
Abstract
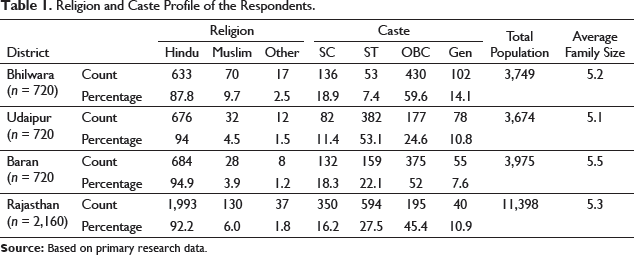
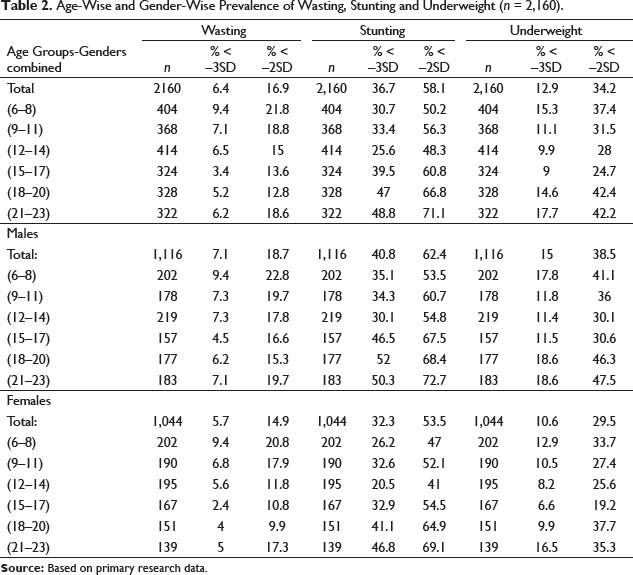
The prevalence of child undernutrition in India is among the highest in the world, nearly double that of Sub-Saharan Africa, with dire consequences for morbidity, mortality, productivity and economic growth (HNP, World Bank). India is home to most malnourished people in the world (FAO, 2015). According to data tabled in the state assembly, 37% of children below 5 years of age are underweight in the state of Rajasthan. A total of 39% of children in Rajasthan under the age of 5 years are stunted, or too short for their age, which shows that they have been undernourished for quite a while (National Family Health Survey-4—Rajasthan factsheet). Region specific magnitude of under nutrition in young children (6–23 months) at the block level is scarce. The present study carried out by IIHMR University, supported by IPE Global could be of use to the Government, policy makers as well as to the development partners working towards the enhanced nutritional status of the children. The specific objectives of the study were to collect demographic and background information about enrolled children (6–23 months) and to assess the anthropometry based nutritional status as far as wasting, stunting and underweight for the children 6–23 months and its determinants. A cross-sectional survey was undertaken. Three stage sampling method was adopted. Three districts were randomly selected from total districts of Rajasthan and from each selected district, four rural blocks/urban slums based on systematic random sampling were enrolled for the study in Stage 1. For Stage 2, for each selected block 10 villages/urban slums primary sampling unit (PSU) were selected. In the third stage, from each PSU six children in the age group of 6–11 months and 12 children from the age group of 12–23 months based on systematic random sampling were enrolled for the study. It was done from the list available to Accredited Social Health Activist (ASHA)/Anganwadi workers in the respective PSU. Thus, from every district, a sample of 720 respondents comprising two groups of infants was enrolled in the study. Hence, the total sample size for the study was 2,160 for all three selected districts. Socio-demographic and economic indicators of the respondent’s household: Information on the family composition of the household, including age, religion, caste, occupation, income was elicited through pretested semi-structured questionnaire. Anthropometric measurements were taken adopting the standard procedure for the same. WHO Anthro form 3.2.2 programming was utilised for the anthropometric examination to evaluate the magnitude of wasting, stunting and underweight in the enrolled children. A total 92% of the households in the sampled population were the followers of Hinduism. Regarding caste/tribe, around 11% of the households belonged to general category, 16% of the scheduled caste group, while the remaining 28% households were found to be from the scheduled tribe group. The overall pervasiveness of wasting, stunting and underweight was 16.9%, 58.1% and 34.2%, respectively. In case of severe wasting, stunting and underweight among children, it was 6.4%, 36.7% and 12.9% individually. It was revealed that prevalence of undernutrition was higher in males as compared to females in all the three districts. In Rajasthan, existing nutritional status of children, including wasting, stunting and underweight is a cause of concern which may get aggravated due to the current pandemic of COVID-19. Some studied shows that ‘poorer households are much more likely to report much less income during April than richer households compare to income during January and February’. To protect the vulnerable groups, especially women and children, from the effects of this nutritional crisis, there is an urgent need for high-frequency surveillance of vulnerable populations and inter sectoral convergence across segments, including health, agriculture, education, water and sanitation, social protection, commerce and livelihood.
Introduction
India is home to most malnourished people in the world (FAO of United Nation, 2015). Multiple forms of childhood malnutrition, chronic hunger, under nutrition, micronutrient malnutrition and overweight/obesity affect millions of Indian children. As per the National Family Health Survey-4 (NFHS-4, 2015–2016), nearly 36% of all Indian children below 5 years of age were underweight, and around 60% of them were having anaemia (IIPS, 2016). Given that there are nearly 139 million children aged under 5 years in India (Census of India, 2011), this translates into 50 million underweight children and 80 million anaemic children.
According to data tabled in the state assembly, 37% of children below 5 years of age are under-weight in the State of Rajasthan (NFHS-4—Rajasthan factsheet).
Thirty-nine percent of children in Rajasthan under age five years are stunted, or too short for their age, which indicates that they have been undernourished for some time, twenty-three percent are wasted, or too thin for their height, which may result from the inadequate recent food intake or a recent illness causing weight loss, and 9 percent are severely wasted, thirty-seven percent are underweight, which considers both chronic and acute undernutrition.
Rajasthan is highly affected with an under five mortality rates of 57 and the prevalence of severe acute malnutrition (SAM) at 8.6% (NFHS-4). It is well documented that child malnutrition has huge intergenerational implications for social, economic and health systems, and poses a major challenge to sustainable human development. For instance, the economic costs of malnutrition, including productivity losses and health care costs, are significantly detrimental to national economies: malnutrition costs are estimated at 2%–3% of national income and 10% of individual lifetime earnings (World Bank, 2006). This recognition is at the heart of post-2015 development agenda, and the Sustainable Development Goal 2 envisage eliminating all forms of malnourishment from the face of the sphere by 2030 (United Nations, 2016).
The Asia United Nations Network on Nutrition, comprising FAO, WFP, WHO and UNICEF, is concerned about the impacts of the COVID-19 pandemic on the nutritional status of those most affected, particularly the poor and vulnerable groups (UNICEF-2020).
The available knowledge and evidence show that although nutrition outcomes are affected by a range of biomedical and social-cultural factors, feeding and dietary practices and lifestyle factors are also important determinants of nutrition and health. Children's nutritional needs and physical endurance levels increase progressively, and adherence to standard norms can pave the way for their healthy growth.
Region specific magnitude of under nutrition in young children is scarce. The present study supported by IPE Global could be of use to the Government, policy makers as well as development partners working towards the enhanced nutritional status of the children. Therefore, the current documentation was carried out on a magnitude of under nutrition and its determinants in children (6–23 months) in the selected block of Rajasthan.
The specific objectives of the study were:
To collect demographic and background information about enrolled children (6–23 months). To assess the anthropometry based nutritional status as far as wasting, stunting and underweight for the children 6–23 months and its determinants.
Methods
Study Setting
Rajasthan, in all has 33 districts (census 2011) which were stratified into different Agro-climatic zones. Districts Udaipur and Bhilwara from Sub-Humid southern plains and district Baran from Humid South eastern plain were selected. A random sampling procedure was adopted for selection of zones and districts.
Study Design
The cross-sectional survey was undertaken. The study focuses on the magnitude of undernutrition in children in the age group of 6–23 months. Three stage sampling method was adopted. Three districts were randomly selected from total districts of Rajasthan and from each selected district, four rural blocks/urban slums based on systematic random sampling were enrolled for the study in Stage 1. For Stage 2, from each selected block, 10 villages/urban slums (PSU) were selected. In the third stage, from each PSU, six children in the age group of 6–11 months and 12 children from the age group of 12–23 months based on systematic random sampling were enrolled for the study. It was done from the list available to ASHA/Anganwadi workers in the respective PSU. Thus, from every district, a sample of 720 respondents comprising two groups of infants was enrolled in the study. Hence, the total sample size for the study was 2,160 for all three selected districts.
Sampling Procedure
To determine the sample size, the single population proportion formula was used. The sample size of the study was determined into the consideration of 95% confidence interval, 5% margin of error and 23.3% prevalence of child undernutrition in Rajasthan from NFHS-4. The estimated sample size was 716 = 720 samples/district.
Data Collection
Socio-demographic and economic indicators of the respondent’s household: Information on the family composition of the household, including age, religion, caste, occupation, income was elicited through pretested semi structured questionnaire.
Anthropometric Measurements
In this study the anthropometric data were accumulated through measuring length/height and weight of all children aged 6–23 months using standard methods. Weight was measured using a standard weighing scale with minimum clothing. Kilogram had been the unit of measurement and values were considered to the nearest value of 0.1 kg. Firstly, the weight of the mother and the child was collectively measured on the weighing scale and then for the mother alone. The value of the weight of the child was finally obtained by subtracting the mother’s weight from the cumulative weight of the mother and child combined. Length was measured with the child in a recumbent position, from head to toe and using a standard measuring tape. The unit of measurement for height was centimetres and height values were recorded to the nearest 0.1 cm.
Anthropometric Data Analysis
For anthropometric analysis, six different age categories were created. Category C1 included children belonging to the age group of 6–8 months, the Category C2 comprised children of 9–11 months, C3 comprised children aged 12–14 months, C4 contained those aged 15–17 months, C5 comprised children of 18–20 months age and C6 involved with children 21–23 months. Age regarding completed months was considered, and it was calculated considering the birth date of the child and the survey date.
WHO Anthro-version 3.2.2 software was used for the anthropometric analysis, inputs were made in the software for the parameters of survey date, cluster, ID, household, sex, date of birth and anthropometric measures—weight (in kg), height/length (in cm) and calculation of age (in months). The WHO Child Growth Standards (2006) were considered as a reference.
The anthropometric index of wasting as per the tool was defined as a low weight-for-height Z-score (WHZ), with WHZ values below –2SD of the reference population indicating wasting, while below –3SD meaning severe wasting, similarly stunting was defined as a low height-for-age Z-score (HAZ), with values below –2SD, stunting while those falling below –3SD indicating severe stunting, and equally underweight was defined as having weight-for-age Z-score (WAZ) value below –2SD as underweight and the values below or –3SD as severely underweight.
Using the Anthro tool the Z-scores of the anthropometric indices of wasting, stunting and underweight, were respectively obtained as WHZ, HAZ and WAZ. The analysis using the software was performed for the entire population of 2,160 children firstly, and then district-wise analysis of the children belonging to each of the three districts (720 sample size per district) was also performed, and results were obtained.
Results
Demographic Profile of the Respondents
Religion and Caste Profile
Religion and Caste Profile of the Respondents.
Anthropometry-Based Nutritional Status of the Children
WHO Global Database on Child Growth and Malnutrition in 1997 stated that low height-for-age or stunting is an indication of undernutrition that reflects an inability to get sufficient nourishment over a significant stretch and is similarly influenced by recurrent and chronic illness. WHO as well as the Population Council define the children as stunted if,
Anthropometric status of children and adolescents if their height for-age is in more of two standard deviations underneath (< –2SD) the WHO Child Growth Standards Median. On the other hand or low weight-for-height, wasting may result from inadequate food intake or from an ongoing sickness causing weight reduction. Underweight, or low-weight scavenge is a composite index that considers both acute and chronic undernutrition. Children are defined as underweight if their weight-for-age is more than two standard deviations (< –2SD) the WHO Child Growth Standards Median. (WHO, 2009)
Incidence of wasting, stunting and underweight in enrolled children is presented in Table 2. The results as per the WHO Anthro software were obtained in the form of age-group wise and gender-wise for the entire child population included in the study and separately for each of the three districts in the three anthropometric indices of wasting, stunting, and underweight.
Age-Wise and Gender-Wise Prevalence of Wasting, Stunting and Underweight (n = 2,160).
Wasting
District and Gender-wise Prevalence of Wasting in Children 6–23 months (n = 2,160).
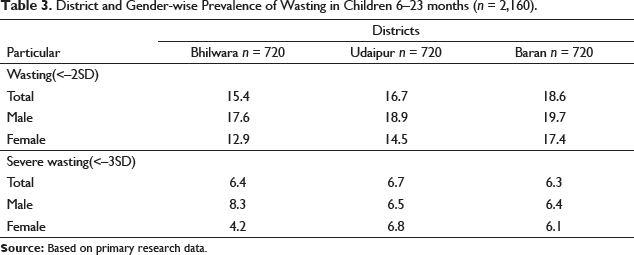
The overall prevalence of wasting in Udaipur district was 16.7%, with severe wasting at 6.7%. Amongst males, 18.9% were wasted, of which 6.5% were severely wasted. The prevalence of wasting in females was found to be 14.5%, with sever wasting at 6.8%.
The overall prevalence of wasting in Baran district was 18.6%, with severe wasting at 6.3%. Amongst males, 19.7% were wasted, of which 6.4% were severely wasted. The prevalence of wasting in females was found to be 17.4%, with sever wasting at 6.1%.
In all the three districts prevalence of wasting was higher in males compared to females. Of all the three districts, Udaipur district had the highest prevalence of wasting at 16.7%. Prevalence of severe wasting was highest in the age group of 6–8 months children.
Stunting
District and Gender-wise Prevalence of Stunting in Children 6–23 months (n = 2,160).
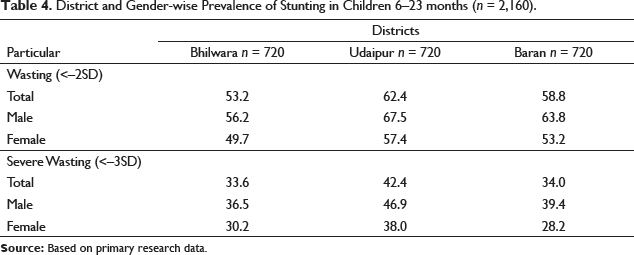
The overall prevalence of stunting in Udaipur district was 62.4%, with severe stunting at 42.4%. The prevalence of stunting amongst males was 67.5%, with severe stunting at 46.9%. Amongst females, 57.4% were stunted, of which 38.0% were severely stunted.
The overall prevalence of stunting in Baran district was 58.8%, with severe stunting at 34.0. The prevalence of stunting amongst males was 63.8% , with severe stunting at 39.4%. Amongst females, 53.2% were stunted, of which 28.2% were severely stunted.
The prevalence of stunting was higher in males compared to females in all the three districts. Similar to wasting, Udaipur had the highest prevalence of stunting at 62.4% compared to Bhilwara and Baran. Prevalence of severe stunting was highest in the age group of 21–23 months children. It was found to be higher in males than females.
Underweight
District and Gender-wise Prevalence of Underweight in Children 6–23 months (n = 2,160).
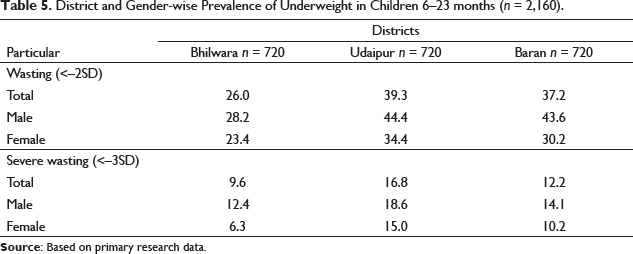
The overall prevalence of underweight in Udaipur district was 39.3% with severe underweight prevalence at 16.8%. The prevalence of underweight amongst males was 44.4%, with severe underweight prevalence being 18.6%. Amongst females, 34.4% were underweight, of which 15.0% were severely underweight.
The overall prevalence of underweight in Baran district was 37.2% with severe underweight prevalence at 12.2%. The prevalence of underweight amongst males was 43.6%, with severe underweight prevalence being 14.1%. Amongst females, 30.2% were underweight, of which 10.2% were severely underweight.
The prevalence of underweight was higher in males compared to females. The Udaipur district had the highest prevalence of underweight at 39.3% compared to Bhilwara and Baran. The study reveals that the Udaipur district had the highest incidence of wasting, stunting and underweight compared to Bhilwara and Baran. Predominance of severe malnourished was highest in the age group of 6–8 months children. It was found to be higher in males than females.
Determinants of Undernutrition
It was thought worthwhile to determine the factors responsible for the higher prevalence of undernutrition in children 6–23 months. A logistic regression analysis was carried out to assess determinants of the under nutrition. To determine the variables significantly associated with the anthropometric outcomes of wasting, stunting and underweight in the three study districts a statistical analysis using SPSS software version 21 was performed. The results of the logistic regression analysis of the three anthropometric indices are presented in Tables 6–8.
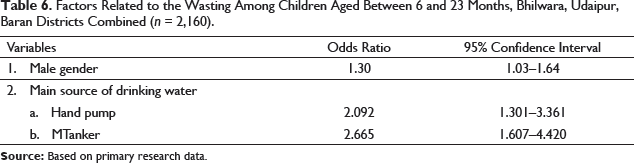
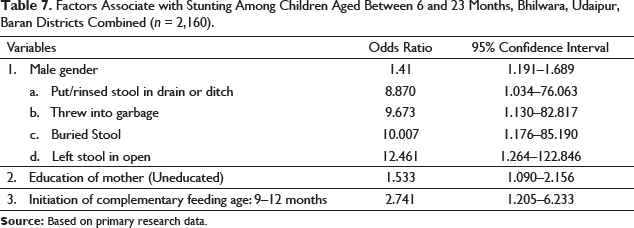
The statistical analysis revealed that gender of the child was substantially linked with wasting, stunting and underweight. The male children were significantly more wasted (OR = 1.30, CI = 1.03–1.64), stunted (OR = 1.41, CI = 1.19–1.689) and underweight (OR = 1.48, CI = 1.23–1.78), as compared to the female children.
Regarding wasting, the main source of water, at the household level, was significantly associated. For those drinking water from hand pump (OR = 2.092, CI = 1.301–3.361) and tanker (OR = 2.665, CI = 1.607–4.) were at higher risk of wasting, as compared to other sources of drinking water.
In agreement to some of the studies done in India, assessing the association of household latrine and personal hygiene practices with stunting of the child, the present study revealed a substantial association between the method of disposal of stool and stunting. For those adopting methods for a stool disposal as putting a stool in drain or ditch (OR = 8.870, CI = 1.034–76.063), throwing into the garbage (OR = 9.673, CI = 1.130–82.817), burying the stool (OR = 10.007, CI = 1.176–85.190) and leaving stool in the open (OR = 12.461, CI = 1.264–122.846) were at a significantly high risk of stunting, as compared to those adapting using toilet/latrine.
Factors Related to the Wasting Among Children Aged Between 6 and 23 Months, Bhilwara, Udaipur, Baran Districts Combined (n = 2,160).
Factors Associate with Stunting Among Children Aged Between 6 and 23 Months, Bhilwara, Udaipur, Baran Districts Combined (n = 2,160).
Factors Linked with Underweight Among Children Aged Between 6 and 23 Months, Bhilwara, Udaipur, Baran Districts Combined (n = 2,160).

Discussion
The first 1,000 days of life offer a crucial window of opportunity to preclude the immutable and lifelong destruction due to poor feeding practices. Children at the age of 6–23 months are at highest risk, for stunting, micronutrient deficiencies and common illnesses like diarrhoea and lung infections. In the present study, the nutritional status of children (6–23 months) was assessed using WHO growth standards. The overall predominance of wasting, stunting and underweight was 16.9%, 58.1% and 34,2%, respectively, whereas, severe wasting, stunting and underweight among children was found to be 6.4%, 36.7% and 12.9% respectively in the studied districts of Rajasthan. It was revealed that the pervasiveness of undernutrition was higher in male child as compared to female child in all the three districts. Similarly, a study in Surat region by Reddy et al. (2016) reports prevalence of stunting, wasting and underweight was 39%, 22.5% and 44%, respectively.
The result of Maharashtra’s comprehensive nutrition survey, which detailed about the nutritional status of the children (0–23 months), depicted that around one-fourth (22.7%) of children were stunted, with more than one-third (7.4%) of them were severely stunted. The most significant predictors of stunting and poor linear growth in children under 2 years were birth weight, child feeding, women’s nutrition and household sanitation. Simultaneously the study also revealed that ‘low feeding frequency, low consumption of eggs, less intake of dairy products, fruits and green leafy vegetables were associated with stunting and poor linear growth in children 6–23 months old’ (Aguayo et al., 2016). Comparable findings were additionally disclosed in the Rajasthan (CNSS, 2017-2018).
As per the International Food Policy Research Institute (IFPRI) resources and analyses of COVID-19 impact study, the current COVID-19 pandemic may fill in as a tempest for worldwide malnutrition. The malady condition will exacerbate the nutritional status of vulnerable groups through multiple factors. A hazardous decline in dietary quality in low-and middle-income countries is due to wage losses as well as from the sub-optimal implementation of schemes such as midday meal program and supplementary nutrients services during lockdown. Due to poor Infant and Young Child Nutrition (IYCN) practices and poor health seeking behaviour malnutrition will also increase. Resources might get shifted from nutritionally important activities as well as from antenatal care, micronutrient supplementation and the prevention and cure of childhood diarrhoea, infection control, which may lead to acute malnutrition in this COVID-19 pandemic situation.
‘The economic fallout of the COVID-19 pandemic could push up to 86 million more children in household poverty by the year ending 2020, 15%’ more children will fall under the category of malnutrition across low and middle-income countries said the study conducted jointly by the UNICEF and Save the Children. The analysis highlighted that ‘without urgent action to save families from the financial hardships caused by the pandemic children are highly vulnerable to even short periods of hunger, malnutrition, potentially affecting them for their whole life’.
Conclusion
In Rajasthan, the nourishing status of children in the age group of 6–23 months, including wasting, stunting and underweight is a reason for concern which may get aggravated because of the current pandemic of COVID-19. To secure these powerless and most vulnerable groups, especially women and children, from the impacts of this nutritional disaster, there is a pressing requirement for high-recurrence reconnaissance of vulnerable population and entomb sectoral intermingling across areas, which include sector of health, farming, water and sanitation, social protection, business and commerce. Just as in normal times, malnutrition remains a multifactorial problem and hence during times of pandemic, it required special attention with multisectoral endeavours. Government should pay special attention to easing hunger and malnutrition to deal with COVID-19 infections among children, particularly to children in the age group of 6–23 months.
Footnotes
Acknowledgement
The study was conducted by IIHMR University, Jaipur. We gratefully acknowledge the technical and financial support of IPE Global Limited to carry out the study.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.