
Abstract
When one talks about a healthcare organisation, in most instances it is an automatic assumption that we are talking about clinical personnel. This article addresses the critical role that non-clinical personnel played during the COVID-19 pandemic. In particular, the authors delineated the critical roles of the marketing department personnel in healthcare organisations. In light of the pandemic, in the future, there will be a greater need for unique training topics that were not even imagined in the years prior to 2020, and using the concepts of marketing, the authors have provided a list of the potential generic topics as well as how to assess its reach, effectiveness and value.
Introduction
There is no doubt that the clinicians in healthcare organisations around the world are true heroes who have risked their lives to make sure other survive during the COVID-19 pandemic. The authors join the whole world in saluting the doctors, nurses and other clinicians who played a direct role under very challenging situations at times during this pandemic. Numerous cases have been written showcasing the clinicians, and they deserve to be acknowledged. This article, on the other hand, provides a deep sense of appreciation to another group of professionals who also work in healthcare organisations, not as a direct patient care provider, but as non-clinician administrators. It also provides some recommendations for leaders of healthcare organisations to plan for and/or make ‘managerial’ decisions, and it does not in any way promote interference in clinical decision-making processes. Doctors, nurses, and other direct patient care healthcare clinicians should always be regarded as the individuals who will make the most appropriate decision regarding the care and treatment of COVID-19 patients. Studies conducted on a global scale have already been published regarding establishing appropriate clinical guidelines and/or protocols for treating COVID-19 (Alhazzani et al., 2020; Li et al., 2020; Reusken et al., 2020). However, despite extensive efforts, the authors were not able to find many studies addressing the evolving roles of healthcare leaders and other non-direct patient care employees of healthcare organisations.
The healthcare executives, directors, patient advocates and other non-clinical professionals, who work in the background, have to work and provide tools, policies and procedures to assist the clinicians in providing quality healthcare to patients. COVID-19 is a very new challenge that has been thrusted upon the healthcare industry with no regard to any nations or boarders or religion or any other demographic variable.
This new challenge is so dynamic and changes so frequently that healthcare leaders are trying to catch up with new policies and procedures to get a handle on it. In many countries, there is a complete lockdown, which in turn has created new challenges for healthcare organisations to distinguish between essential and non-essential personnel. Obviously, the clinical professionals are essential personnel, but it does not mean that several non-direct patient care employees in a healthcare organisation are not.
Role of Non-Clinicians During the Covid-19 Pandemic
Though most of the reports that are broadcast or printed in the news media during the initial stages are related to clinical information, morbidity and mortality, there have been few reports regarding the critical roles played by organisational leaders, such as executives, directors, administrators and so on, who are often non-clinical healthcare management professionals. The commendable roles played by these organisational leaders, particularly in many organisations in the United States, are by individuals who have educational backgrounds in the management aspect of healthcare organisations, with graduate degrees in fields such as healthcare administration, hospital administration, business administration, public health, to name a few. On the other hand, in India, the Principal Secretary (Health), and District Magistrate, and Collector, some of who come from the Indian Administrative Services (IAS), played a key role during the COVID pandemic. Apart from these public administration officials, the police also played a key role in implementing and enforcing lockdown throughout India.
Individuals with undergraduate degrees in these or similar non-clinical fields also played critical roles in lower level positions, such as in the accounting, human resources, front office, reception and so on. Needless to say, the level of strategic planning, organisation, coordination, marketing, public relations, communication, community outreach, and other non-clinical activities that helped healthcare organisations during the COVID-19 pandemic has given greater value and credence to the field of healthcare administration. This field is still in developmental stages in most parts of the world, but fortunately it is well established in many countries whose educational programmes and values are highly regarded.
Critical Roles That the Healthcare Organisation’s Marketing Departments Play During the Pandemic
Unfortunately, the fact is that many times, the term ‘marketing’, in the healthcare field in particular, is considered unethical and with many other unflattering terms. This is far from the truth and an underappreciation of what marketing does and can do for the greater good of the stakeholders, including the patients and providers. Perhaps the most critical job for a marketing department in any healthcare organisation is to provide appropriate communication, and this is even more imperative during the COVID-19 pandemic. A brief list and examples of some of the various activities that the marketing department in a healthcare organisation during COVID-19 can do for different parties are as follows:
Develop a message or tool of communication which is not scary and fearful, but more compassionate and reassuring. This is quite done in the form of a public service announcement and delivered by the public relations officer or offices; Develop surveys specifically related to issues around the pandemic, such as patient satisfaction survey or even an employee satisfaction survey. These should be specific to the issues and challenges related to the pandemic, many of which were not even being thought of prior to the year 2020; Develop a tool so as to simplify a communication between a COVID patient in a hospital and their loved ones who may not even be able to visit them during the time that they would really like to see a familiar face. The marketing department can help generate an app or a pictorial flip chart that can easily communicate the message without causing the stress of reading or writing too much.
There is no doubt that once things settle down and clinicians have a greater control over COVID-19, there will be a tremendous amount of fatigue, burnout, and emotional impact on clinical as well as non-clinical health professionals who were day in and day out engaged in providing care to COVID-19 patients (Bromley, 2020; Hartzband & Groopman, 2020; Peinado & Anderson, 2020). The organisational leadership should pay special attention in identifying these impacts on different individuals, or even groups of individuals (such as ‘ICU nurses’) and then devise a plan to address them (Charney et al., 2020; Shen et al., 2020).
Not all individuals will need the same plan of action, but a plan of action should be ready for all. For example, ICU nurses who saw a disproportionate amount of deaths related to COVID-19 may need counselling and no matter what people say, they also do grieve (Shen et al., 2020).
Strategies for Healthcare Organisations When Getting Back to the ‘New’ Normal
The new normal in healthcare organisation definitely will have to do with ‘social distancing’. However, despite all our best intentions, it is very likely that once the pandemic numbers start going down, there will be a lack of adherence to this policy. In hospitals, some of the strategies to implement social distancing are listed below:
Protecting your own employees: COVID-19 has no doubt created fears among the healthcare organisation employees. Hospital or even standalone emergency rooms are obviously going to be the place where patients are going to be brought in particularly if they are perceived by first responders or family that they are in need for emergency care. Whether these patients are infected with COVID-19 or not, now the most common assumption is going to be that the patient is infected. Hence, these healthcare organisations should have a plan of action in place to protect the emergency room employees, both clinical and non-clinical, from getting infected (Jalili, 2020). Redesigning the patient waiting area: One way can be of having multiple registration windows with squares about 6 feet apart for people to stand in prior to reaching the registration window. However, it may not be practical in most organisations because having such gaps requires giving up ‘valuable real estate’ in a hospital. Better patient scheduling: Hospitals will have to come up with better scheduling of patient appointments so that not many congregate in the waiting area at the same time. Appropriate scheduling is already being done in many hospitals; however, with the new social distancing norm, it is highly likely that hospitals and clinics may reduce the number of patients that they schedule per hour. The downside of this is that people may start seeing their appointment time pushed back more than the desired. Greater utilisation of PPEs in healthcare organisations: The Centers for Disease Control and Prevention in the United States has stated that COVID-19 created tremendous challenges for the healthcare organisation due to the shortage of personal protective equipment (PPE) (CDC-1, 2020). Among the various PPEs recommended by the CDC, the demand and use of three specific types of PPEs—eye protection, isolations gowns and facemasks—will definitely be greater in the near future. Facemask will perhaps be in the greatest use among non-clinical employees in the healthcare organisations. Providing masks to patients and visitors: For the near future, there is going to greater reluctance among patients who visit hospitals and clinics to be in close proximity to individuals who are coughing and sneezing as they may be perceived as contagious and infected with COVID-19. Hence, it is imperative for these healthcare entities to try to mitigate the situation to a certain degree by giving out masks, scarves or other similar face coverings, and encouraging individuals to use them. Now granted, these masks were not a budget item in the past for healthcare organisations; they can actually still get something back in return, like by having information of the institution printed on it, such as the logo, name, address, website and so on. This can become a tremendous marketing opportunity as well for these organisations. The reality is that there are going to be new expenses which will have significant financial implications on organisations. The marketing of the organisations on items such as masks do have the potential of providing long-term value and recognition for the organisation. Greater presence of hand sanitisers: Now that people are more aware of hand sanitisers in most parts of the work, individuals working in, or visiting as a patient/guest, a healthcare entity such as a hospital, clinic, doctor’s office, to name a few, will be expecting easily locatable hand sanitiser dispensers. Hand sanitisers are not inexpensive; therefore, the costs of these products should now be incorporated in the budgets of the entities. The presence and easy availability of these products in healthcare entities has the potential to indirectly positively promote the organisations. More billboards/flyers/brochures promoting practising social distancing and personal hygiene: In the near future, it can be assumed that there will be greater presence of public health–oriented marketing efforts worldwide related to social distancing, personal protections by way of masks, and encouraging practice of cleanliness. These marketing efforts will definitely be one of the major tasks for local/state/national government public health agencies, as well as by public and private healthcare organisations. New biohazard disposal containers for used PPEs: Traditionally, masks and gloves were used by health professionals in healthcare organisations, and they were appropriately disposed of in properly identified biohazard containers. Now that there will be a greater use of masks and gloves by the community at large, it is imperative that they are informed and educated about proper ways of disposing of these PPEs. It will be irresponsible for the consumer to just discard the PPEs in public, or outside the hospital after a visit, because not only will it create trash but more importantly it may result in spreading of the disease. Studies have indicated that improper disposal of PPEs, such as gloves, can lead to environmental contamination (Munoz-Gutierrez et al., 2019). In the beginning, the most effective utilisation of the biohazard disposal containers by non-healthcare individuals can only happen if they are educated about it, made aware of it and sadly even monitored that the individuals properly dispose their PPEs in those containers.
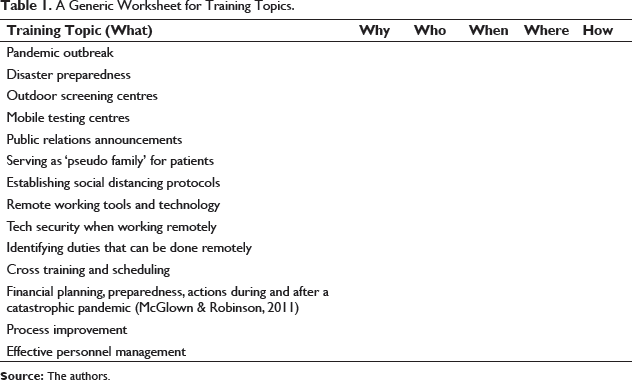
A Brief List of Some Future Training Programmes for ‘Non-Clinicians’ for Healthcare Organisations
A Generic Worksheet for Training Topics.
Needs and Strategies for Healthcare Organisation to Play a Greater ‘Societal’ Role
Now is the time for healthcare organisations to start planning for the future, in particular how can they serve a larger community on a national or international scale, when the healthcare needs of the society at large are greater than the community that they are designed and developed to serve. These are the tasks that non-clinical and/or non-direct patient care providers in healthcare organisations should be engaged in. These are the individuals who will be looking at the organisations viability more so from the ‘business’ aspect and less from the clinical aspect. Healthcare organisation leaders will have to make critical decisions on whether they want or not want to participate in addressing such pandemics if and when they arise in the future. Despite all their good intensions, it is up to the organisations to do an honest assessment of their organisation and whether they will be able to make a contribution or not. Realistically, a majority of the healthcare entities, such as small hospitals and clinics, may not have the capacity or capability to contribute.
One of the biggest challenges was shortages of health professionals, particularly doctors and nurses, in some hard-hit cities across the globe. Many doctors and nurses in the United States left their place of employment and worked as a ‘travelling doctor or nurse’. The primary reason for this for most of these healthcare professionals had more to do with their being a healthcare professional first. At the same time, these travelling healthcare professionals, particularly nurses, were also paid decently for their services. Nurses could easily make more than $100,000 per year as a travelling nurse, and even higher during this pandemic (Walker, 2020).
This pandemic has no doubt re-emphasised that there is a greater need to have global strategic plans in place to address such an outbreak. Below are some strategies to address appropriation of health professionals in a more effective and efficient manner:
A national database of volunteer nurses and doctors: There are already several healthcare-related databases that exist for volunteers, such as for bone marrow donation. A similar volunteer database should be established in all countries where doctors and nurses are asked sign up to be volunteers in case of a pandemic. Of course not all volunteers will be able to go when a need arises, but at least there is a central database which can be quickly tapped into when the need arises. A comprehensive questionnaire should be created for volunteers so that only the appropriate health professionals are contacted. For example, during the COVID-19 crises, there is a greater need for emergency room physician or nurse as compared to a surgeon or a transplant nurse. An international volunteer database: Similar to the strategy mentioned above for national databases, an international database should also be established. However, in doing so, there is a great need for collaboration among nations, for example having provisions such as covering expenses of healthcare providers who are temporarily relocated to a host country for delivering care. When pandemic such as COVID-19 happens, that is not the time for governments to decide between saving a life versus saving money. Increased telemedicine utilisation and subsequent reimbursement issues: Almost a couple of decades ago, authors Chandra and Cheek had suggested how the international healthcare market was emerging and had proposed strategies for improving healthcare delivery through telemedicine (Chandra & Cheek, 2001; Cheek & Chandra, 2002). Over the past decade, use of telemedicine has seen a significant growth. With such growth, it has also created new opportunities for healthcare providers by increasing their market reach, but has also created challenges for these providers particularly when it comes to reimbursements. Fortunately, there has been a greater recognition of the value of telemedicine and its cost-effectiveness, thereby providing more reimbursement opportunities for telehealth providers (Lacktman, 2016). Flexibility in providing temporary licensure waivers/reciprocity for health professionals: One of the great challenges with telemedicine will be for different states and nations to remove some of the licensure-related barriers. Providers based in different states and/or countries should be given at least a temporary licensure waiver as a reciprocity if a professional is licensed with certain approved organisations or boards (Chandra et al., 2005). Healthcare organisation’s internal database of ‘travelling health professionals’: Organisations should create an internal database of health professionals who are willing to go to the frontlines or remote locations in case of a pandemic or emergency. The database should be frequently updated because over time the desires of individuals change. Organisations should be careful in who they are willing to accept as a member of the travelling health professional pool. A simple questionnaire can be developed by the marketing or human resources departments of healthcare organisations that can be distributed to clinicians after they have been with the organisation for at least a year. The reason of recommending a year is that when these individuals go out to the community they are ambassadors of the organisation. Most organisations will know by the end of a year of employment the capabilities of their employees. Develop health professional employment protection policies and procedures: The COVID-19 pandemic has brought to light the great sacrifice and willingness of health professionals to go to the frontlines, just like a soldier would during wartime. This is a type of war that is being fought against an invisible enemy by highly trained professionals. Many organisations, particularly in the United States, have provisions, policies, and procedures in place whereby they do not come in the way of a soldier to decide whether to go for a war to serve the nation or skip it and save their job. Why can’t a similar concept be designed and developed by healthcare organisations whereby they will not get in the way of a healthcare professional who is willing to go to the ‘pandemic warfront’? Health professional contributions to ‘vacation hour pool’: Granted that not all health professionals can be ideal ‘soldier’ to go to the frontlines at the time of a pandemic. It could be due to a whole range of reasons, from the lack of need for their specialty to their physical disability or even their willingness to go to the frontlines. But this does not mean they may not want to contribute. Organisations can establish a ‘vacation hour pool’ within their entity whereby clinicians can ‘donate’ their vacation days that can accumulate over time and be used by travelling healthcare professionals when going to the frontlines of medical needs of distant communities. This way, a volunteer will not have to take their own personal vacation time or paid/unpaid time off. Telecommuting support for non-essential personnel: Healthcare organisations should now work on establishing a list of jobs and personnel who can telecommute and work from home. Having this strategy in place can be used not only when there is a pandemic but also when there may be a disaster, natural or manmade, that can cause physical or mental distress for these employees if they had to come to their place of employment. Obviously, there are costs that these organisations should start budgeting for, such as laptops, reliable internet, and so on (Regional News, 2020). Develop simulation tools for future pandemic: There are numerous management simulation tools that are used in businesses these days. Many of these are also used to train MBA students worldwide. Now it is time for healthcare leaders to start thinking outside the box and run simulations for different types of real and even hypothetical pandemic scenarios. The best-case scenario would be that these scenarios never happen, but just in case they do, the leaders have an idea of how to get started and not start to plan when the pandemic is growing. They can even generate distribution models for healthcare-related products and services not only across their organisations but also across regional, national and even international boundaries.
Conclusion
The COVID-19 pandemic is no doubt a sobering reminder to all how fragile the healthcare industry is and that the leaders in these industries need to think of all kinds of scenarios including issues of new roles for its variety of non-clinical personnel and departments. The year 2020 can also be considered as a year where employees got to learn new tools and techniques not by using simulation models but rather facing it on a real time bases. Organisations, its personnel, and leaders who did not fray away from this pandemic but instead performed more than what was expected of them should be recognised, and once this pandemic is over, should also be appreciated. It should also be a sobering reminder to entities external to healthcare organisation that these organisations should not be taken for granted and that even these organisations have their limitations of they can or cannot do. In these trying times, it is imperative that everyone shows some empathy, respect for each other, and follow the appropriate recommendations of health professionals and public health agencies who are also tackling a pandemic beyond the expectations of most the population.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.