
Abstract
Healthcare establishments are unique and complex. The Indian healthcare system comprises of public and private healthcare establishments. Different challenges are encountered by the healthcare professionals in their daily operations. The sudden emergence of COVID-19 posed a new threat to the already burdened healthcare system. The pandemic changed the healthcare paradox with newer workplace and societal challenges faced by the healthcare personnel. The purpose of this study is to identify the antecedents of workplace and societal challenges faced by the healthcare personnel.
Our study conducted in Kolkata and other adjoining areas of West Bengal included respondents who volunteered for individual in-depth interviews. The sample size was kept at n = 20 after due technical considerations. Freelisting and pile sorting was done to generate clusters.
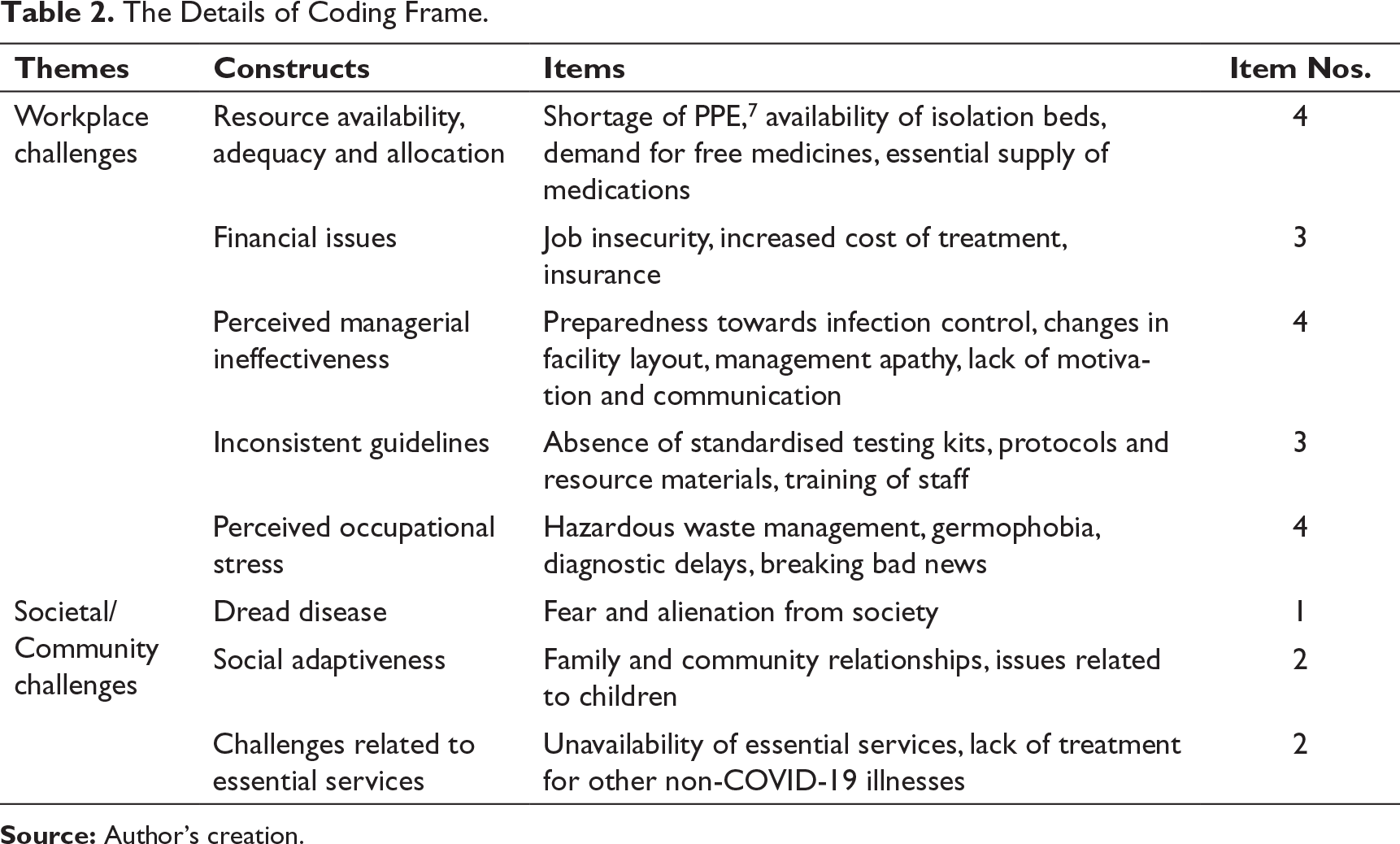
The qualitative study identified five constructs with 18 items under workplace challenges and three constructs with five items under societal/community challenges. Workplace challenges included resource availability, adequacy and allocation, financial issues, perceived managerial ineffectiveness, inconsistent guidelines and perceived occupational stress, while societal/community challenges included dread disease, social adaptiveness and challenges related to essential services. A salience threshold was established and the multidimensional scaling provided four major clusters: financial support and sustainability, adaptive resilience, infection risk mitigation and healthcare facility preparedness.
Suggestive actions for the identified challenges were summed as enhanced production of diagnostic kits through public–private partnership models and industrial production reforms. Enhanced testing facility for COVID-19 will help to identify new cases. Financial stresses need long-term sustainable alternative that will avoid pay cuts and unemployment. Treatment regimen, diagnostic protocols, waste disposal guidelines should be worked upon and leading national agencies be consulted for technical support, research and development.
Life will never be the same either professionally or personally. [‘The great realization’—Tomos Robertson aka Tom Foolery]
Introduction
The healthcare organisations are evolving to adapt to shifts pertaining to demography, epidemiology and societal mindsets that are emerging in the backdrop of several contexts, challenges and uncertainties. The divergent infrastructure needed by the healthcare personnel include physicians, clinicians, nurses, paramedics, practitioners, administrative staff, managers and leaders to respond to various ongoing and contemporary issues remain unclear or not effectively understood. The global health has become even more complex as a result of various technological, social, political and environmental developments and practicalities.
The significant shortage of skilled human capital in healthcare for addressing the health needs of the current and emerging population across the world has been identified by World Health Organization (WHO, 2006). Though, there have been some developments and improvements in global health workforce, still there are remarkable differences due to varied individualised healthcare challenges of the different health systems.
The numerical shortage of human capital is one common challenge, however, the notable differentiation in skill mix, uneven distribution of human healthcare capital across geography, strenuous inter-professional collaborations, injudicious use of resources and burnout variations vary across nations (Figueroa et al., 2019). The studies conducted till date are largely country or region specific and have not been integrated from the multidimensional or international insight since a single defining global healthcare system is lacking (WHO, 2018).
The Indian healthcare sector provides a contrasting landscape in the spectrum of healthcare activities. On the one side, there are well-built glass and chrome structures that are state of the art with advanced medical aid that is always ready to welcome and provide service to the patients, though only a thin section of the population can afford it. On the other side, there are public health centres with average infrastructure, which still serve patients and attempt to identify as a healthcare facility though desperately looks forward to a face lift and transformation.
The Indian healthcare system is categorised into two main types based on the mode of deliverance (Kumar & Prakash, 2011). Public healthcare covers about 18% of total OPD 1 and approximately 44% of total IPD 2 (Thayyil & Jeeja, 2013). It is subsidised and largely free for those below the poverty line. The private healthcare has strengthened its foundation in the last two decades acting as healthcare provider for the 70% households located in urban India and 63% in rural India (International Institute for Population Sciences, 2007). It consists of approximately 58% hospitals in the country with 29% beds covering different hospital types with 81% on-roll doctors (NHM task report). The various causes of differentiation in these two systems are ascribed to poor quality of care in public health, long waiting time, timing issues and long queues for subsidised or free diagnostic/surgical procedures (Bajpai, 2014). It is one of the leading reasons for burgeoning of various private healthcare facilities.
The Indian out of pocket (OOP) expenditure model provides various options and opportunities to a certain class with its advantages, faults and limitations (Barik & Thorat, 2015). Most importantly, these ‘faults’ are largely identified and highlighted by the negative media reports, individual perceptions, public trials, social media judgments and disputes between different individuals, systems and agencies. The end reaction are instances of masses destroying hospital facilities, attacking healthcare personnel, especially doctors and frontline staff being lynched and growing mistrust between different stake holders. To negate such situations, legal frameworks and policies have been enforced by different central and state government agencies.
With the sudden coronavirus disease (COVID-19), the world became standstill and united to address the common challenge encountered by countries across varied population, sizes and economic capacities. The infection rates and disease spread was too high. WHO 3 declared a public health emergency and global pandemic. India declared complete lockdown from the midnight of 24th of March 2020 (Pulla, 2020). Globally COVID-19 positive cases and deaths have exponentially increased, urging the countries to declare lockdown. As per MOHFW, 4 Government of India, there are approximately 742,023 active cases in India and 61,529 deaths as on 28 August 2020 (GOI, 2020). The official records could be lower than actual statistics, due to low testing rates compared to other developed countries (Editorial: The Lancet, 2020). These numbers are undergoing rapid changes and the trend is unfortunately rising.
This crisis completely changed the healthcare paradox and pushed the doctors, their teams and other frontline medical personnel to become the torch bearers. With the declaration of coronavirus disease a pandemic, the government and public enthused medical and paramedical healthcare workers, identified them as frontline forces and named ‘corona warriors’ (Pandey & Sharma, 2020). Motivations through moral boosting using broadcast, showering of flowers on doctors/healthcare personnel and designating them as corona warriors were successful; however, the real battle was about to unfold.
Warriors, like any other ordinary countrymen, have concerns with enemies, especially that are unseen (microscopic minuscule), inadequacy and under preparedness (lack of essential resources like preventive medicines: hydroxychloroquine [under review], protective shields, etc.), absence of a standardised treatment protocol and expensive confirmatory tests like RT-PCR, 5 the declaration of pandemic overthrew the already burdened healthcare system. There was sudden requirement of molecular laboratories to conduct RT-PCR tests requiring trained manpower alongside budget for covering costs (Mitra, 2020). Initially, procuring standardised kits from national and international manufacturers became challengeable. Costs apart the technicalities, validation, performance and end results required expert interpretation and medical acceptance, and since then things suddenly turned hostile for everyone.
The healthcare personnel were taking severe blows on their individual lives, family, relationships and mental health. Different societal attributes such as avoidance, home confinement, stress, work-life balance and increased expenses were experienced.
This article has attempted to document the perception of the Indian healthcare personnel—physicians, nurses, hospital managers, paramedical staff and frontline workers and their challenges on-duty and beyond during COVID-19 pandemic. The primary aim of this article is to identify the challenges of healthcare personnel during COVID-19 pandemic and suggest actions for possible mitigation.
Methodology
Study Approach
This study utilised a mixed approach, consisting of qualitative analysis (in-depth interview) and quantitative visualisation of qualitative data (freelisting and pile sorting). Prior to the main study, a pilot study was conducted with 50 healthcare personnel, working at public and private healthcare hospitals in West Bengal. This pilot study was conducted to validate the different items listed in extant literature and find out if there are new items in line with the objectives of current research. The different factors/challenges suggested by the respondents during the pilot survey included ‘workplace settings’, ‘community/neighbourhood settings’, ‘health status of patient before entry to healthcare facility (HCF)’, ‘during the course of treatment’, ‘breaking bad news (BBN)’ and ‘communication on death’.
Study Respondents
The data collection occurred in February–April 2020 after taking prior approval from the respondents. This study was given the ethical approval from the institutional ethical committee. The sample size for the present study was kept at 20 as justified by many existing studies (Marshall et al., 2013). Respondents were individually interviewed (IDI; in-depth interviews).
Data Collection and Analysis
Socio Demographic Characteristics of Participants.
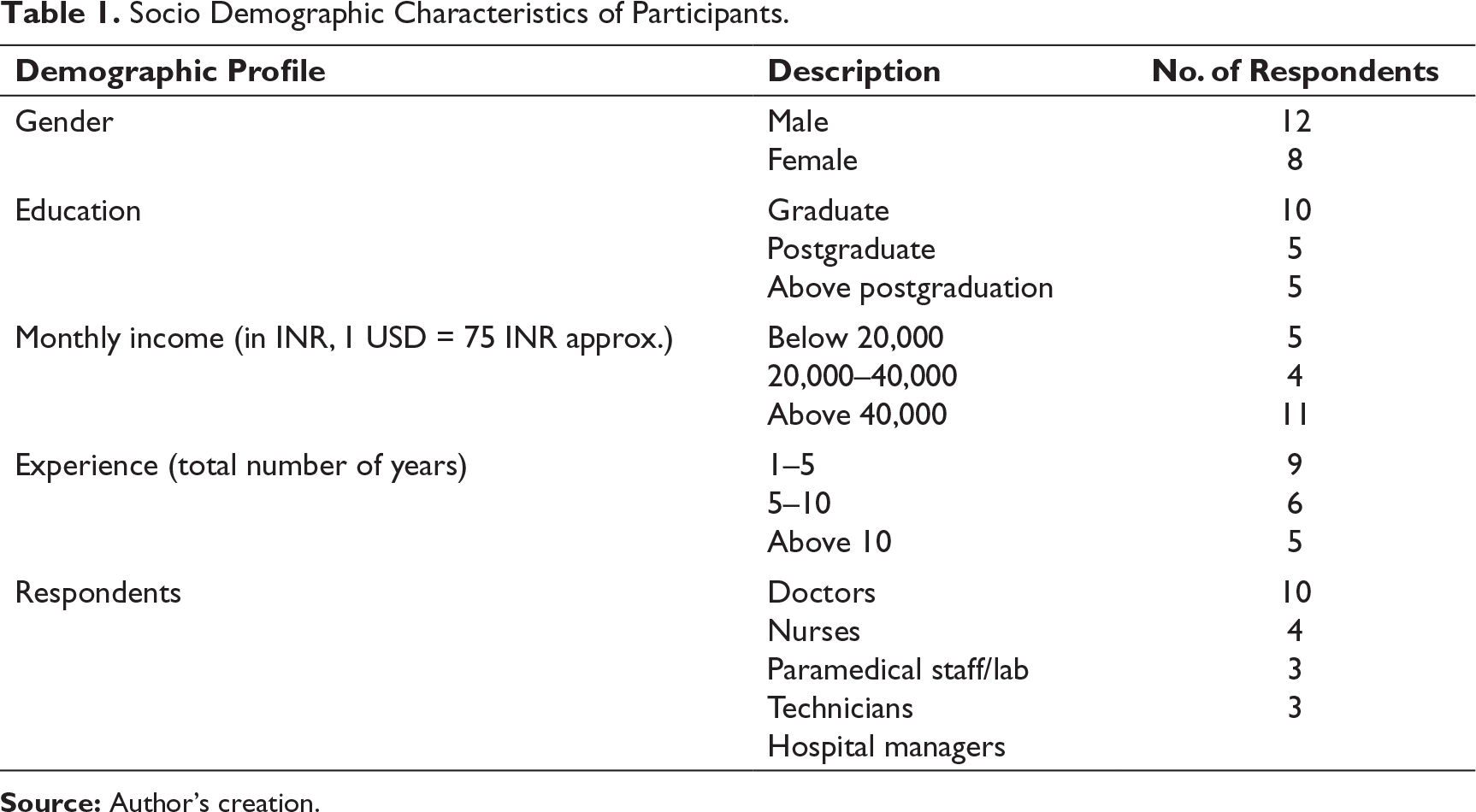
Socio Demographic Characteristics of Participants.
A semi-structured questionnaire was constructed based on pilot survey items to determine challenges faced by healthcare personnel (doctors, nurses, paramedical staff and all other healthcare workers) in this COVID-19 pandemic (Appendix 2). Before the actual interview, all the respondents were given prior knowledge regarding the topic (Sengupta et al., 2019). This was done for rapport building and to make them feel comfortable.
The interview was done using above questionnaire, recorded and transcribed verbatim. Purposive sampling technique was used. Since the respondents spoke in English and vernaculars, the transcripts were subjected to back-translation and were cross-checked and tallied by the researchers to keep the meanings unchanged (Baishya & Samalia, 2020). The audio tapes and field notes were heard and read multiple times for familiarisation with issues that were highlighted.
A coding manual was made based on the responses. The authors did the coding independently and separately and matched the data with another independent coder and fine-tuned until the explanations and relationships could be established.
The quantitative analyses of the qualitative data are commonly done using freelisting and pile sorting methods that exhibit visually reflective results (Smith & Borgatti, 1997). The workplace challenges during COVID-19 were identified through freelisting and pile sorting (n = 12).
The perceived challenges were identified by individual respondents and freelists were prepared in order of priority. The research team reviewed the freelists and standardised word forms and also combined synonyms. The specific domains grouped both positive and negative comments. For instance, ‘unavailability of medicines’ and ‘shortage of medicines and essentials like PPE 6 ’ were grouped under resource availability, adequacy and allocation.
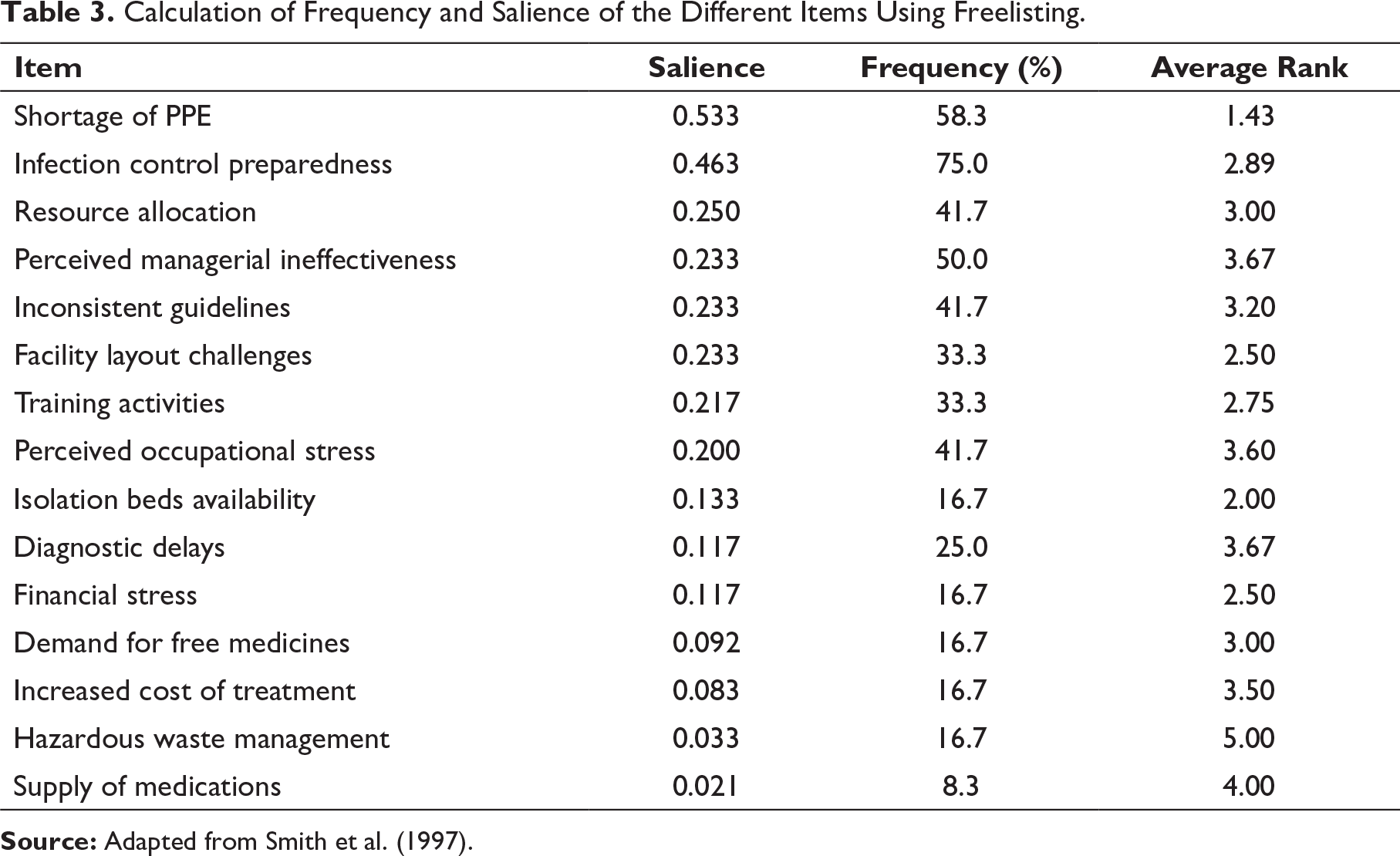
The analysis of freelists was done using Anthropac, version 4.983 (Analytic technologies, Kentucky). The output for the workplace challenges was reviewed to identify words that were most salient for healthcare personnel. The derivation of salience utilised Smith’s salience index, that is, S = ((L Rj + 1)/L)/N, where L denotes each list length, Rj denotes item J’s rank in the list, and N denotes total number of lists in the sample (Fiks et al., 2011). Salience indicates those terms that serve as constructs for a particular domain and take into account frequency and the order of words. The salient scores have been plotted and a natural breaking point was selected with high to low salience scores on the axis (Schrauf & Sanchez, 2008).
As the words became less frequent, the slope got flattened. Those words that were above the breaking point were considered salient. The respondents sorted the freelists and identified items of pile sorting (Yeh et al., 2014). Each pile named by the respondents was further compiled into spreadsheet. Once this was done, two researchers from the team independently went through the list of pile names, and a consensus was reached for appropriate cluster name. A cluster map was thus created for the respondents, using the ranged list of workplace challenges gathered from interviews (IDIs) and freelisting data.
Results and Discussion
The Details of Coding Frame.
Workplace Challenges
Resource Availability, Allocation and Adequacy
Resource refers to all physical, infrastructural and human capital entities. The Indian health sector is resource scarce. The gross mismatch in resource availability and allocation is of great concern. The healthcare expenditure is about 3.66% (2016) of the GDP (Bhukta & Patra, 2019). Allocation becomes a major issue when resources are limited and the demand exceeds supply, thereby creating competition and power games (Kluge, 2007). This is conventionally one of the leading healthcare challenges where there are lack of resources to apply the policies and schemes to actual practice. To ensure resource optimisation, the government hospitals charge a subsidised user fee from everyone barring a section of people that are below the poverty line (Kurian et al., 2011).
In this COVID-19 pandemic, the problems of resource availability, allocation and adequacy have reached manifolds. The healthcare personnel have reported different challenges involving resource availability, allocation and adequacy and highlighted the following:
There is a serious shortfall of PPE. We are forced to reuse it since they are not readily available… The gloves, masks, sanitisers and other disinfectants have suddenly become so important but scarce… (Physician) …I am a pathology lab technician. Since we do not directly come in contact with patients, I have been told to use the same PPE at least for 2 weeks, However, we do process different kinds of infective samples and in these times, I feel threatened ... (Lab technician) The problem is overnight transformation of wards to isolation units…. We have been forced to convert many of our wards into isolation rooms since the common symptoms of fever and respiratory distress, calls for isolation until the test results are received… (Hospital manager) There are no designated areas to change and wear the PPEs or their disposal is also an issue. Wearing PPEs for long hours do not let us eat or drink water or use the washroom. (Nurse) The medicine supply chain has been affected due to lockdown. The various kits and other laboratory reagents are taking more time to reach, patients are unwilling or even incapable to bear the treatment cost… But you tell me, in a private hospital, being the physician, I can make some discounts but can’t waive off the major part…. It is difficult to deal with such patients. (Physician)
In India, rising medicine prices and other healthcare costs have always been a concern (Wilson, 2009). The coronavirus pandemic has increased the scale of healthcare costs. The respondents felt intimidated due to limited supply of important safety equipment such as PPE, N-95 masks, and sanitisers, infrastructure limitations and difficulty in addressing patient concerns.
The previous pandemic containment for H1N1 influenza was possible through efficient intervention (Suri & Sen, 2011). Similar strategies such as nationwide lockdown and attempts of disease containment are attempted through social distancing, closure of all the non-essential services, mass education, prime minister’s address, mobile communications on COVID-19, detailed information on home isolation or hospital visit and field visits by healthcare workers to understand the prevalence of infection are ongoing.
Financial Issues
Managing finances has been burdensome for many healthcare personnel (Roy et al., 2020). While, they are scared of infection, unauthorised absence may incur pay cuts, departmental enquiries and job losses. Most respondents from the private sector were apprehensive of the same as highlighted below.
I work in the medicine OPD of a private hospital; the hospital has been closed until further notice after five patients and two staff were COVID-19 positive. I really don’t know if they will pay full salary or deduct something. … I am scared, have EMIs to pay and meet other expenses. (Nurse) My father needs dialysis weekly. I used to get him to this hospital where I work. However, with the sudden COVID-19 impact, being government run, we have transformed into COVID hospitals and I am scared to bring him here… I am spending a lot of money in a private facility for weekly dialysis. (Paramedical staff) Suddenly, there is no medicine vendor that is providing any discount in medicines—online or offline. Many routine patients are finding it difficult to buy medicines at such high prices…. They are turning out to us for help… I feel bad when I really can’t help anyone…. (Physician) The private practice and revenue generation is severely affected. There are government regulations for COVID-19 regarding social distancing, less patients in OPDs at one time and other regulatory compliances which are difficult to be fulfilled. Additionally, fear factor among staff has led to lack of manpower for daily operations, and many patients further requesting cheaper alternatives fearing economic loss… establishment cost is taking a toll. (Physician) There is no clarity whether medical insurance companies shall cover COVID-19 patients, this is a stress for the patients and also us when they request for waiver on bills. (Physician) The prices of all essential commodities have suddenly spiked; also I have to compromise on brands due to limited availability. (Paramedical staff)
Increased healthcare costs have been one of the major challenges in developing countries like India (Mishra & Mohanty, 2019). Many Indian households are one major source of financing healthcare costs. The depth of poverty, indebtedness and impoverishment have accounted for significantly high OOP that is ever increasing (Garg et al., 2009) as reported in Mishra & Mohanty (2019). Sudden COVID-19 onsets have created a rush for essential medicines, scarcity due to altered conventional supply chain and also hoarding of medical essentials.
In summary, it can be said that fear of pay cut, employment losses, enhanced healthcare costs, medicine supply limitations and ambiguous insurance policies have resulted in additional burden of financial issues for healthcare personnel.
Perceived Managerial Ineffectiveness
Any discussion on healthcare remodelling or delivery must include the workforce. It is essential for the administrative managers and top management to identify trained and skilled manpower, ensure equitable deployment and work on motivation and morale of healthcare workers for promoting holistic healthcare system (Kasthuri, 2018). However, in practice, there is a gap that is often perceived as managerial incompetency and ineffectiveness. Following facts were highlighted by the respondents:
With this COVID-19 pandemic, there has been terrible increase in work pressure. The OPD timings have increased and there is an increase in inpatient load, especially for the fever clinic. We have been working continuously for 12 to 14 hours…. Without proper access to food and other essential amenities. All shops are closed. (Physician) In my hospital, there is no cooperation, management is so apathetic towards our needs and there is also sudden movement of staff from one specialty to another discipline of COVID treatment without prior intimation …. (Nurse) The emergency services are only open for COVID-19 or potential COVID-19 patients, my other patients are suffering as a result. (Physician)
The current challenges are due to excessive work pressure and coordination laxities at workplaces. The respondents faced issues with altered facility layout, lack of motivation and morale, management apathy and communication limitations that hospital management need to work out. The prime minister on behalf of the common Indian has also acknowledged the selfless services by the healthcare personnel.
Inconsistent Guidelines
The healthcare guidelines have become important in the backdrop of questions on standard protocols and corresponding delivery by healthcare systems/personnel. Many issues and concerns on healthcare service quality have been raised (Velen, 1997). Changing attitude, mindset, public expectation and underlying economic, technological, demographic and social developments demand more accountability and openness.
The MOHFW, India (2020) has issued detailed guidelines for prevention and control of infection in healthcare facilities. Routine investigations, protocols and other healthcare operations have been elaborately detailed with regular training sessions to develop the technical skills of healthcare personnel. The healthcare practitioners are periodically audited as per the accepted national and international standards. In hospital settings, sometimes theoretical purview differs from practical experience.
The COVID-19 pandemic has posed threat to all existing machineries of the healthcare system. Knowledge, judgment and decision of healthcare personnel have been challenged due to limited guidelines on COVID-19 testing. There are no standardised protocols, kits or previous literature on this particular pandemic strain of COVID-19. It crippled not only the Indian healthcare but also the entire world. The rippling aftermath of COVID-19 on other sectors are in limelight. The respondents listed the following challenges:
I have been seeing patients in the fever clinic. The turnout has been huge… The RT-PCR kits that are to be used for testing are not always available, they are very expensive ones. More so, it is not always the RT-PCR kits, our existing set of technical staff is not even trained to do RT-PCR, we normally outsource these tests to another laboratory… but with this COVID-19 pandemic, we can’t do that now. (Physician) The major challenge is … the entire world is facing this crisis together … we don’t have any previous reference material for such crisis … the testing strategies, validation, kit availability … Everything is under review and thus it is taking more time than expected… We are working hard … but still…. (Physician) There is no update on how our health status shall be monitored since we are doing the sample processing everyday… What if, one of us tests positive? (Nurse)
The healthcare challenges are related to lack of literature, technical expertise, demand and supply of kits, costs and health status monitoring of healthcare personnel.
Perceived Occupational Stress
Occupational stress is one of the potential causes of concern for healthcare personnel. Conventionally, it reduces job satisfaction and leads to days off work, anxiety, depression and sleeplessness, often near misses or medical errors (Kushal et al., 2018). According to Gandham (2000), as cited by Sagar et al. (2017), certain degrees of stress are experienced in all professions; however, stress should not cross threshold limits, resulting in psychosomatic symptoms or dire consequences. The stress factors have become multidimensional with COVID-19 pandemic onset. The different occupational stresses are from varied domains but are interlinked, resulting in phobia, working conditions and communication. The fear of contracting a disease while on-duty haunts all the frontline healthcare personnel. The private practice has been stopped indefinitely by many consultant doctors for the fear of germophobia in non- COVID set-ups, essentially due to lack of testing mechanism. This is creating delays in diagnosis and identification of different infections.
Safe disposal of the different hazardous materials requires lot of research and development. The disposal of biomedical waste is a socio-legal responsibility for all associated people and ensures sustainability of the environment (Datta et al., 2018). Regulatory compliance demands proper handling of biomedical and hazardous healthcare wastes. There is an enormous generation of hazardous materials and infectious items during this COVID-19 pandemic that challenged authorities with proper disposal.
Another stressful job is positive COVID-19 declaration or COVID death to family members and relatives. A positive report of COVID-19, in the current scenario, is a bad news since the next of kin feels vulnerable, miserable and as opposed to other conventional diseases like cancer or any other terminal illness, there are bouts of sudden dissociation of this next of kin from the diseased individual. The treating doctor needs to be skilful while breaking bad news (BBN) to the bereaved family. In such a situation, any inappropriate communication might prove as a primer for dissatisfaction and conflict thereby affecting healthcare provider-acceptor relationship. The respondents highlighted the following:
Most of the government hospitals including ours have turned into COVID hospitals in the last 90 days. The OPDs that routinely dealt with other diseases and infections have virtually stopped after being declared as COVID hospitals, I am scared of self-infection… . (Physician) All of a sudden we are producing too much of waste for disposal. Proper disposal of PPEs, masks and gloves along with routine things has been a challenge. We are really finding it hard to do so, especially when there is less manpower. (Hospital manager) The anticipation and the process of telling the next of kin, regarding the disease is quite challenging… Various questions and their answers are to be given … when the patient load is high, things become even more difficult when the patient has died. (Physician)
Therefore, the various perceived occupational stress by healthcare personnel can be summarised as germophobia, waste management, diagnostic delays and breaking bad news.
Societal Challenges
Dread Disease
There is always fear and anxiety regarding any infectious disease. Various diseases such as plague, H1N1 influenza and others have been witnessed in the past, globally and locally (Suri & Sen, 2011). In such scenario, there is increased panic and doubts regarding the diagnosis. The supplementary information and electronic and print media trials create an alarm response as people feel agitated and frightened (Sivaramakrishnan, 2011). The national and international health organisations have redesigned and redefined certain agendas for the various infectious diseases so that these lessons from previous challenges could be used for understanding, mobilising and persuading people to act logically alongside disease eradication.
The recent COVID-19 scenario has given rise to sudden increase in such societal challenges for the common man. These challenges become profound for healthcare personnel, who apart from the workplace challenges need to work on challenging situations they face in community. The respondents have spoken about following challenges:
I stay in a rented accommodation. The landlord of the house has asked me to either go to any relative’s place or vacate the house since he fears that I might be a carrier of infection. No explanations are working to convince him… (Nurse)
The common man, on one side, treats healthcare personnel with a lot of respect since pursuing medicine is a noble profession; however, the fear and anxiety of infection is forcing them to alienate such people from community settings.
Social Adaptiveness
Various innovations have resulted in growing expectations from the healthcare personnel (Velen, 1997). Current population expects quality healthcare services. With the COVID-19 pandemic, there has been a serious toll on the work-life balance of the healthcare personnel severing their personal relationships. The respondents have noted the following challenges:
My elderly parents stay with me. Every day when I come out of the house, I see the panic in my mother’s face while she waves me bye. Her eyes speak that she is scared about my life and prays that I don’t contact the disease… To be honest … the feelings are mutual. Even I am scared about the same, more so since my parents stay with me… (Physician) … At the beginning, I had to stay in the hospital for a week due to sudden increase in work load. My daughter who is 4 years old, cried every night since she didn’t see me. I felt so miserable and helpless… When I came home, I was scared not to touch her before sanitising everything including the mobile. (Nurse)
In summary, it can be said that the fear of infection and altered family relationship have been a real challenge for the healthcare personnel.
Challenges Related to Essential Services
In this fast-paced world, everyone is dependent on one another. The unprecedented work load coupled with infection scare and social distancing norms have affected households, more so the healthcare personnel that report to duty. The respondents listed the following:
Previously, whenever I was tired or my cook didn’t come, I ordered food online, however… now… no matter how tired I am… for eating I have to cook since no cooks or eateries are available even house cleaning is to be done on my own… (Nurse) ‘My daughter is 3 months old and needs vaccination. I am currently in maternity leave… Though I miss my OPD, but fear to take her to the hospital for the scare of infection. (Physician)
Precisely, there are issues with essential services and treatment for other non-COVID illness (Editorial: The Lancet, 2020). The experiences of different healthcare personnel based on their workplace and societal challenges reflected the changing scenario during COVID-19, which enhanced their already existing challenges at work and home settings.
Frequency, Salience and Multidimensional Scaling
The frequency, salience and multidimensional scaling (MDS) was done for workplace challenges faced by healthcare personnel. While analysing descending frequency values and salience indices of items of freelists as described in methodology, breaks (or elbows) were identified, and this was used to discern the most salient items.
Calculation of Frequency and Salience of the Different Items Using Freelisting.
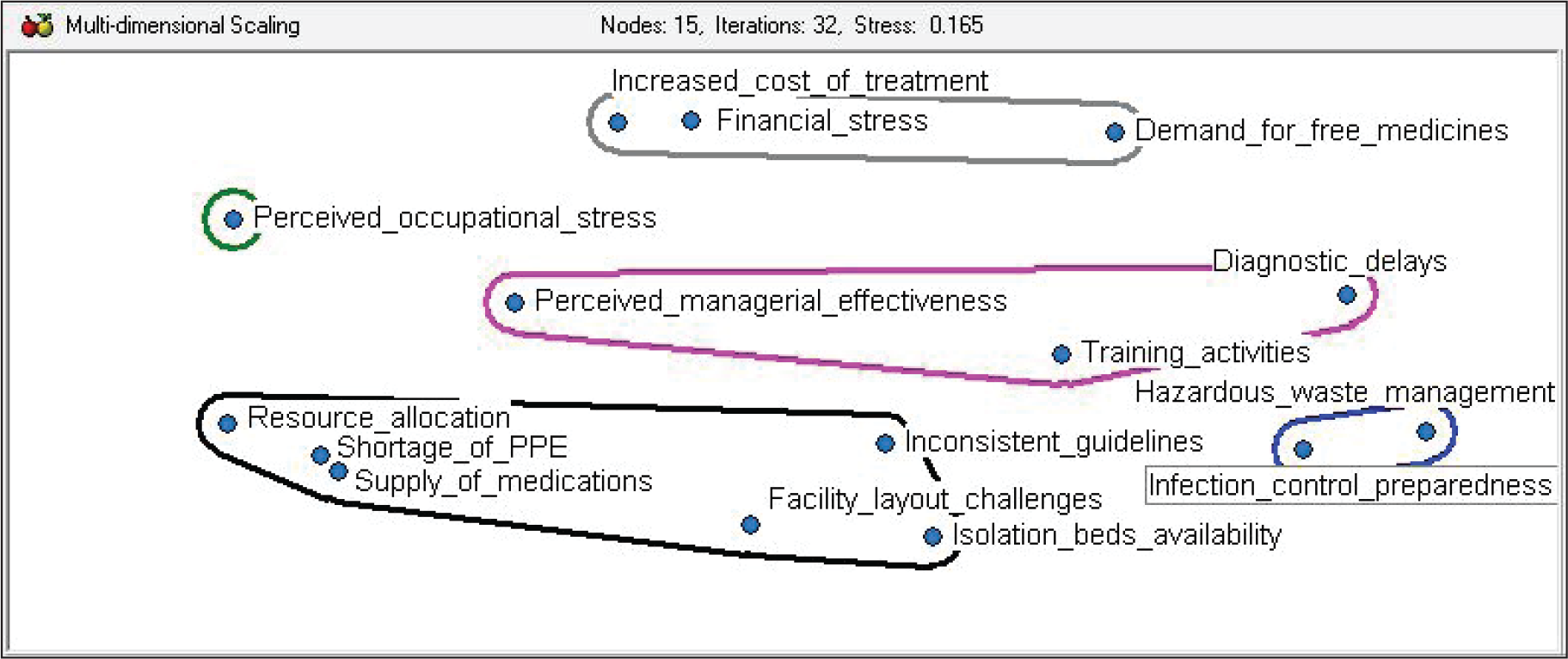
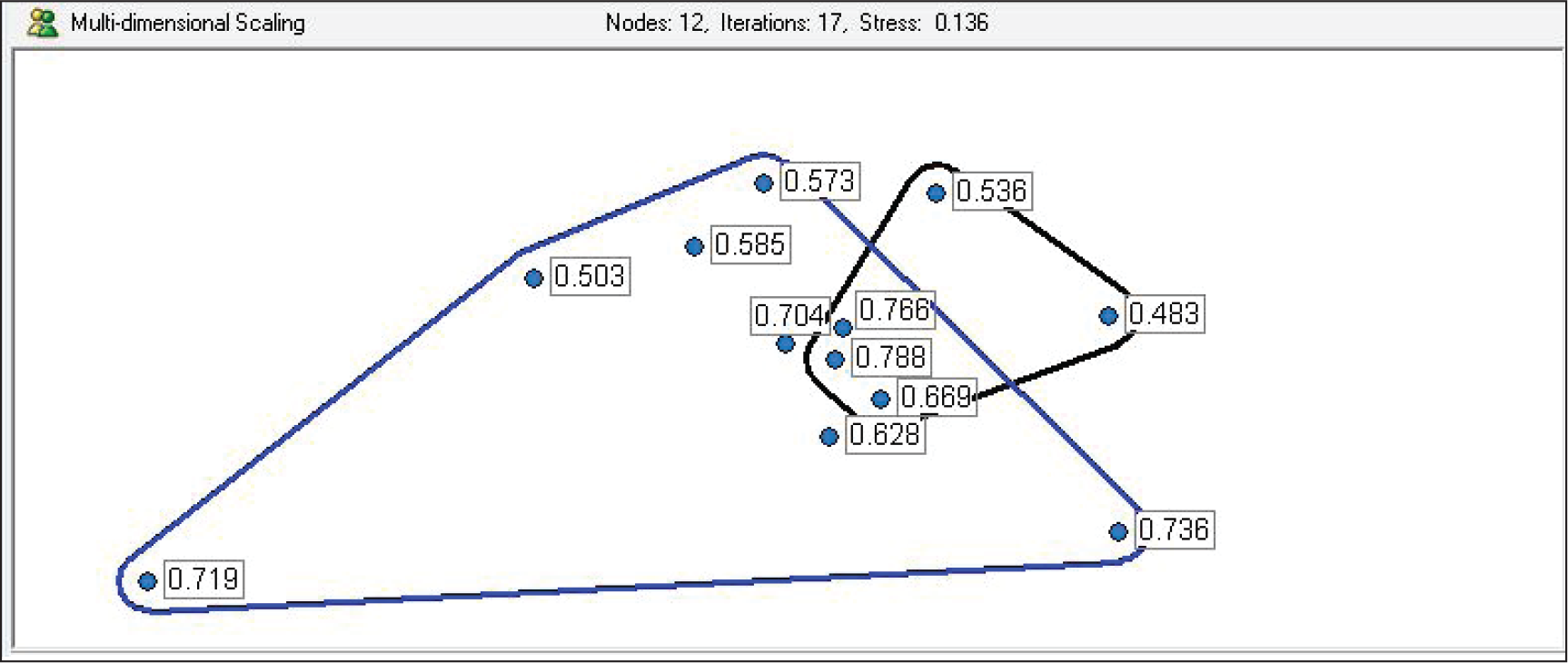
The MDS maps provided visual distance directly among the different barriers and thus communication and projections became easy. The survey research, in many cases, is troubled due to non-responses that create missing data and it further complicates the analysis. Pile sorting during the semi-structured interviews is interactive and conversational thereby reducing non response chances (Yeh et al., 2014).
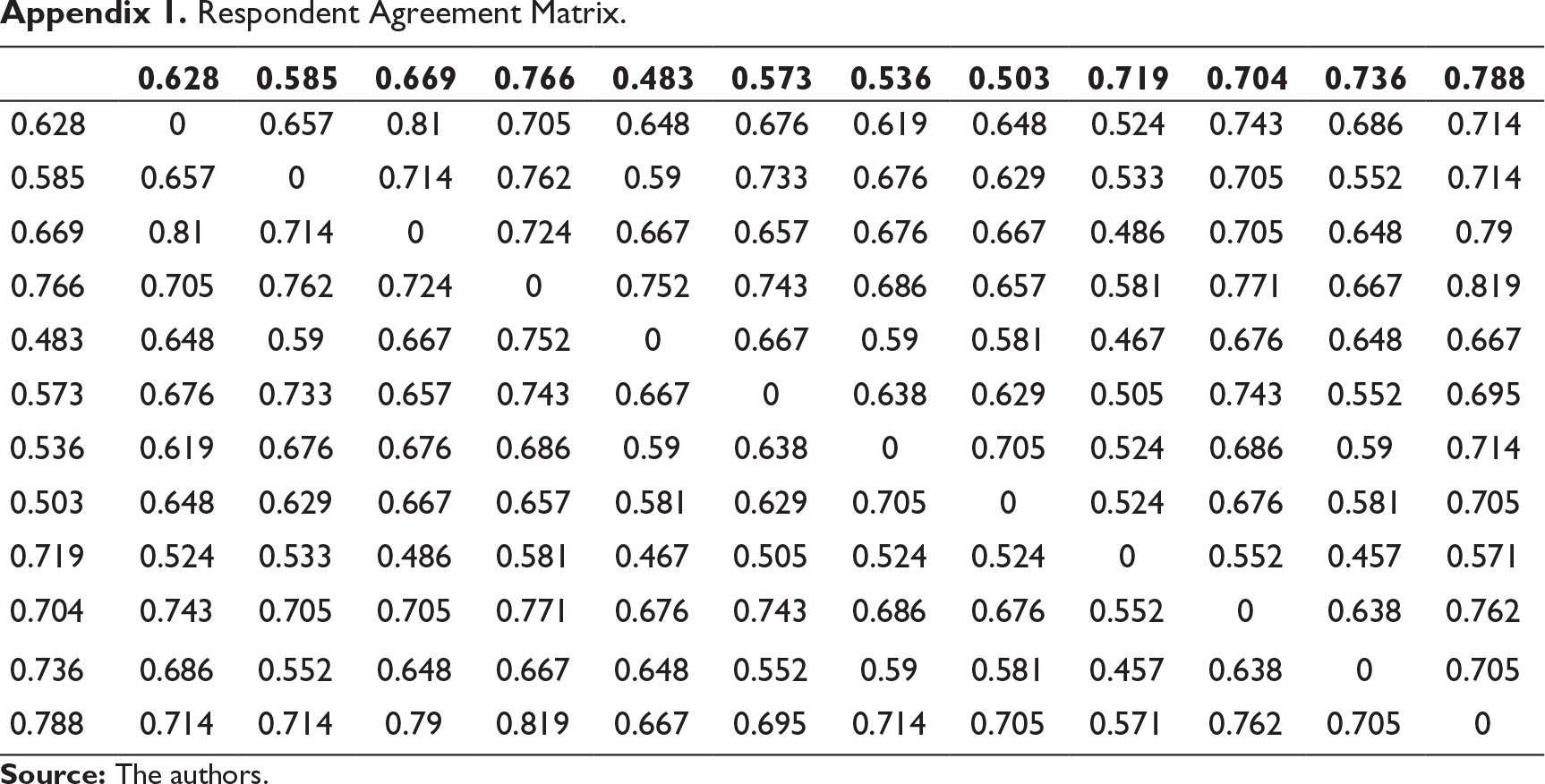
The graph for MDS, as shown in Figure 1, clusters the different workplace challenges that the respondents associated with COVID-19 into four major clusters labelled as financial support and sustainability, adaptive resilience, infection risk mitigation and healthcare facility preparedness. In Figure 2, the associations of the constructs have been visualised quantitatively. By investigating the contents of each cluster, the researchers were able to comprehend the context of the challenges. The respondent agreement matrix has been attached in Appendix 1.
Practical Implications and Suggestive Actions
Our research identified the constructs as financial support and sustainability, adaptive resilience; infection risk mitigation and healthcare facility preparedness. COVID-19 pandemic combat measures necessitate availability of diagnostic kits, protective gears and essential medications. Production of gears, generation of diagnostic kits, upscaling medicine production facilities through public–private partnership (PPP) models is needed. Industrial houses and start-ups should be encouraged and resources pipelined to meet these sudden demands. Examples to be followed are from EU countries where enhanced fostering of large-scale interactions between companies, small-scale enterprises (SMEs) various universities, research centres and public authorities to provide essential materials and drugs and alter their research and development facilities to work on the different facets of COVID-19 pandemic is noted (Rombi, 2020).
Livelihood is a fundamental need of any individual; the scarcity of this will seriously hamper his/her performance and enhance stress levels to unimaginable heights. While revenue generation has become a concern for different private hospitals, the realisation that the pay cuts/loss of employment shall stabilise their finance needs to be judged with caution and long-term sustainability. Government hospitals and their finances is a different scenario. However, consideration regarding pay cuts in both these sectors needs to be looked upon with humanitarian concerns and not just overt annual figures.
The processes of individual and collective learning must be promoted within the society to adjust to the new normal. Cooperation among different stakeholders is necessary for achieving healthcare resilience. In this regard, learning from errors and crises serves as an effective tool. Innovation, group developments, building capacities and social cohesion can only be nurtured through quality learning. It is essential to focus on using traditional ethno-botanic healthcare knowledge for positive adaptations and resilience.
Fear factors on COVID-19 are real and the effective way to mitigate is by enhancing testing rates. Public and private healthcare providers should be equal stakeholders in the long term. Treatment regimen, diagnostic protocols and waste disposal guidelines should be worked upon and followed immediately. Leading agencies of the country such as ICMR (Indian Council of Medical Research), NIV (National Institute of Virology), AIIHPH (All India Institute of Hygiene and Public Health) and other reputed institutes should be consulted for technical leads. Resource management, allocation, dynamic administrative measures and a will to go an extra mile can ensure better combative management.
Limitations and Future Scope
This study was conducted with respondents from Kolkata, West Bengal, and nearby areas. Though, utmost care has been taken to choose the hospitals and respondents that belong to both public and private sector, however, the challenges in other metropolitan and non-metropolitan cities of India might be different. Due to paucity of time, the study could not be extended to other cities. This limitation can be eradicated by recruiting numerous healthcare personnel from different Indian cities.
Another limitation of this study was that it was conducted qualitatively, although the researchers attempted to quantify the qualitative data through visual reflections. The quantitative assessment in the near future shall help to draw a composite conclusion and design suitable intervention strategies. Quantitative research can be further progressed keeping the sampling frame constant.
Conclusion
The main objective of the study was to identify the different challenges faced by healthcare personnel (physicians, clinicians, nurses, paramedics, practitioners, administrative staff, managers and leaders) in public and private healthcare facility (HCF) during pandemic COVID-19. The challenges were broadly classified into workplace and societal/community challenges. The factors underlying these challenges were considered from the extant literature and pilot survey.
The work was done using 23 items under eight constructs. These constructs categorised the challenges and issues encountered by the hea lthcare personnel into their respective workplaces and community constructs.
This study has successfully the existing concepts of healthcare research, and provided newer findings and avenues of further research on the impact of COVID-19 pandemic on lives of healthcare personnel.
To conclude, the final themes based on constructs and items devised through individual interviews, freelisting and pile sorting in agreement with respondents included the following: Financial support and sustainability, adaptive resilience, infection risk mitigation and healthcare facility preparedness.
Respondent Agreement Matrix.
Hello, may I know your name please?
May I know your age and qualification?
Could you please tell me what is your official designation?
Please tell me the name of the healthcare facility where you are currently working.
Could you please let me know your approximate income?
How long have you been working in this field?
In the current COVID-19 pandemic, what are the different workplace challenges that you have faced? Please elaborate.
Would you like to describe about the working conditions and situations at work?
Did you find any differences between conventional problems at work and those that you are facing now?
Would you like to add any more things related to problems and issues you faced while on-duty?
In the current COVID-19 pandemic, what are the different challenges that you faced in your community or society where you stay?
What are your views regarding how your neighbours and friends are interacting?
Would you like to add anything related to your societal interactions or community interactions?
Is there anything that you would like to share regarding what you are facing/have faced in this pandemic?
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.