
Abstract
Introduction
Since the first reported case of coronavirus disease 2019 (COVID-19) in December 2019, in Wuhan, China, it has quickly spread globally, prompting the World Health Organization (WHO) to declare it a pandemic on 12 March 2020 (WHO, 2020a). As of 6 May 2020, the WHO had reported 3,588,773 COVID-19 cases (including 247,503 deaths) in more than 210 countries and regions (WHO, 2020b).
India reported its first COVID-19 case on 30 January 2020, in Kasaragod town in the state of Kerala, and had reported 49,391 cases (including 1,694 deaths) by 6 May 2020 (WHO, 2020b). To contain the disease, a nationwide lockdown was declared in India on 25 March 2020, which has been extended at least until 31 May 2020. The citizens were advised to stay at home and maintain social distancing.
COVID-19 is caused by a previously unreported strain of coronavirus, officially named Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). It primarily spreads person to person through close contact and contaminated surfaces, often via small droplets produced by the infected person through coughing, sneezing or talking (CDC, 2020a; WHO, 2020c). COVID-19 is most contagious immediately after the onset of symptoms, although the spread through asymptomatic cases has been reported (Bi et al., 2020). The incubation period is around 5 days (range, 2–14 days) and common symptoms include fever, cough and shortness of breath (CDC, 2020b, 2020c; Chen et al., 2020; Elsevier, 2020). There is no known vaccine or effective antiviral treatment for COVID-19 (WHO, 2020c), but only symptomatic management and supportive therapy (CDC, 2020d). Therefore, it is important to empower people by educating them and effectively communicating accurate information about the preventive measures (e.g., handwashing, covering one’s mouth while coughing or sneezing, maintaining social distancing and self-isolation).
As researchers continue to study COVID-19 pathogenesis, new information is being generated daily. However, the pandemic-induced panic has led to rapid spread of myths and misinformation. Therefore, governments have urged citizens to confirm the authenticity of information before sharing it with others.
University students represent a special subset of the student population that has more autonomy and pressing needs to live independently but lacks life experience. Furthermore, university students are among the most active members of various social media platforms. Their perceptions and behaviours could have a massive impact on the spread of a pandemic (Peng et al., 2020). Therefore, it is important to evaluate their understanding of the COVID-19 pandemic. We conducted a cross-sectional study to access the knowledge, attitude and practices (KAP) associated with COVID-19 among a group of university students.
Materials and Methods
Study Design
This cross-sectional study enrolled student participants from the Indian Institute of Health Management Research (IIHMR) University, Jaipur, Rajasthan, India, between 31 March and 10 April 2020. After obtaining consent of each participant, a semi-structured questionnaire was administered using the Lime platform (
Sampling
Purposive sampling technique was applied to collect data from 529 students who were currently enrolled in the IIHMR University. A total of 231 students (43.7%) who had access to the Internet during the lockdown period and had agreed to participate completed the survey.
Data Collection
The questionnaire was developed using the Risk Communication and Community Engagement (RCCE) tool, which was modified according to the local setting. The RCCE tool was developed by the China International Famine Relief Commission publication, United Nations Children’s Fund (UNICEF) and WHO, to develop, implement and monitor an action plan for effective communication and community engagement. This tool aided in preparing and protecting individuals, families and their health during the early response to COVID-19 (WHO, 2020d).
The questionnaire consisted of four sections, namely demographic background (4 questions), knowledge (17 questions), attitude (5 questions) and practices (3 questions) regarding COVID-19. The questionnaire consisted of closed-ended questions requiring either one or multiple responses from the choices provided. The link to the questionnaire was emailed to the participating students. They received a system-automated email, which clearly mentioned that after starting the survey, the students could take up to an hour to record their responses to survey questions, in order to capture their real knowledge about COVID-19. After reading a brief introduction of the study and providing informed consent, participants responded to a set of questions that appeared sequentially on their screen.
Data Analysis
The data were analysed using the Statistical Package for Social Sciences (SPSS) version 22 (Chicago, Illinois, USA). Descriptive univariate analysis of the demographic characteristics was performed. Categorical variables were summarised through frequencies and percentages, while continuous variables were expressed as means and their standard deviations and 95 per cent confidence intervals. The correct knowledge level was assessed using a scoring system, where each correct response earned the participant one point; thus, the score ranged from 0 to 15 points. Students’ correct knowledge levels were defined as ‘good’ or ‘poor’ based on an arbitrary cut-off point (70%). Inferential statistics (chi-squared test and t-test) were used to measure differences in responses and average scores between different groups of participants. A p-value of less than 0.05 was considered statistically significant.
Results
Cohort Characteristics
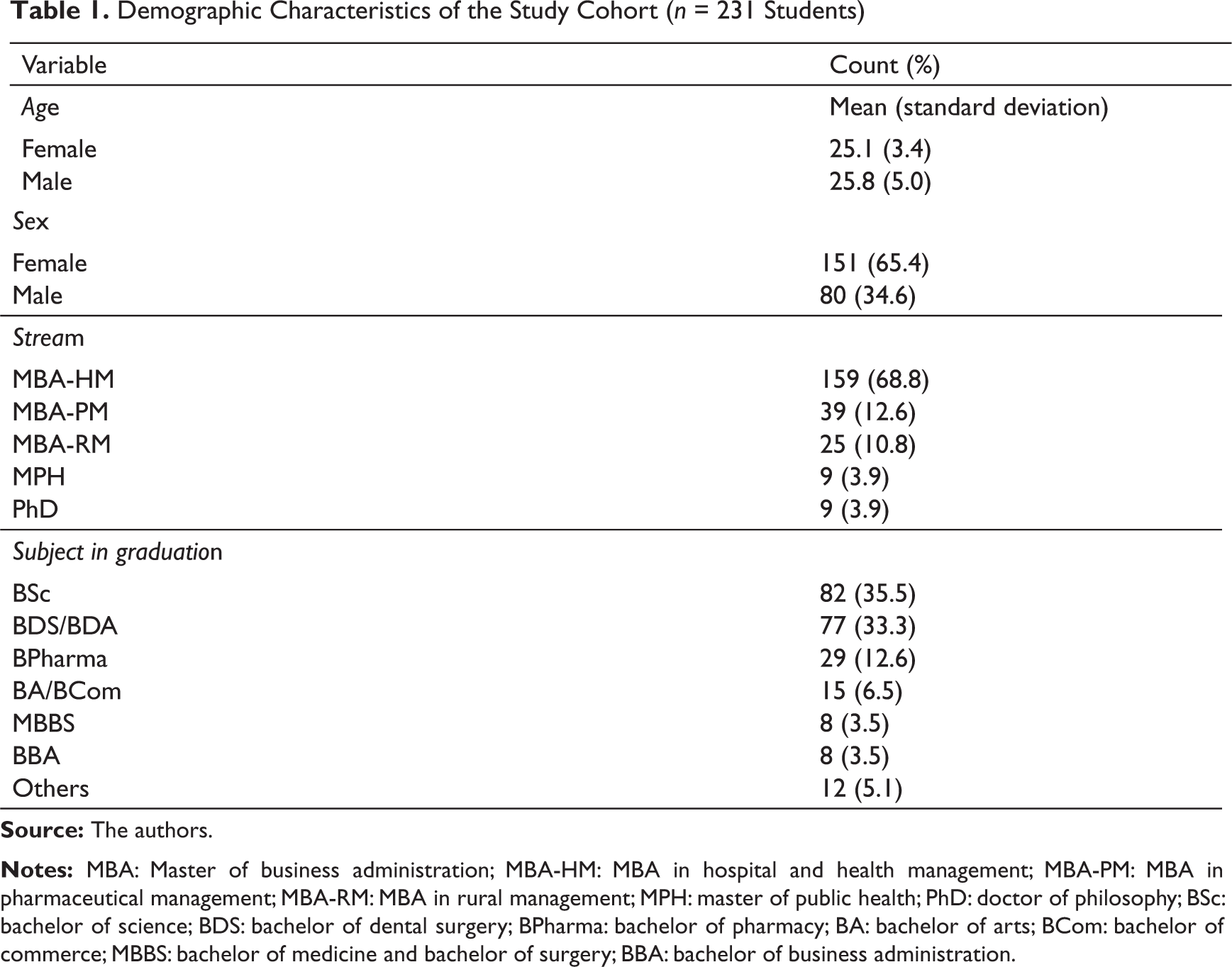
A total of 231 students participated in the study. Distribution of the students by age (mean, 25.3 ± 4.1 years; range, 20–47 years), sex, degree programme and subject undertaken at graduation is summarised in Table 1. The majority of respondents were females (65%).
Demographic Characteristics of the Study Cohort (n = 231 Students)
Awareness and Source of Information
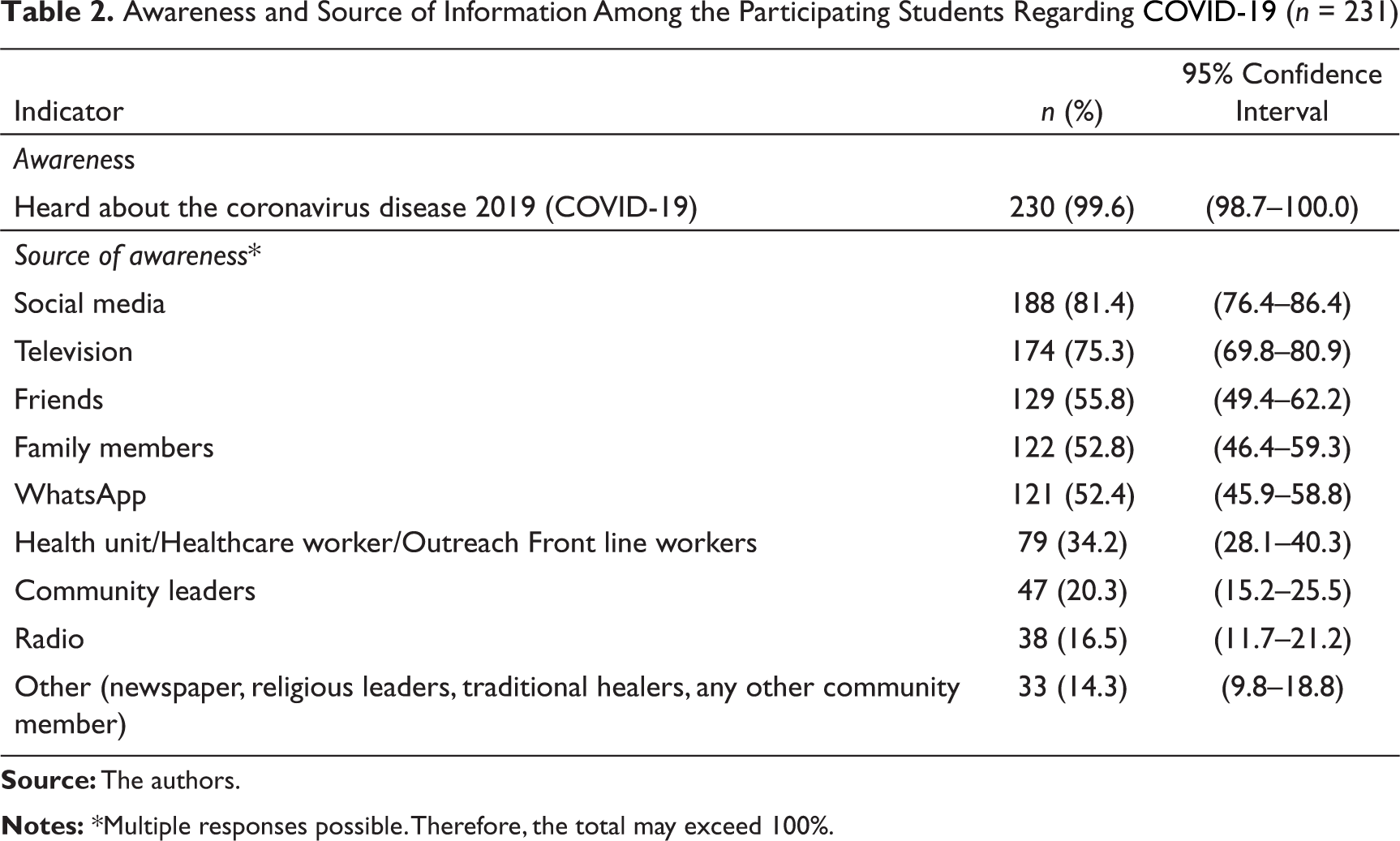
Almost all participants (99.6%) had heard about COVID-19. Social media (81.4%) and TV (75.3%) were the main sources of receiving COVID-19-related information. Over 50 per cent of the respondents mentioned friends, family members and WhatsApp as the source of information of COVID-19. Health units/healthcare workers/outreach frontline workers were reported as the source by over one-third of students. Other sources mentioned were community leaders (20%) and radio (17%) (Table 2).
Awareness and Source of Information Among the Participating Students Regarding COVID-19 (n = 231)
Knowledge
The average knowledge-level score was 9.97 ((±2.27; range, 0–15), suggesting an overall average level (66% or [9.97/15] × 100) of COVID-19 knowledge (Table 3). According to the arbitrary cut-off point, 60 per cent had poor and 40 per cent had good knowledge levels. More than a fifth of students acquired 10 points; however, only 15 students got a full score.
Correct Knowledge and Mean Score of Students Regarding Indicators Related to Protective Means, Treatment and General Awareness about COVID-19 (n = 231)

Various knowledge indicators were broadly categorised into three domains, namely protective measures, treatment and general awareness about COVID-19. The mean score (4.33 ± 1.178) for the protective measures domain was the highest, followed by the treatment (3.93 ± 1.304) and general awareness domains (1.71 ± 0.631). No significant difference was identified for any domain (protective means: χ2 = 0.667, p = 0.414; treatment χ2 = 0.305, p = 0.581; and general awareness χ2 = 1.252, p = 0.263). No significant sex differences were identified (protective means: t = −0.184, p = 0.854; treatment: t = 0.332, p = 0.740; and general awareness: t = −0.916, p = 0.360).
Ninety-one per cent of students knew that fever, cough, shortness of breath and breathing difficulties are the main symptoms of COVID-19. Two-thirds (68%) of the students knew that droplets from infected people, direct contact with infected people and touching contaminated objects or surfaces are modes of person-to-person transmission. A vast majority (94%) of students knew that regular handwashing using soap and water, the use of alcohol-based hand sanitizers, covering mouth and nose while coughing or sneezing and avoiding close contact with anyone who has a fever or cough prevent disease transmission.
Most students (92%) were aware that no COVID-19 vaccine is available. Only about half the students knew about the diagnostic test and symptomatic treatment available. Eighty-eight per cent of the students knew that COVID-19 is highly contagious. Almost all (96%) students knew that COVID-19 was first reported in Wuhan city of China in December 2019. More than 90 per cent (92%) students selected 2–14 days as the incubation period of COVID-19.
The results indicated misconceptions among students regarding the COVID-19 symptoms, transmission, prevention and treatment. Twenty per cent reported that one of the modes of getting infected was eating contaminated food, and 16 per cent marked airborne transmission. Twenty-two per cent of students felt that COVID-19 could be prevented by consuming cooked meat and eggs, followed by drinking treated water (11%). About a third of the students felt that antibiotics are effective in treating or preventing COVID-19.
Attitude and Practices
Risk perception, prevention intentions and self-reported prevention practices were analysed (Table 4). Slightly more than one-fourth of the students believed that they were at risk of getting infected with SARS-CoV-2. Almost all students agreed that they considered it very important to take action for preventing the spread of COVID-19 in their communities and felt that social distancing was an important step to prevent the spread of COVID-19. Considering the situation in India, the lockdown was considered a good strategy. Forty-two per cent of the students suggested alternative steps to prevent the spread of COVID-19 in the community. Suggestions included creating awareness about social distancing and hygiene practices; door-to-door screening; performing more tests; making wearing a mask compulsory; sealing the hotspots; extending the lockdown period; and ensuring the availability of personal protective equipment, masks and gloves for health workers.
Nearly all students reported regular handwashing and sanitisation, covering mouth and nose while coughing or sneezing, avoiding close contact with anyone who had fever or cough and following the stay-at-home advisory. Thirty per cent of the students reported that they were avoiding unprotected direct contact with live animals and surfaces that come in contact with animals. Around one-fifth of the students reported that they were consuming well-cooked meat and eggs. Most students (87%) reported that they would go to a health facility if a family member experiences disease symptoms.
Attitude and Practices of Students Regarding COVID-19 (n = 231)

Discussion and Conclusions
For a highly contagious disease like COVID-19, protecting self and others depends on complying with the recommended protocols. The KAP are important determinants of desired protective behaviours and may ultimately influence the clinical outcomes at individual and community levels. This study focused on evaluating the extent of KAP about the COVID-19 pandemic. The data were collected a week after the formal nationwide lockdown was implemented in India; therefore, almost universal or a high level of awareness was expected.
The Digital India initiative by the Government of India resulted in the country’s digitally connected population amounting to approximately 688 million active users as of January 2020 (Diwanji, 2020a). Around 35 per cent of the Indian Internet user base was between 20 to 29 years of age, the highest among all age groups (Diwanji, 2020b). Students are likely to be carriers of infection due to their lifestyle and close proximity with fellow students. Additionally, many students are information givers to their respective family members, and thus play an important role in information dissemination. Therefore, this survey aimed to provide appropriate recommendations to policymakers to facilitate effective communication of correct information to other segments of the population.
Receiving a very high percentage of correct responses in our study is very encouraging. However, information on the modes of transmission and the contagious nature of the disease was relatively low at 68 per cent and 88 per cent, respectively. The score was even lower (59%) about the knowledge of the survival of SARS-CoV-2 on different surfaces. The other indicator of concern was that only 33 per cent of the respondents knew about the vulnerable population for COVID-19. These three indicators are important in the prevention of the disease. The elderly, people with co-morbidities and healthcare workers were reported to be at the highest risk of contracting the disease and needed special care. The above results support the curative approach, whereby the treatment would probably be sought early in case of symptoms due to high knowledge; however, the preventive approach needs further strengthening. Prevention definitely assumes the highest place for personal protection, and the knowledge in this aspect was high. However, a poor understanding of whom to protect from infection and modes of transmission and survivability of the virus weaken the protective approach. The results of other KAP studies done on COVID 19 are comparable (Zhong et al., 2020); however, the difference in knowledge by sex could not be substantiated. Additionally, low perception of disease risk reduces pandemic-induced panic; however, inadequate knowledge of disease transmission, non-compliance to the stay-at-home guidelines and complacency due to lower risk perception could put these individuals and others at risk. This low perception of risk was found high among those with low knowledge of transmission, suggesting that correct and adequate knowledge is the key to keep oneself and others safe. Non-pharmaceutical public health measures are being promoted for mitigating the risk and impact of epidemic and pandemic influenza (WHO, 2019).
A deeper analysis of correct knowledge, including filtering out incorrect responses, resulted in a drastic reduction in the proportion of correct responses for those reporting symptoms, modes of transmission and preventive measures. This reduced to an even lower level of 7 per cent among those who were knowledgeable about the contagious nature of the disease, its survivability on different surfaces and high vulnerability. This was alarming and indicated the need for more awareness among the youth.
This study was conducted during the early period of the spread of disease (Stage 1) to know about the KAP of university students. As expected, social media was the primary source of information for most students. It is noteworthy that healthcare workers, who could be the source of correct and reliable information, were reported as the source by only one-third of the responders. This study underscores the importance of social media as an important source of receiving and disseminating information. Therefore, the health system could improve its social media platform and visibility to effectively disseminate information to the masses.
In conclusion, our results show the degree of adherence to personal protective measures and provide evidence to healthcare authorities and university administrations to improve communication with the students. This study provides a valuable and early insight into the areas that need attention and issues that need to be prioritised and improved for correctly sharing information and preventing the spread of misinformation about an outbreak, which dilutes the effectiveness of health policies. Community engagement activities, including communication initiatives, need to incorporate these modifications in their awareness generation activities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.