
Abstract
Hospital discharge is a complex matter. For patients it often involves insecurity; for hospitals, efficiency plays a major role. The consequences include uncertainty and anxiety among patients, unnecessary readmissions and rising costs for hospitals. Like in hotels where the check-out is the last part of the guest journey, the hospital discharge is crucial for, among other things, image-building. Improving the hospital discharge procedure contributes to a better patient experience and quality of life, word-of-mouth advertising, efficiency and costs for the hospital. In this preliminary study, the hospital discharge in a cancer clinic was studied. It was assumed that the hospital discharge went according to a protocol and a fixed procedure and to everyone’s satisfaction. In order to verify this, the procedure was examined and compliance with the protocol was checked. Amongst others, it became clear that patients experienced the planning of the hospital discharge as unstructured and improvised as there seemed to be no clear moment for discharge. On the staff side, the main focus was on the administrative burden of discharge. Furthermore, a clear coordination and division of tasks between the doctors and nurses was lacking. Hotel management check-out procedures are suggested to improve hospital discharges.
Introduction
Where one patient is overjoyed and cannot wait to go home, another dreads the idea of being discharged. Having to leave the hospital again after an admission triggers a lot of emotions in patients. The hospital discharge procedure remains problematic. Some hospitals hardly involve patients in their discharge, nor are their wishes and needs clear; other hospitals encounter difficulties dismissing patients because they experience the hospital stay as a ’luxury’ or dread the loneliness at home. On the hospital side, there is often a great deal of pressure on the capacity of staffed beds (Hesselink et al., 2013; Waring et al., 2014). Research shows the persistence of this problem (Gonçalves-Bradley et al., 2016; Shepperd et al., 2013). The consequences can be guessed: in addition to uncertainty and anxiety in patients, unnecessary readmissions and rising costs (Kiers, 2017).
Both hotels and hospitals consider customer/patient satisfaction important for their good reputation. However, hospitals prefer to see as few patients as a possible return for the same condition (re-hospitalisation or unplanned readmission) but do hope to see them return when they need healthcare. This is because repeat visits are a good indicator of loyalty to and quality of an organisation (Lemon & Verhoef, 2016). Guest journeys provide insight into the various moments of truth and decisive contact moments in the guest experience. In the patient journey—from the point of view of hospitality—the discharge together with the reception is the most important contact moment (Zygourakis et al., 2014). And just like in hotels, this is crucial for, among other things, image-building. Hospitals, on the other hand, want to limit the number of readmissions and at the same time improve the patient experience. Improving the hospital discharge procedure contributes to a better patient experience, word-of-mouth advertising amongst patients, their households/families and their general practitioners, efficiency and costs for the hospital.
In this preliminary study, the hospital discharge in a Dutch cancer clinic was studied. It was assumed that the hospital discharge went according to a protocol and a fixed procedure and that this was done to everyone’s satisfaction. In order to verify this, the procedure was examined and compliance with the protocol was checked. Furthermore, departing from hotel management, that is, hospitality stance, the comparison with the check-out as part of the guest experience was made in order to share hospitality policies and/or knowledge to the healthcare industry.
Hospitality in Hospitals
Hospitality in Healthcare
Hospitality as a concept can roughly be framed in two different ways. Broadly speaking, one can say that there are two main streams: One deals with issues in the hospitality industry—research ’for’ hospitality—and the other studies hospitality—research ’of’ hospitality—as a social phenomenon (Lashley, 2017). Today, the majority of the literature on the concept of hospitality and related services such as the provision of food, drinks and accommodation comes from the commercial hospitality industry, so the subject may well tend to dominate. As a result, the term ’hospitality’ remains poorly defined, as it may not capture the essence of hospitality, limiting its intellectual potential (Lashley, 2017; Lynch et al., 2011).
What is generally agreed is that hospitality distinguishes itself from other forms of service provision by its behavioural component, namely hospitable behaviour (Ariffin et al., 2013; Tasci & Semrad, 2016). Hospitality and ‘hospitableness’ are interrelated concepts; however, their meaning is different. Hospitality derives from the Latin hospes, meaning ‘host’, ‘guest’ or ‘stranger’. This is the basis on which the words, amongst others, host, hospitality, hotel, hostel, hospice and also hostile (sic) are based. ‘Hospitableness’ is an elusive concept which can be defined as a behaviour or an attitude (Ariffin et al., 2013; Lashley, 2007). The elusiveness of the concept of ‘hospitableness’ is the way it is abstract and intangible. ‘Hospitableness’ is adaptive to its situation, as it changes depending on the extent of familiarity between host and guest (Lashley, 2007).
In order to apply the concept of hospitality to a broader context, Lombarts (2018) developed a revised model of hospitality, adapting the ancient and renowned model of Reuland et al. (1985). This revised model focuses on the service provider, direct and indirect stakeholders and their interaction in a given context (Lombarts, 2018). It addresses hospitality as an experience, not a transaction. The behavioural component of all stakeholders is taken into consideration, looking into the needs and goals of the direct stakeholder and into the interests of the indirect stakeholders. As a result, this hospitality experience model can be applied to more situations rather than the commercial hotel management or corporate hospitality ones only; hence, it is also applicable to healthcare situations.
As early as the 1990s, Hepple et al. (1990) looked at the most important elements of hospitality, that is, behaviour, product and environment, and showed that the behavioural component has the greatest influence on the patient’s perception during admission. Bitner (1992) looked more in particular at the impact of the physical environment on one’s behaviour whereby interaction and reciprocity were distinguished as important determinants in service delivery. Relating to more recent research, Rosenbaum and Massiah (2011) translated Bitner’s seminal servicescapes’ framework beyond a physical dimension and underlined the importance of the service experience that ought to be physically appealing, socially supportive, symbolically welcoming and naturally enjoyable. When studying the factors affecting the quality of healthcare services, Mosadeghrad (2014) mentions as well the environmental factors next to organisational factors and the customer- and provider-related factors. Moreover, he concludes that empathy is one of the five determining factors of the experienced quality. The other factors relating to the perceived quality are the more tangible ones such as the environment, efficiency, effectiveness, and efficacy (Mosadeghrad, 2014, p. 78). Tasci and Semrad (2016) use the term ‘hospitableness’ instead of empathy as crucial for creating a memorable experience and distinguish three distinct features of ‘hospitableness’: heart-warming, heart-assuring and heart-soothing. They define hospitableness as a construct to initiate an emotional response in the interaction, thanks to one’s personality, attitude or behaviour. Also, Pijls et al. (2017) developed an Experiential Hospitality (EH) scale and looked beyond the personal interaction level, the main focus of Tasci and Semrad (2016). However, the EH scale shows a great resemblance with the hospitableness scale of Tasci and Semrad, particularly on the interaction level: The heart-warming features are comparable with Pijls’ experiential factor ‘inviting’; the heart-assuring with the experience of care; and the heart-soothing with the experience of comfort. Interestingly, Pijls’ original nine categories have been reduced to three main dimensions in which the three categories of entertainment, efficiency and surprise no longer appear as hospitality experience dimensions. Recent research indeed indicates that hospital professionals do not see these three categories as the five most important hospitality traits with regard to healthcare (Hermans, 2018; Maarel, 2018; Schaik, 2018).
It can be concluded that the human aspect or the behavioural component in the service provision, either described as empathy, hospitality or hospitableness, in brief, the relational process has over the years become a decisive factor in the perception of the client, guest or patient.
The Patient Experience
In the Netherlands, the healthcare system is centred around basic insurance, which is mandatory for all residents. The government is responsible for setting healthcare priorities. As such, hospitals’ financing derives from the government and the insurance companies. Patients have the option to choose their hospital; however, many patients do not seem to be aware of their deliberate choice as there is no clear moment in their medical journey to choose a hospital. As a result, many patients do not expect anything more than their ‘medical’ care.
However, societal changes have an impact on hospitals. Our ageing population is suffering from multiple conditions, and their healthcare beds are increasingly complex; a lot of diseases become chronic, and patients are turning into repeat and ever more demanding ‘customers’ (Idenburg & Schaik, 2010; Victoor et al., 2014; Zygourakis et al., 2014). Next to that, hospitals are under increasing pressure to improve their performance as one of the key indicators of the hospitals’ success.
The traditional hospitality industry focuses on the attraction of guests. This ‘deterministic’ setting of Dutch healthcare makes one question whether hospitals would need to consider hospitality or ‘hospitableness’ at all as the patients will come either way. With the inevitable changes in society, there is a growing demand from hospitals to improve the patient experience. A good interpersonal relationship between patient and caregiver improves the quality of healthcare (Bayer et al., 2016; Meyer, 2018; Mosadeghrad, 2013). The involvement of the patient and the patient’s trust are key factors for achieving desired outcomes (Mosadeghrad, 2014). The experience of the patient is an important outcome of medical care and a key component of the quality of care.
Hospitality is the social interaction, the experience between patient and caregiver. The quality of care may be improved by the extent of empathy exchanged by these two stakeholders. Empathy reflects ‘hospitableness’, as ‘hospitableness’ is measured by the three H’s: heart-warming, heart-assuring and heart-soothing. The two concepts of empathy and ‘hospitableness’ overlap, which means that ‘hospitableness’ contributes to a higher quality of care. The patient experience and quality of care related; however, receiving a high quality of care does not necessarily imply that the patient experience was good. The patient may have received excellent care and still pass away. It goes without saying that in this example the patient experience (at least for their loved ones…) was poor.
For a long time, the patient’s perspective on his experience of healthcare and care provision has been overlooked as an important input. Interactions between patient and caregiver are defined as ‘The orchestrated touchpoints of people, processes, policies, communications, actions, and environment’ and patient perceptions are ‘what is recognised, understood and remembered by patients and support people’ (Wolf et al., 2014). The management of hospital patient flow can provide safe, efficient and effective patient care. Moreover, hospital resources can be used to the best of their abilities that way (Gualandi et al., 2019).
Thoughtfully designed interpersonal interactions are necessary to gain a good understanding of the patient’s medical history and condition throughout the entire patient experience. It allows for the caregiver to understand the social determinants and goals of the person seeking care, contributing to building common ground, which is necessary for the development of a personalised treatment plan (Hunter-Jones et al., 2020). Perhaps even more important is that Hunter et al. emphasise to look at the patient holistically, as a cognitive, emotional and social being and to see the health journey as a relational rather than a transactional process (Hunter-Jones et al., 2020, p. 5). This required mindset applies to all hospital staff and not only to medical staff that needs to gain a good understanding of the patient’s medical history and condition.
The perception of the patient’s relationship with the professional is a key issue for the quality of service. Patients remember moments that are not specifically related to the clinical care they receive, but moments that are of value to the patient. These other moments are of value to the patient as they show attention to the patient as an individual. An example is a nurse coming by to say goodbye to the patient as she would not see the patient anymore for the rest of the duration of her shift (Gualandi et al., 2019).
In order to provide the highest quality of healthcare, mapping the patient journey is an increasingly valuable tool for healthcare companies of all types and sizes, for many applications. As mentioned before, the patient plays a fundamental role in determining the quality of healthcare, managing patient data and streamlining medical diagnostics. Three critical needs for a better patient-centred experience:
Making the patient’s health goal visible;
Instigating transparent, shared decision-making;
Using a closed-loop communication process (Meyer, 2018, p. 1).
Hospital Discharge
Gualandi et al. distinguish seven main phases in the journey: (1) outpatient visit, (2) examination of outpatient clinic, (3) hospitalisation and surgery, (4) post-surgical care, (5) discharge, (6) rehabilitation stay and (7) follow-up visit (2019, pp. 4, 7–8). Discharging patients from the hospital can be considered (as one of) the final stages of the patient journey —but the beginning of another. It is considered to be a process and not an isolated event impacting the family and caregivers involved majorly (Kamalanathan, 2015). Discharge planning gives patients the possibility to move from one healthcare setting to another—in most cases their homes. Efficient discharge planning ensures seamless continuity of care to meet the patient’s post-discharge needs in order to avoid re-hospitalisation (Leland et al., 2019; Pedersen et al., 2018). Thus, it is extremely important as it may have severe implications for the patient’s future health. Though discharge is often considered the end of the patient’s journey within the hospital, it is the start of the rest of the health journey for the patient. Often overlooked, hospital discharge may have a significant impact on how patients enter the next phase of their journey to health.
The enhancement of the continuity of care is the primary aim of discharge planning. Moreover, efficient discharge planning has significant implications for a patient’s well-being and recovery, the efficient use of medical resources and the effectiveness of hospital management processes. The discharge process’ complexity requires careful planning in order to make the process an effective one (Kamalanathan, 2015).
The principles of discharging patients from the hospital have not changed over the years; however, the pace and process of discharge planning have changed. This is a result of external forces: political, financial and cultural. However, predicting the future of Dutch healthcare is challenging. Forecasting which of these forces or trends will manifest itself and in what way has proven to be a hard task (Idenburg & Schaik, 2010). Currently, the ageing population requires complex healthcare needs which need to be met (Idenburg & Schaik, 2010; Lees, 2012). Nevertheless, two fundamentals have been identified to shape the process of an efficient and ‘good’ discharge process: (1) the planning of the discharge and (2) the communication with the patient in question (Lees, 2012). There are multiple situations in which not enough attention is paid to the two components: understaffing, poor communication and attention, and pressure to discharge patients as quickly as possible (Bowles et al., 2003).
Looking into more detail the two fundamental issues of discharge planning, the first one, the planning of the discharge, shows that the patient’s readiness for discharge is a commonly used criterion for the discharge planning process and a predictor of re-hospitalisation risk (Weiss et al., 2015). It is therefore important to carry out thorough discharge planning in order to minimise the chance of readmission. Additionally, other research has found a correlation between negative working conditions for the caregiver and poor discharge planning (Carthon et al., 2015; Lasater & Mchugh, 2016; Ma et al., 2015; Mistiaen et al., 2007). This indicates that context does influence the quality of discharge planning. In other words, it is crucial to understand a given context thoroughly in order to improve the process of discharge planning. As ‘hospitableness’ plays a fundamental role in the hospital context, it also influences discharge planning and must be considered in the process.
The second fundamental point concerns the patients and their family caregivers’ often unmet information needs as a result of inadequate preparation (Driscoll, 2000; Henderson & Zernike, 2001). The information was possibly communicated but not in a way which was clear enough for the patient to understand or remember or the needed information was not given in the first place. Another explanation is that information was provided by the caregiver; however, it was not the information the patient needed post-discharge. Thus, an information gap exists between the patient and the caregiver. From the above, the following themes have been formulated:
The needs of the patient imply the extent to which a patient needs to be involved in the process of discharge planning. The expectations of the caregiver imply what the caregiver expects his/her role to be in the process of discharge planning. Discharge planning in its given context implies the ‘how’ of the concept in the setting of a specific hospital. Communication implies the communication between the patient and caregiver and their perception of the communication.
In short, understanding the process of discharge planning and communication within its given context is important for improving the discharge. Moreover, an understanding is required from both perspectives of patient and caregiver to see whether gaps between the two exist. Once the gaps are identified in a specific context, it becomes clear what possible obstacles are.
Data and Methods
Study Design
This research was a qualitative explorative research with a phenomenological hermeneutic approach making use of interviews with patients and staff members such as doctors and nurses (Laverty, 2003; Starks & Brown Trinidad, 2007). Hermeneutic phenomenology is concerned with language and understanding, inseparably bound together, an ongoing and evolving interpretation of the lived experience, of what it means to be human (Laverty, 2003; Van Manen, 1990). Gadamer’s hermeneutic phenomenology is followed, which focuses on concepts such as inter-subjectivity, authenticity, temporality, historicity, pre-supposition and play (Regan, 2012).
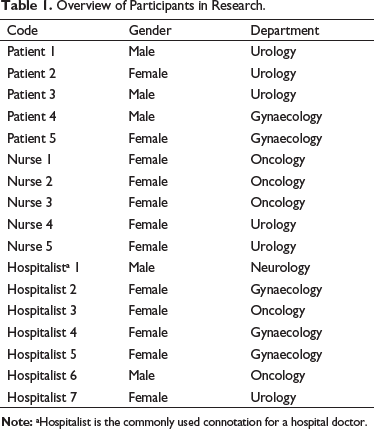
The research was done in a Dutch cancer clinic with x beds. Patients who had been operated on and dismissed were selected as well as doctors and nurses who were involved in the discharge procedure. The hospital was involved with the selection of the patients who had been hospitalised at various departments (see Table 1). As it concerned only non-clinical or non-medical information, it was not necessary to have a statement of approval of the hospitals’ medical-ethical review commission.
Overview of Participants in Research.
Next to the qualitative research, quantitative data from patient experience surveys from the hospital were used to check if these substantiated the qualitative findings.
Data Collection
As an introduction to the research and the professionals in the hospital, a preliminary interview was held. This provided information on the subject useful both for the literature review and as a guideline for the data collection.
The data collection took place between April and July 2020, right in the middle of the first lockdown due to COVID-19. This meant that the interviews with the patients were held by phone, with the hospital professionals, and the interviews were all held in private offices within the hospital. This ensured privacy and a higher quality of recording. In total seven hospitalists, five nurses and five patients participated, all on a voluntary basis and by assuring anonymity and confidentiality.
A purposive sample of patients was selected on the basis of their having undergone surgery and consequent discharge during the data collection period. They all had stayed at least one day and one night at the hospital, at the departments of gynaecology, urology or neurology and they all spoke Dutch. With this, a small but nice spread of the various departments was guaranteed. In order to identify the different viewpoints of a variety of hospital professionals working in various departments, also a collaborative purposive sampling technique was used. As selecting the staff members was beyond the researcher’s expertise and capabilities, she was assisted by a hospital doctor and two care managers.
All interviews were recorded after the researcher obtained permission and transcribed verbatim. Patients were only approached if the doctors deemed it ethically correct. Once the patient agreed to participate, the hospitalists requested the patient to fill out a form of informed consent which was prepared by the researcher. This form was handed to the patients 48 hours before discharge and collected 24 hours before discharge.
The quantitative data were collected from surveys which were carried out by the hospital self over the past three years. The utilisable number of survey answers or respondents differs from 673 to 1,043.
Data Analysis
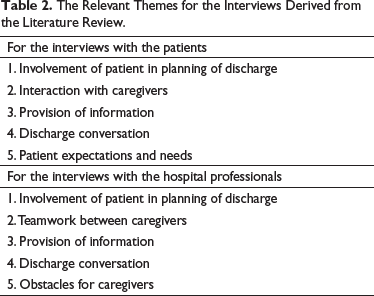
The preliminary interview was semi-structured as a list of open questions was prepared beforehand. Afterwards, the interview was transcribed and coded using qualitative data analysis software, specifically Nvivo software with an inductive approach as the codes were created in accordance with the data. Inductive reasoning means that general conclusions are drawn from gathered data, which is what happened in an analysis of this interview (Georgsson & Staggers, 2016; Kaczynski, 2004). After answering these questions, the current situation with respect to hospitality was discussed between the care managers and the hospitalist, showing their different perspectives on the current discharge policy. Both inductive (from the preliminary interview and as a basis for the following interviews) and deductive coding were used to code the interviews with the patients and hospital professionals during the data collection. The insights obtained from the literature review resulted in the following relevant themes for the patient and staff members’ semi-structured interviews (see Table 2).
The Relevant Themes for the Interviews Derived from the Literature Review.
The survey questions mainly connect to the theme of the provision of information. They are considered important as they show whether everything that should have been discussed with patients when discharged was done. It gives more insight into whether the time was taken to ensure the patient understood all the information they needed.
Findings
From the Patients’ Perspectives
1. Involvement of patient in the planning of discharge
None of the patients had a choice in deciding the moment of discharge. Patient one and patient three stated that they were ‘informed the same day’. The other three patients stated that they ‘knew that from the previous day, if it stayed the same’ that they would be ‘allowed to go home’ (Patient 5). All of them were able to inform their family timely of their discharge, and they were informed timely enough to arrange transportation home.
2. Interaction with caregivers
All of the patients were satisfied with the way that the caregivers interacted with them.
‘I felt that I was in very experienced hands, and that goes for the whole team.’ (Patient 3)
Patient four mentioned that the nurses ‘have time to explain things you later on things have questions about. They are the most important and best channel’.
3. Provision of information
Four out of the five patients mentioned that bits of information were communicated prior to discharge ‘every time it’s a piece of this, a piece of that, oh yeah and then that…’ (Patient 4).
This patient also mentioned that the reason for this was they did not have the time for it otherwise, ‘it’s not that it all goes according to a certain standard, there are certain actions that need to happen. However, those only happen when they have the time for it.’
Part of the formal discharge procedure is to call the dismissed patient the day after the discharge. However, four out of the five patients stated that they did not receive this phone call. Patient 3 did receive the phone call; however, he ‘was under the impression that the lady was not completely focused on our conversation, but that could also seem that way because it was a phone call. But it was very superficial’.
4. Discharge conversation
All the reactions to the discharge conversation were that it was ‘barely a conversation’. Patient 3 stated ‘the conversation itself was meaningless. And then I mean absolutely meaningless.’ Moreover, he stated that the discharge conversation was ‘disturbed’ because the nurse’s phone rang ‘every 10 to 20 seconds’ and ‘she took the phone every time’. Patient 2 also mentioned that ‘the discharge conversation did not add any value’. Furthermore, he mentioned that he overheard the doctor and nurses talking just outside his room, as ‘they said they needed the room for a new patient.’
5. Patient expectations and needs
Patient 3 stated that he was told he would ‘receive instructions for home, medication, etc.’ and that the caregivers would ‘take time for that’. However, when it did not happen, patient 3 had to ‘ask for it and that was annoying. Then I took matters in my own hands’. He also mentioned that he had to take responsibility to collect the information he needed ‘I did get everything, but actually it was me who mainly collected it.’ For a proper discharge, the caregivers should ‘take a moment for summary or recap’.
Patient 2 mentioned that it was not clear what he had to do. ‘Well, so that was partly explained, but not entirely. And in the end, it all became clear so that uhm… But it was a bit improvised, so to speak.’
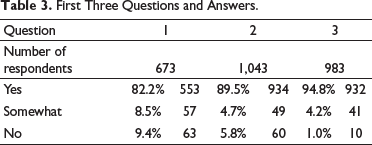
The survey questions concern the discharge process and relate mainly to the theme of provision of information. They substantiate the qualitative data and give more insight into whether the time was taken to ensure the patient understood all the information they needed.
Did someone explain to you about your new medicine when you went home? Did someone explain to you when to contact the hospital? Did someone explain to you who to contact when complications arise?
First Three Questions and Answers.
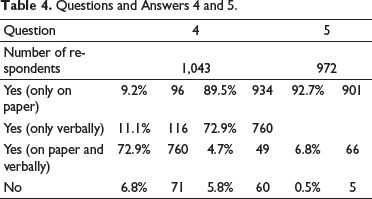
Did you receive lifestyle guidelines when you went home? Were these lifestyle guidelines clear for you when came home?
Questions and Answers 4 and 5.
From the Hospital Professionals’ Perspectives
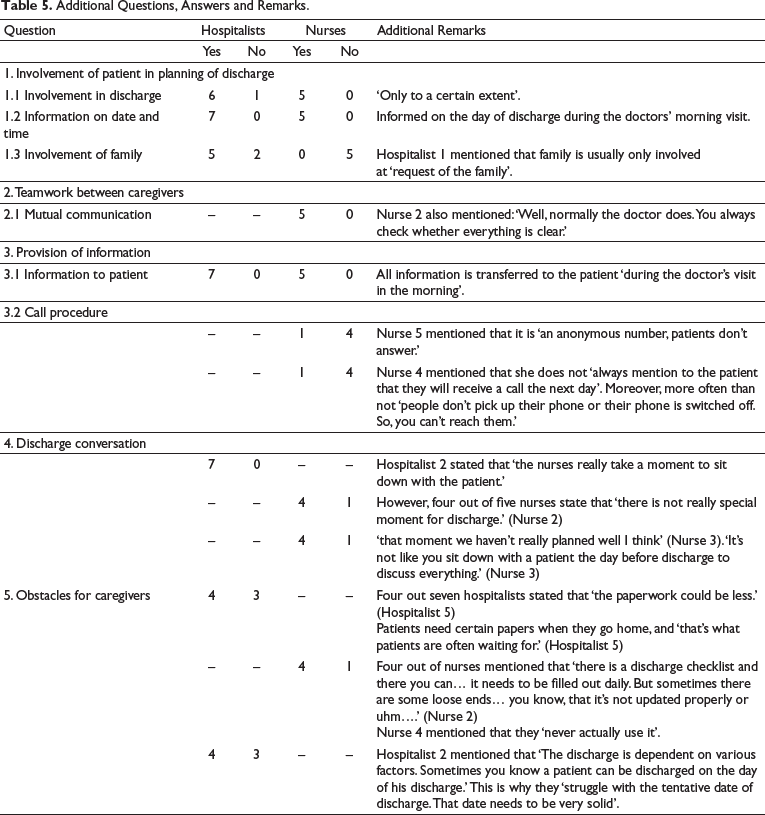
The patient must be medically ready to leave the hospital; moreover, the patient must be able to go home. Table 5 provides a comprehensible summary of the frequency of specific answers and by whom they were given, the hospitalists or nurses. Comments clarifying the answers or elucidating other divergent opinions have been presented.
Additional Questions, Answers and Remarks.
Discussion and Conclusion
This research revealed that the discharge process is not clear, neither to the patients nor to the staff. It outlines three major problems: (i) the moment of and communication around the discharge, (ii) the mutual communication between hospitalists and nurses and the (iii) follow-up call procedure.
First of all, the hospital discharge currently lacks a clear and dignified moment of discharge. Both patients and caregivers acknowledge the need for a specific moment serving for caregivers to summarise the patient’s hospital stay and allowing them time to provide information on the aftercare for patients. Patients expect the caregivers to take a moment to carefully go through their hospital journey and what comes after. A moment where the caregiver has full attention for the patient is expected to answer questions and reduce the patient’s feeling of anxiousness. Moreover, the focus should be on taking time for these patients to ensure a moment of closure. Such a moment would also allow to inform patients properly on the call procedure which currently is lacking clarity. Secondly, the actual discharge process requires a clear division of tasks between the hospitalists and nurses when it comes to information provided in the discharge conversation. Nurses often struggle to find out what a patient has been told and what not. This means that communication between hospitalists and nurses when it comes to discharge is insufficient at times. This discrepancy between the disciplines causes patients to experience a poor discharge conversation. In addition, caregivers currently experience a lack of time for discharge. The need for beds is one factor which puts pressure on caregivers to discharge patients quickly.
Finally, the call procedure is not effective as patients are not informed that they will receive a phone call from an anonymous number the next day. Moreover, the patients who received the phone call experienced no added value—if it does not, then they do not need it.
To conclude, a dignified moment of discharge could be created by implementing a standardised discharge conversation. Adequate provision of information is very important for patients to ensure a feeling of closure and reduction of anxiousness. Patients are often not medically knowledgeable, which means that patients often do not know what questions they have until they receive all the information. A standardised discharge conversation with a set order is expected to increase effectiveness of the current discharge procedure. A standardised discharge conversation may also work as a tool to prioritise discharge more for the caregivers. It forces caregivers to take time for discharge and communicate more amongst each other. Communication between caregivers is fundamental for planning this moment of discharge well.
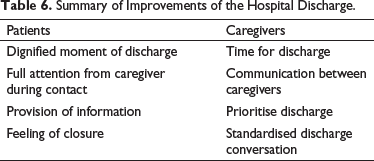
The above underlines the importance of understanding the process of discharge planning and communication from both perspectives, the patients’ and the caregivers’ ones, in order to identify gaps between the two perspectives. Once the gaps are identified in a specific context, it becomes clear what the possible obstacles are and improvements can be made (see Table 6). These findings endorse the critical needs for a better patient experience as described by Meyer (2018), that is, clear goals with regard to the patients’ health, transparent decision-making and, as said before, clear communication. To conclude, it became obvious that the behavioural and relational component in the discharge process, either described as empathy, hospitality or hospitableness, is the pivotal aspect in the perception of both patient and caregivers.
Summary of Improvements of the Hospital Discharge.
This research, however, has several limitations. First, this research is explorative and therefore indicative. It provides insights, most and for all, for the hospital that participated in the research. It revealed that the well-set discharge procedure was not followed, although it was assumed that this would be. Moreover, it disclosed important obstacles in the process. Second, in line with the first limitation, despite the variety of participants, their number is low. Third, the research was conducted at one, Dutch hospital; hence, the results are not generalisable.
While this research has its limitations, it contributes to understanding hospitals’ constraints as amongst others time and occupancy pressures. In addition, it compares the service delivery of hospitals with those of the hospitality industry, in specific with regard to behavioural or relational aspects. It alludes the applicability of hospitality knowledge and experience for the hospital and in general the healthcare industry. Ultimately, it aims to stimulate a more frequent exchange and leverage of synergies between the two industries as recognised by Hollis and Verma (2012).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.