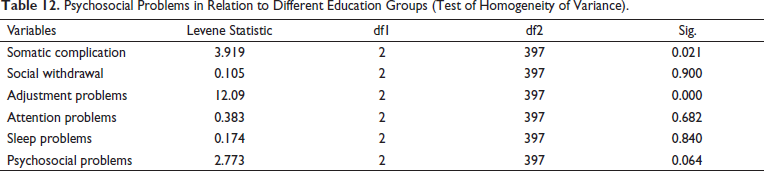
Table 12 reveals that Levene’s test is insignificant for the social withdrawal, attention problems, sleep problems and overall psychosocial problems. These values evidently state that the variance within these three groups is not statistically different. However, Levene’s test is significant for somatic complication (p = 0.021) and adjustment problems (p = 0.000), which violate the assumption of homogeneity of variance for the ANOVA test. Consequently, these values are considered as insignificant as they are above 0.05 (level of significance). It clearly indicates that there is no significant difference in adolescent girls on attention problems with respect to their educational status.
Psychosocial Problems in Relation to Different Education Groups (Test of Homogeneity of Variance).
However, it was detected that social withdrawal, sleep problems and overall psychosocial problems had significance values of 0.001, 0.001 and 0.001, respectively, which are less than the significance value of 0.05. So, it is clear from these values that there is a significant difference among adolescent girls on social withdrawal, sleep problems and overall psychosocial problems with respect to their educational status (Table 13). For social withdrawal, sleep problems and overall psychosocial problems, there was a significant change as educational status changed from dropouts to school going and never been to school. It is evident from the mean scores of the adolescent girls that dropouts experience more social withdrawal, sleep problems and overall psychosocial problems compared to the girls belonging to the school-going and never-been-to-school groups.
Psychosocial Problems in Relation to Different Education Groups (ANOVA).
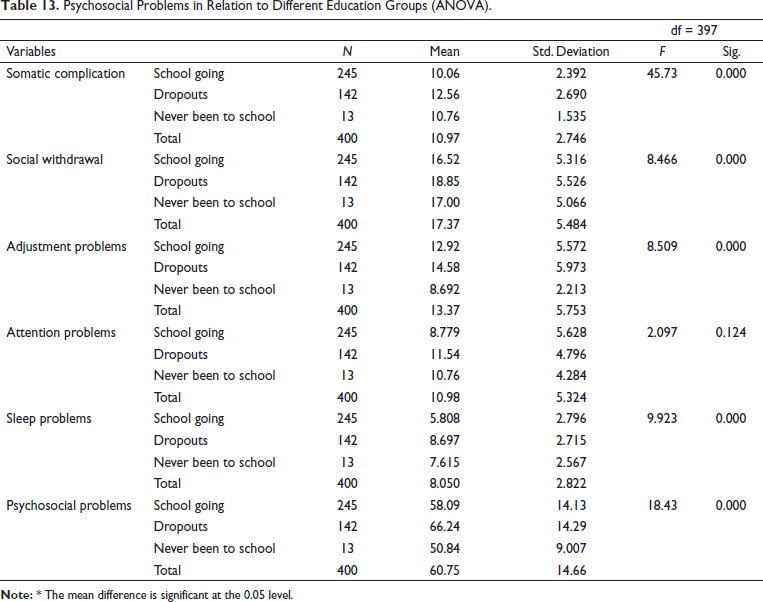
It is evident from Table 14 that the value of Welch and Brown–Forsythe statistic was found significant for somatic complication and adjustment problems, which indicates there is a statistically significant difference. It is evident from Table 13 that there is a significant change in the somatic complication of the adolescent girls as their educational status changed from dropouts to school going and never been to school. However, no significant change was found as the educational status changed from school going to never been to school. Moreover, a significant change was found in adjustment problems as educational status changed from ‘dropouts’ to ‘school going’ and ‘never been to school’ and ‘school going’ to ‘never been to school’. The mean scores clearly reveal that the school dropouts experience more adjustment problems compared to school going and never been to school. Furthermore, it was also found that adolescent girls who had never been to school also experienced more adjustment problems compared to the school-going girls.
Psychosocial Problems in Relation to Different Education Groups (Equality of Means).

It is clear from the above results that adolescent girls face a lot of problems with respect to different demographic variables. Therefore, our hypothesis Ha4, which states that ‘the adolescent girl beneficiaries of the ICDS programme in Kashmir are facing psychosocial problems of varied nature’, stands accepted.
Difference of Income on Psychosocial Problems
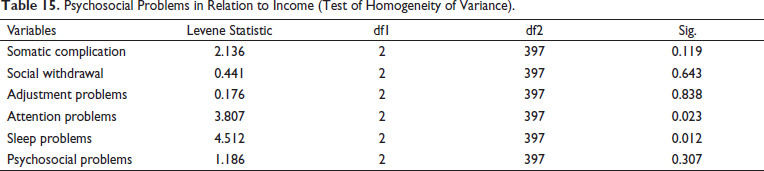
Table 15 reveals that Levene’s test is insignificant for the somatic complication, social withdrawal, adjustment problems and overall psychosocial problems. These values evidently state that the variance within these groups is not statistically different. However, Levene’s test is significant for attention problems (p = 0.023) and sleep problems (p = 0.012) which violate the assumption of homogeneity of variance for the ANOVA test.
Psychosocial Problems in Relation to Income (Test of Homogeneity of Variance).
In Table 16, the significance value was checked, and it was revealed that somatic complication and adjustment problems had a significance value of 0.276 and 0.131, respectively, which are greater than 0.05 value. However, it was detected that social withdrawal and overall psychosocial problems had significance values of 0.019 and 0.001, respectively, which are less than the significance value of 0.05. So, it is clear from these values that there is a significant difference among adolescent girls on social withdrawal and overall psychosocial problems with respect to the annual income of their parents.
Psychosocial Problems in Relation to Income (ANOVA).
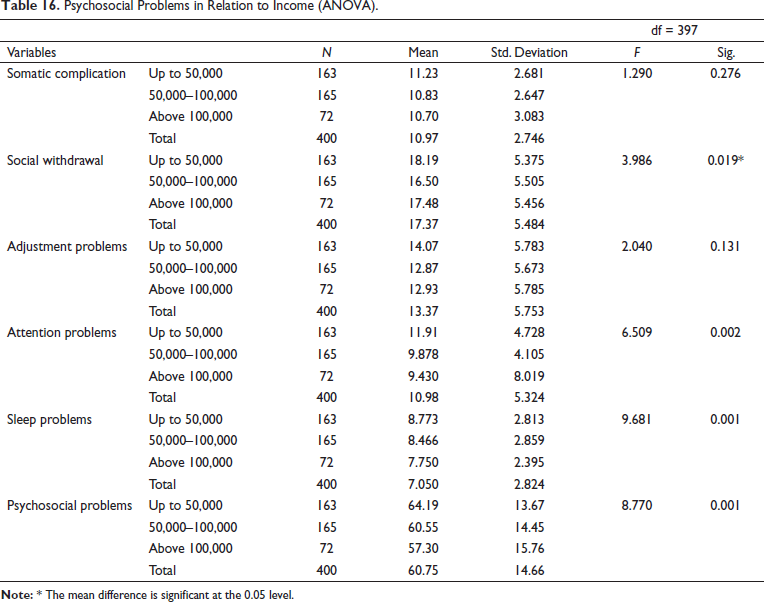
For social withdrawal (Table 17), there was a significant change as the income of the parents of adolescent girls changed from ₹50,000 per annum to ₹50,000–100,000 and above ₹100,000 per annum. However, there was no significant change in social withdrawal as the income of the parents of adolescent girls changed from ₹100,000 to above ₹100,000 per annum. In the case of the overall psychosocial problems, there was also a significant change as income of the parents of adolescent girls changed from up to ₹50,000 to ₹50,000–100,000 and above ₹100,000 per annum. Significant change in overall psychosocial problems among adolescent girls was also found as the income of their parents changed from ₹50,000–100,000 and above ₹100,000. It is evident that there is a significant change in attention problems and sleep problems of the adolescent girls as the income of their parents changed from up to ₹50,000 to ₹50,000–100,000 and above ₹100,000. However, no significant change was found when the income changed from ₹50,000–100,000 and above ₹100,000.
Attention Problems and Sleep Problems in Relation to Income (Equality of Means).

Therefore, it is evident from the results of Tables 15 –7 that the hypothesis Ha5, which states that ‘The presence of psychosocial problems among adolescent girl beneficiaries of the ICDS programme is due to low-economic profile’, stands accepted.
Findings and Discussions
The study revealed that somatic complication adjustment problems and sleep problems were found prevalent mostly in adolescent girls falling in the age group of 11–12 years compared to the adolescent girls aged 13–14 years, 14–15 years and 15–16 years. The reason could be linked to the initial stages of adolescence phase in which adolescent girls find such bodily changes odd that cause somatic complaints, adjustment problems and sleep problems. The results further reveal that there is a significant change in the overall psychosocial problems of adolescent girls as their age changes from 11–12 years to 13–14 years, 14–15 years and 15–16 years. A drastic change was found in overall psychosocial problems when the age of adolescent girls changed from 12–13 years to 13–14 years and to 15–16 years. The reason could be that as adolescent girls’ progress from one stage of adolescence to another, they adapt to such changes. This is the reason that such drastic changes can be observed.
For attention and sleep problems, there was a significant change among adolescent girls as the district changed from Srinagar to Budgam and to Ganderbal. However, there was a significant change among adolescent girls in adjustment problems and overall psychosocial problems as the district changed from Srinagar to Budgam and to Ganderbal and from Budgam to Ganderbal. The adolescent girls of district Srinagar experience more somatic complications and social withdrawal problems compared to the adolescent girls of district Budgam and Ganderbal. Similarly, the adolescent girls of district Budgam also experience significantly higher somatic complications and social withdrawal problems compared to the girls of district Ganderbal.
For somatic complications, adjustment problems, sleep problems and overall psychosocial problems there was a significant change as the area of adolescent girls changed from tribal to rural and to urban areas. In the case of attention problems, there was a drastic change as the area of the adolescent girls changed from urban to rural and to tribal areas. These findings are in contrast with the study carried out by Sood and Misra (1995).
The results also indicate that depression is more likely among children from lower socio-economic status families, joint/extended families, families where fathers are absent and families where parents have a problematic relationship. Further research suggested that interactions between these variables can cause problem behaviour in children.
No significant difference in adolescent girls on social withdrawal, attention problems and sleep problems with respect to the ration card category of their families was revealed. The adolescent girls belonging to BPL families experience more somatic problems and overall psychosocial problems compared to the adolescent girls belonging to APL and PHH families. Adjustment problems of adolescent girls belonging to BPL families experience more adjustment problems compared to girls belonging to APL and PHH families. Moreover, the girls belonging to APL families also experience more adjustment problems compared to the girls of PHH families. These findings are in agreement with the findings of Rajamanickam and Mercy (1992, as cited in Reddy, 2014) who reported that higher income was associated with better adaptation and some psychosomatic issues among adolescents in contrast with adolescents from low-income backgrounds.
No significant difference in adolescent girls on attention problems with respect to their educational status was revealed. Dropouts experience more social withdrawal, sleep problems and overall psychosocial problems compared to the girls belonging to ‘school going and never been to school group’. There is a significant change in the somatic complication of the adolescent girls as their educational status changed from ‘dropouts’ to ‘school going’ and to ‘never been to school’. The ‘school dropouts’ experience more adjustment problems compared to ‘school going’ and ‘never been to school’. Furthermore, it was also found that the adolescent girls belonging to ‘never been to school’ also experience more adjustment problems compared to the ‘school-going girls’.
Conclusion
The study objectives were successfully tested with the help of different statistical techniques that revealed interesting information about the psychosocial issues faced by adolescent girls in ICDS centres. This research work also examined the relationship between different socio-economic variables and psychosocial problems with respect to the adolescent girls. Psychosocial problems or issues such as somatic complications, social withdrawal, adjustment problems, attention problems and sleep problems were found to be prevalent amongst the study respondents. The research findings also reveal that the majority of the girls belonged to marginalised sections of the society in terms of the economic status. The nation’s development is intricately linked with the education and status of the women in the society. Taking care of the girls’ requirements at a young age is a desirable social investment which ultimately leads to the nation’s future progress and growth. ICDS in essence represents the aspirations and spirit of a ‘New India’, which is committed to reach out to the most needy and deprived sections of society.
Suggestions
It was observed that the majority of the study respondents suffered from psychosocial problems like somatic complications, adjustment problems, sleep problems, attention problems and sleep problems. This means the ICDS should resort to making significant attempts to solve the problems and issues amongst adolescent girls. This finding can help programme implementers to hire trainers or workers who are adept in primary healthcare. Even medical practitioners can be called for occasional visits to ICDS centres to provide care and offer counselling sessions on such issues. This can offer insights to public policymakers to target adolescent girls from weaker and marginalised sections of the community. Region-specific issues ought to be dealt with through training interventions. Instant steps are required to be taken by the state to determine these issues and intervention modules need to be adapted with the guidance of specialists in this area. The proposed adolescent development education programme, though not complete and comprehensive has tried to tackle these issues to a certain extent. Programmes can be plotted out with a positive youth development framework in mind. More opportunities can be offered to these girls for pro-social engagement, for example, getting associated with environmental protection, service activities, etc. Building up the fortnightly AG (Anganwadi) club activities can be the crucial point for organising the adolescent girls in the neighbourhood. As proposed by the working group for the eleventh plan, NYK (Nehru Yuva Kendra) activities can be organised through AG clubs of the Anganwadi centres.
Health workers should also be properly trained so that they can counsel these girls on various issues such as mental health and physical health. ICDS centres can also hire specialists that can provide special attention to these girls to resolve any problems faced by them. They can also apprise these girls on various developments and challenging situations they might face in the future. They can provide assistance on how to avoid risky behaviour, build resilience and acquire the necessary skills to utilise the opportunities in their lives. These experienced professionals and trainers can help these girls to imbibe constructive values, build societal competencies and build a positive self-identity for a better future. Social workers can play a huge role by educating adolescent girls about menstrual cycles. Such orientation sessions with adolescent girls can take place at Anganwadi centres or at the school. Schools should always be the preferred choice as social workers can find most adolescent girls together in one place, that is, school.
Limitations and Future Research Directions
The study was only exploratory in nature, which limits its scope to develop an intervention programme for adolescent girls. Future researchers can focus on other research designs like qualitative or triangulation for better insights into the problem. Limited demographic data were collected for the sample in this study. Information regarding birth order in the family would also have been an important variable to be included in the analysis. A number of variables can influence the psychosocial issues of adolescent girls which were ignored in the study. The future works can examine the role of parents in helping their adolescent daughters deal with their psychosocial issues and improving their quality of life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.