
Abstract
Pandemic-related pressures and responsibilities increase the likelihood of burnout for all health care professionals. The consequences of burnout are significant, as it has been linked to high anxiety, increased turnover, decreased employee morale, higher absenteeism, and lower quality of service. To date, most research explores burnout’s relationship with these variables in isolation. This study explores the anxiety, burnout, and employee engagement relationships among community pharmacists during the global pandemic. Pharmacists in the Canadian province of Saskatchewan completed an online questionnaire that asked questions related to their levels of anxiety, burnout, and work engagement among other control variables. The relationships among the variables were explored via SPSS and the moderation and mediation PROCESS macro. The findings suggest that burnout fully mediates the anxiety and employee engagement relationship, suggesting that anxiety alone is not enough to reduce employee engagement. The results confirm burnout’s relationship with anxiety and lack of engagement and provide a more specific understanding of burnout’s antecedents and consequences, offering important insight for academics and practitioners. Due to the positive implications of eliminating burnout and the importance of employee engagement to organisational performance, managers should seek to reduce workplace stress to avoid burnout and disengagement.
Keywords
Introduction
Like many health care providers, pharmacists experience many workplace stressors, including competing demands and lack of control over their work environment, which can lead to job dissatisfaction, conflict with management, and risk to patient quality of care. Stressors identified by pharmacists include excessive workloads combined with a lack of resources necessary to achieve desired goals and outcomes, as well as an inefficient work environment and the obligation of non-clinical duties (McQuade et al., 2020). Furthermore, community pharmacists must balance their health-care provider role while working in a commercial environment, which can cause role strain and ambiguity (Perepelkin & Dobson, 2010). Increases in job demands and decreases in job resources have been shown to predict burnout (Schaufeli et al., 2009). In some instances, declining profit margins have led to reduced staffing hours; added to this was the global pandemic that resulted in added pressures on pharmacists and amplified health risks (Johnston et al., 2021; Paudyal et al., 2021).
Literature Review
Burnout is described as feelings of emotional exhaustion, depersonalisation or detachment from one’s work priorities, and reduced personal accomplishment (Durham et al., 2018). Accordingly, burnout is defined by high emotional exhaustion and depersonalisation, and a low sense of personal accomplishment (McQuade et al., 2020). Burnout results from an inadequate psychological response to prolonged chronic interpersonal stressors in the workplace (Maslach & Leiter, 2016).
In the 11th Revision of the International Classification of Diseases (ICD-11), burnout is classified as an occupational phenomenon, not as a medical condition, and is characterised by three dimensions, including feelings of energy depletion or exhaustion, increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job, and reduced professional efficacy (World Health Organisation, 2019). Negative consequences of burnout include physical, behavioural, and motivational problems, along with work dissatisfaction (Suñer-Soler et al., 2014). Among health care professionals, factors identified as contributing to burnout include a rapidly changing industry, increased clerical and documentation needs, and the emotionally intense role of patient care (McQuade et al., 2020).
For employers, employee burnout is associated with higher job turnover, lower employee morale, increased absenteeism, and a decline in quality of service (Haase, 2020; Kaluzna et al., 2020; Suñer-Soler et al., 2014). For those receiving services, burnout is linked to increased adverse events and lower patient satisfaction (Haase, 2020; Kaluzna et al., 2020). There is also evidence of a significant association between burnout and depression, as well as burnout and anxiety (Koutsimani et al., 2019). Burnout is a predictor of various negative physical outcomes, including type 2 diabetes, coronary heart disease, headaches, and prolonged fatigue (Salvagioni et al., 2017). Psychological effects of burnout include insomnia and depressive symptoms as well as negative professional outcomes including job dissatisfaction and absenteeism (Hagemann et al., 2020; Salvagioni et al., 2017).
Maslach et al. (2018) describe burnout as a syndrome with three types of feelings: emotional exhaustion, defined by the feeling of being emotionally overextended and exhausted by work; depersonalisation (cynicism), defined by unfeeling and impersonal responses towards recipients of one’s service, care, or treatment; and personal accomplishment (professional efficacy), defined by feelings of competence and successful achievement in one’s work with clients/patients (Maslach et al., 2018).
Many use burnout and stress interchangeably, but burnout is the result of experiencing sustained and persistent, rather than acute, stress (Thomas, 2011). Addressing burnout can increase one’s personal wellness and improve patient safety, satisfaction, and the quality of care provided (Mind Garden, 2018). Furthermore, increases in job resources predict work engagement, and burnout and engagement predict registered sickness duration and frequency, respectively. Work engagement is characterised by a high level of energy and strong identification with one’s work (Schaufeli & Bakker, 2004).
Work engagement is defined as a positive, fulfilling, and satisfying work-related construct characterised by vigour, dedication, and absorption (Schaufeli & Bakker, 2004; Schaufeli et al., 2006). Vigour is defined as a high level of energy and mental resilience while working; dedication is defined as being involved in and finding meaning in one’s work; and absorption is defined as being fully concentrated and engrossed in one’s work (Schaufeli & Bakker, 2004; Schaufeli et al., 2006). According to Schaufeli and Bakker (2004), ‘engaged employees have a sense of energetic and effective connection with their work activities and they see themselves as able to deal well with the demands of their job’ (p. 4). Employee engagement is critical to organisational success (Enright et al., 2015) as it improves employee performance and efficiency (Amerine et al., 2017). Furthermore, engaged employees are more loyal to employers, less likely to miss work, willing to trust and cooperate with colleagues and push through challenges, and be more of a team player by offering constructive feedback (Amerine et al., 2017).
In positive psychology, work engagement is viewed as the antidote to burnout (Schaufeli et al., 2006), where emotional exhaustion and depersonalisation (cynicism) of burnout are the opposite of vigour and dedication in work engagement (Maslach et al., 2001). Employee engagement has been shown to increase when the causes of burnout are removed (Green et al., 2017) and result in lower levels of depression and distress (Schaufeli et al., 2008). However, if an individual scores low on burnout, it does not necessarily indicate that they will then score high on work engagement (Schaufeli & De Witte, 2017).
Despite this dynamic work environment, there is not a good sense of the levels of pharmacist burnout and work engagement. Furthermore, pharmacists are essential workers, and the pandemic increased demand for medications, caused drug shortages, created anxious customers, increased the risk of infection, and amplified workplace stress (Johnston et al., 2021).
The purpose of this study was to explore the relationship between burnout and work engagement among pharmacists. Shortly before data collection was to commence, the COVID-19 pandemic emerged, and items on pandemic anxiety were added to the instrument (see below). In this study, we measured levels of burnout and work engagement to understand whether these two states are complementary or mutually exclusive. The three hypotheses were:
Methodology
Questionnaire Design
Data collected for this study was collected through a self-administered online questionnaire using Qualtrics. The questionnaire was primarily developed by utilising two existing instruments—the Maslach Burnout Inventory (MBI) and the Utrecht Work Engagement Scale (UWES). Questions related to pandemic anxiety were adapted from the work of Matsuishi et al. (2012), which focused on pandemic anxiety during the 2009 H1N1 pandemic.
The MBI was first published in 1981 (Maslach et al., 2018) and is the most widely used and validated instrument for measuring burnout. For this study, the Maslach Burnout Inventory Human Services Survey (MBI-HSS) was utilised; this version of the MBI is designed for professionals in the human services (e.g., pharmacists, nurses, physicians, social workers, etc.) that help people live better lives (Maslach et al., 2018). The MBI is a copyrighted instrument, made up of 22 items that requires a fee for each respondent and only sample questions can be displayed, and therefore data is reported based on the constructs, described above, of Emotional Exhaustion (9 items), Depersonalisation (cynicism) (5 items), and Personal Accomplishment (professional efficacy) (8 items). Examples of items in the MBI include: I feel emotionally drained from my work; I have accomplished many worthwhile things in this job; and I don’t really care what happens to some patients. The UWES is the most widely used, validated instrument to measure engagement and is comprised of 17 items (Schaufeli & Bakker, 2004); from the 17 items come three constructs, described above, of Vigour (6 items), Dedication (5 items), and Absorption (6 items). The three constructs of the UWES can be combined to create a unidimensional construct for work engagement (De Bruin et al., 2013). Examples of items in the UWES include: I am proud of the work that I do; at my job, I am very resilient, mentally; and I am enthusiastic about my job. The three pandemic anxiety items were adapted from the work of Matsuishi et al. (2012). The three questions assessed anxiety about being infected, infecting others, and hesitation to work. The final questionnaire contained 52 items, including respondent demographics and a few questions on childcare responsibilities.
Survey Implementation
The Pharmacy Association of Saskatchewan (PAS), the provincial pharmacy advocacy organisation, and the Canadian Society of Hospital—Saskatchewan Branch (CSHP), the provincial hospital pharmacy advocacy organisation, sent out three emails to pharmacists in the province of Saskatchewan, Canada: the first was a week before data collection began to let potential respondents know they would be asked to fill out an online questionnaire the following week; data collection began a week after the overview email was sent outlining the study and providing pharmacists with a link to the study questionnaire; and the final email was a reminder email 2 weeks after data collection began, with data collection closing 4 weeks after the reminder email. This technique is a modified Tailored Design Method approach (Dillman et al., 2014).
Data was collected from 22nd September to 2nd November 2020. On 15 September 2020, a pre-data collection email was sent to 1,315 pharmacists in Saskatchewan. One week following the introduction email (September 22, 2020), all pharmacists received a request to complete the online questionnaire. On 5 October 2020, 2 weeks following the participation request email, a reminder was sent to pharmacists. Data collection closed on 2 November 2020, and no responses were received after that date.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS) was used to explore descriptive statistics, test the internal reliability of the constructs, examine construct correlations, perform an analysis of variance (ANOVA), and test the delineated hypotheses. Post-hoc mediation tests followed Baron and Kenny’s (1986) testing procedures and were conducted with Hayes’ (2017) PROCESS macro for SPSS.
Results
Response Rate
At the end of data collection, a total of 264 responses were received, yielding a 20.1% (264/1,315) response rate. This response rate was higher than similar studies of Canadian pharmacists (Hussein et al., 2021; Isenor et al., 2018; Jorgenson et al., 2017; Wilson et al., 2020) and exceeded expectations among the population of interest (Hardigan et al., 2016).
Demographic Results
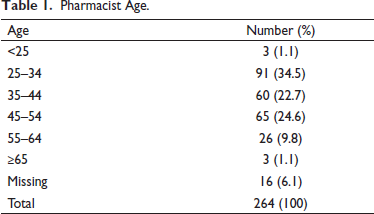
The majority of responding pharmacists were female; specifically, 216 (81.8%) identified as female and 48 (18.2%) identified as male. Most pharmacists were aged 25 to 54 (Table 1).
Pharmacist Age.
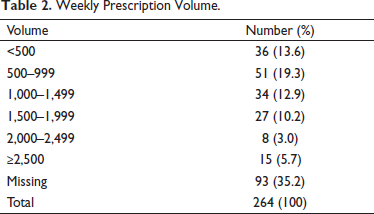
Approximately one-third of respondents (31.8%) required childcare. Of the 264 responding pharmacists, 94 (35.6%) practiced in independent/franchise pharmacies, 85 (32.2%) practiced in chain/grocery pharmacies, 50 (18.9%) practiced in hospital pharmacies, and 35 (13.3%) practiced in other settings or did not report where they practiced. The number of weekly prescriptions ranged from fewer than 500 to greater than 2,500 (Table 2).
Weekly Prescription Volume.
Construct Results
The items of the MBI components were tested for internal reliability. The nine-item emotional exhaustion construct (α = 0.935) and the five-item depersonalisation construct (α = 0.792) showed acceptable internal reliability (George & Mallery, 2019). The eight-item personal accomplishment construct initially showed poor internal consistency (α < 0.50). However, after two items were deleted, personal accomplishment’s internal reliability was acceptable (α = 0.610) (Hinton, 2014). As personal accomplishment is positively connotated, as compared to the negatively connotated emotional exhaustion and depersonalisation, it was reverse coded and renamed inefficacy. Reverse coding personal accomplishment is similar to other work (Leiter & Maslach, 2016). Although the burnout components are conventionally analysed separately, an internal reliability analysis of the final 20 items was undertaken. The results showed acceptable internal consistency (α = 0.903) and an unweighted burnout mean score, consisting of emotional exhaustion, depersonalisation, and inefficacy items, was used in subsequent analyses. Next, the internal reliability of the UWES items was explored. The results showed acceptable reliability (α > 0.600) (Hinton, 2014). However, if one of the absorption items were deleted, Cronbach’s alpha would improve. Accordingly, the item in question was eliminated, resulting in improved internal reliability for the UWES construct (α = 0.743). Based on these results and previous work that has successfully combined the UWES components (DeBruin et al., 2013), an unweighted engagement score was used in subsequent analyses. Internal reliability of the three pandemic anxiety questions (anxiety about being infected, anxiety about infecting others, and hesitation to work) was also tested. The results showed acceptable internal reliability (α = 0.743) (George & Mallery, 2019). As with the other measures, an unweighted mean score of the pandemic anxiety items was created and utilised in all analyses.
Non-response Bias
Non-response bias was tested by comparing anxiety, burnout, and engagement among early and late responders. Responses were deemed early/late if they were completed before/after the reminder message on 5 October 2020. Independent sample t-tests were completed, comparing the anxiety, burnout, and engagement group mean scores among early and late responders. Missing data was treated by means of listwise deletion. There were not any statistically significant differences among the groups’ anxiety (t(253) = 0.780, p = .498), burnout (t(249) = −0.620, p = .606), and engagement (t(178) = 0.155, p = .694) scores. Accordingly, it can be assumed that there was no non-response bias (Armstrong & Overton, 1977; Latif, 2000).
Correlation Analysis and Mean Comparisons
A bivariate correlation analysis of the major constructs (anxiety, burnout, and engagement) and control variables was performed (Table 3). Pharmacist control variables included sex, age, and children. Sex was a dichotomous variable, females (0) or males (1). Age was numeric, ranging from under 25 to over 65. Children were a dichotomous variable, pharmacists who did not have children needing care (0) and those with children needing care (1). The two pharmacy-related control variables were size and type. Pharmacy size was numeric based on average weekly prescriptions filled. For the purpose of the correlation analysis, dichotomous variables were created, distinguishing between non-hospital pharmacies (0) and hospital pharmacies (1). The results of the correlation analysis showed that anxiety was positively and significantly correlated with burnout (β = 0.246, p < .01) and pharmacists with children needing care (β = 0.179, p < .01). Anxiety was negatively and significantly correlated with engagement (β = −0.133, p < .05) and hospital pharmacies (β = −0.127, p < .05). Burnout was negatively and significantly correlated with engagement (β = −0.441, p < .01), males (β = −0.145, p < .05), and hospital pharmacies (β = −0.177, p < .05). With the exception of age and children, all of the control variables were not significantly correlated. Age was negatively and significantly correlated with pharmacists with children needing care (β = −0.154, p < .05).
Correlation Matrix.
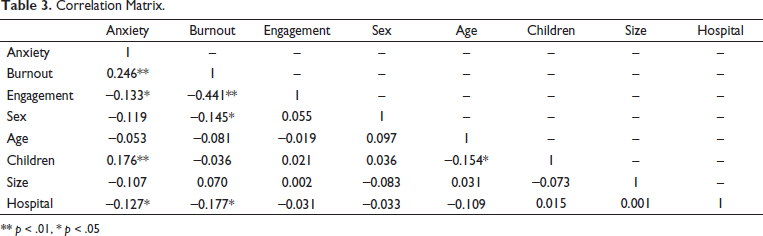
** p < .01, * p < .05
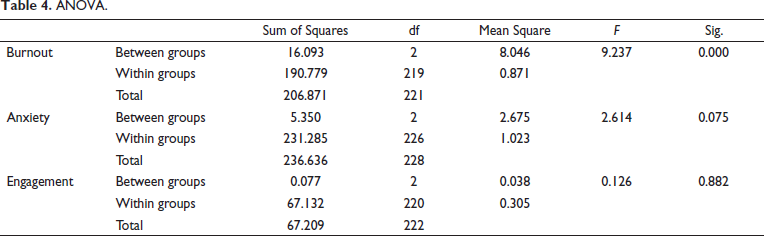
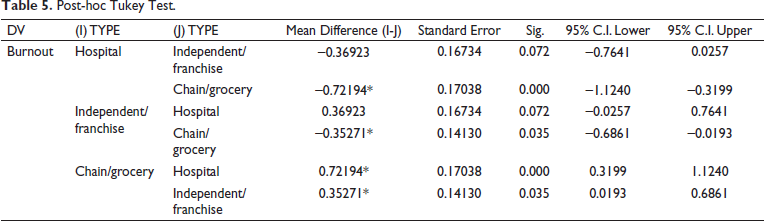
As burnout and engagement were negatively correlated with hospital pharmacies, further investigation of the differences among pharmacy type was undertaken. A one-way ANOVA was conducted to compare the mean burnout, anxiety, and engagement scores among pharmacy types. A statistically significant difference was found among burnout scores (Table 4). Accordingly, post-hoc Tukey’s and Bonferroni’s tests revealed that burnout was significantly higher among chain/grocery pharmacies as compared to hospital pharmacies and independent/franchise pharmacies (Table 5).
ANOVA.
Post-hoc Tukey Test.
Hypothesis Testing
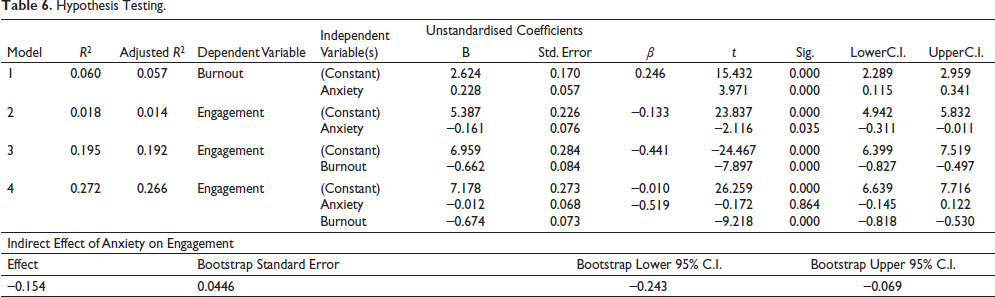
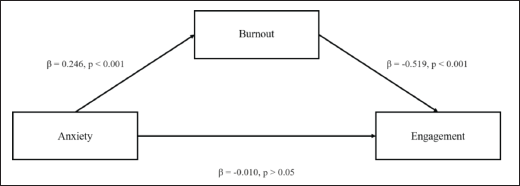
The results of the first regression model that included pandemic anxiety as the independent variable and burnout as the dependent variable were positive and significant (β = 0.246, p < .01), supporting the first hypothesis (Table 6). The second regression model showed that the independent variable anxiety and the dependent variable engagement were negatively and significantly correlated (β = −0.133, p < .05), supporting hypothesis two. The results of the third regression model supported hypothesis three, as the independent variable burnout was negatively and significantly correlated with engagement (β = −0.441, p < .01). In the fourth regression model that included anxiety and burnout as independent variables with engagement as the dependent variable, burnout’s negative and significant correlation with engagement remained but anxiety’s effect on engagement became non-significant. The results of these regression analyses resemble a mediation effect (Figure 1), as described by Baron and Kenny (1986). Specifically, the effect of anxiety on engagement is mediated by burnout. To confirm the mediating role of burnout in the anxiety and engagement relationship, Hayes’s (2017) PROCESS macro for SPSS was used to test the indirect effect. The result of this test showed an effect size of −0.154 with 95% confidence intervals ranging from −0.243 to −0.069. As the 95% confidence intervals did not cross zero, it can be concluded that burnout fully mediated the anxiety and engagement relationship.
Hypothesis Testing.
Mediation Model.
Post-hoc Mediation Tests
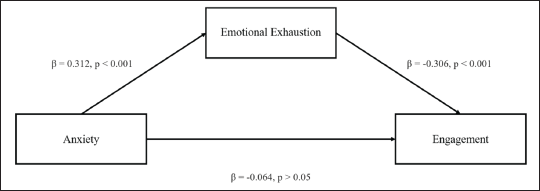
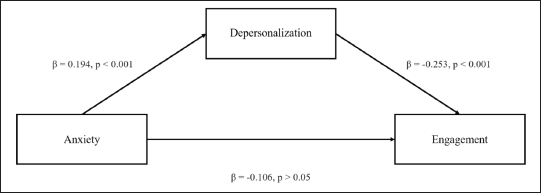
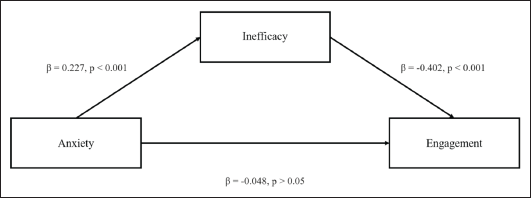
Given the burnout components (emotional exhaustion, depersonalisation, and inefficacy) are typically explored independently, post-hoc regression mediation analyses were performed. The results of all three regression analyses showed that emotional exhaustion (Figure 2), depersonalisation (Figure 3), and inefficacy (Figure 4) fully mediated the anxiety and engagement relationship. Not only did these results resemble those of the burnout model (Figure 1), but they also empirically justify the combination of components to comprehensively measure burnout as they work in unison.
Post-hoc Mediation Model (Emotional Exhaustion).
Post-hoc Mediation Model (Depersonalisation).
Post-hoc Mediation Model (Inefficacy).
Discussion
This study supports previous literature that illustrates the negative implications of burnout (Haase, 2020; Hagemann et al., 2020; Kaluzna et al., 2020; Koutsimani et al., 2019; Salvagioni et al., 2017; Suñer-Soler et al., 2014). Specifically, this study finds that there is a sequential relationship between anxiety, burnout, and lack of engagement. This article, through a series of mediation tests, shows that pandemic-induced anxiety alone is not enough to pose negative organisational consequences, such as lack of engagement. Instead, lack of engagement only occurs in the presence of burnout. This is congruent with previous research that separately shows the positive relationship between anxiety and burnout (Koutsimani et al., 2019) and the relationship between burnout and unfavourable organisational consequences (Haase, 2020; Hagemann et al., 2020; Kaluzna et al., 2020; Salvagioni et al., 2017;Suñer-Soler et al., 2014). However, this article offers novel insight into the exact interplay between anxiety, burnout, and lack of engagement. Given the favourable consequences of reducing and eliminating burnout (Green et al., 2017) and the importance of employee engagement to organisational performance (Enright et al., 2015), such actions to reduce burnout should be the new community pharmacy strategic imperative.
This study suggests that burnout is higher among female pharmacists, those with children needing care, and those working in chain/grocery pharmacies. Interestingly, this study’s finding that females experience higher levels of burnout as opposed to their male counterparts, contrasts recent pandemic research (Jang et al., 2021). Future research should explore why these differences exist in some contexts and not in others. It is not surprising that pharmacists with children requiring care were more likely to report higher levels of burnout, as other studies have reported similar findings (Griffith, 2020; Öngören, 2021). Data from this study also shows that chain/grocery store pharmacies have higher rates of burnout compared to hospital and independent/franchise pharmacies and may indicate that the work environment in chain/grocery store pharmacies is more conducive to burnout and less likely to have engaged employees. Such insight offers a starting point for pharmacy managers seeking to reduce burnout and improve organisational performance in an increasingly dynamic and complex health care environment. Strategies to mitigate burnout among pharmacists are likely to increase professional performance such as patient care (Mind Garden, 2018). According to Wilson et al. (2020), strategies to enhance the professional objectives of community pharmacy have favourable financial performance implications. As such, to improve the professional and commercial objectives of community pharmacy, management should look to enhance the work environment by reducing anxiety and burnout.
This article contributes to burnout literature in several ways. First, it confirms burnout’s relationship with anxiety and lack of engagement. Second, examining anxiety and engagement simultaneously, allows for a more specific understanding of burnout’s antecedents and consequences, providing important insight for academics and practitioners. Finally, the article is novel as it successfully combines the burnout components in a unidimensional construct. As burnout is not usually measured using an unweighted mean score, its components were retested as mediating variables in the anxiety and engagement relationship via three separate models. The results showed that emotional exhaustion, depersonalisation, and inefficacy fully mediate the anxiety and engagement relationship. The replicable nature of the results validated the use of a unidimensional burnout measure to be used in future research.
Limitations
As with any research, there are limitations, and therefore the findings should be approached with some caution. This study was conducted in one province (Saskatchewan), in one country (Canada), and therefore may not be applicable, nor generalisable, to other jurisdictions. Due to the self-reporting methodology utilised in this study, there is the possibility of respondent bias. Furthermore, data collection occurred in the fall of 2020, just as the second wave of the COVID-19 pandemic was beginning in Canada, and therefore respondents may not have been thinking and remembering clearly due to the added demands and stress on them at the time of responding; furthermore, due to the increasing demands and stress potential respondents may not have responded due to other, more pressing priorities. As with any survey research, there is the potential for nonresponse bias; a non-responder survey was not conducted, but early versus late responder analysis was completed (see above).
Conclusion
Traditionally, methods used to overcome burnout have focused on the individual as opposed to the job situation or environment (Maslach, 2017). Instead of placing the onus for burnout recovery on the individual employee, it may be time to place the onus on employers to create a work environment that engages employees and therefore decreases the chances of burnout and increases the chances of higher productivity, with fewer errors and decreased employee turnover. Furthermore, the MBI and UWES have been used to predict mental health issues that result in long-term sickness and suggest that they can be used to identify employees for a further mental health assessment (Roelen et al., 2015). Therefore, there are arguments for assessing employee burnout and work engagement in an effort to be proactive in addressing the potential negative consequences, for employees, employers, and clients, of employees that are, or are approaching, being burnt out and/or lack engagement in their work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was supported by a Social Science and Humanities Research Council of Canada (SSHRC) Explore Research Grant.