
Abstract
Background: Mathematical modelling of epidemics and pandemics serves as an input to policymakers and health planners for preparedness and planning for the containment of infectious diseases and their progression in the population. The susceptible–exposed–infectious/asymptomatic–recovered social distancing (SEIAR-SD) model, an extended application of the original Kermack–McKendrick and Fred Brauer models, was developed to predict the incidence of the COVID-19 pandemic and its progression and duration in the state of Rajasthan, India.
Objective: The study aimed at developing a mathematical model, the SEIAR-SD model, of the COVID-19 pandemic in the state of Rajasthan, for predicting the number of cases, progression of the pandemic and its duration.
Materials and methods: The SEIAR-SD model was applied for different values of population proportion, symptomatic and asymptomatic cases and social distancing parameters to evaluate the effect of variations in the number of infected persons, size of the pandemic and its duration, with value of other parameters fixed in the model. Actual reported cases were plotted and juxtaposed on the prediction models for comparison.
Results: Social distancing was the crucial determinant of the magnitude of COVID-19 cases, the progression of the pandemic and its duration. In the absence of any proven treatment or vaccine, effective social distancing would reduce the number of infections and shorten the peak and duration of the pandemic. Loosening social distancing will increase the number of cases and lead to a heightened peak and prolonged duration of the pandemic.
Conclusions: In the absence of an effective treatment or a vaccine against COVID-19, social distancing (lockdown) and public health interventions—case detection with testing and isolation, contact tracing and quarantining—will be crucial for the prevention of the spread of the pandemic and for saving lives.
Introduction
The World Health Organization (WHO) declared the COVID-19 infection a public health emergency and, subsequently, a pandemic affecting almost the whole world. The disease is caused by Severely Acute Respiratory Syndrome (SARS) coronavirus-2, which is more contagious and virulent than the SARS coronavirus. At the time of writing, over 4 million persons have been confirmed to be affected by the COVID-19 infection globally, and over 276,000 (6.88%) people have died. About 35 per cent cases have recovered from the disease. The pandemic posed a serious threat to the health of the people worldwide and emerged as a serious concern of the global health community and governments, especially since there is no available effective treatment or vaccine against the disease. In India, the first case of the SARS coronavirus-2 was reported on 30 January 2020. The state of Rajasthan, which is the largest state in India, reported its first case on 2 March 2020 in Jaipur. The national and state governments made a serious effort to contain the spread of the disease and the resultant morbidity and mortality in the population.
Many researchers have attempted to predict the number of infectious cases of the COVID-19 outbreak (Fang et al., n.d.; Nesteruk, 2020; Song et al., 2020; Zhang et al., 2020). The present study has attempted to develop a mathematical model based on the reported cases in the state of Rajasthan since the start of the outbreak to predict the number of cases and the progression of the pandemic in the state of Rajasthan, using the susceptible–exposed–infectious/asymptomatic–recovered social distancing (SEIAR-SD) predictive model.
Methods
An extended version of the susceptible–infectious–recovered (SIR) model of Kermack and McKendrick (1991) was applied for developing a prediction model for the COVID-19 pandemic in Rajasthan for estimation of the number of COVID-19 cases (Tomie, 2020). It assumes that as an infectious disease is introduced in a population, its progression will be determined by the availability of the susceptible population (S), transfer rate of infection from an infected person (I) and those recovered or killed by the disease (R). Brauer (2006) further improved the SIR model by introducing exposure to infection and asymptomatic cases, the susceptible–exposed–infectious/asymptomatic–recovered (SEIAR) model. The population is further characterised into: exposed but do not acquire the infection (E) and asymptomatic (A)—those who acquire the infection without symptoms but are infectious. Exposed and asymptomatic would move to the R stage in the model.
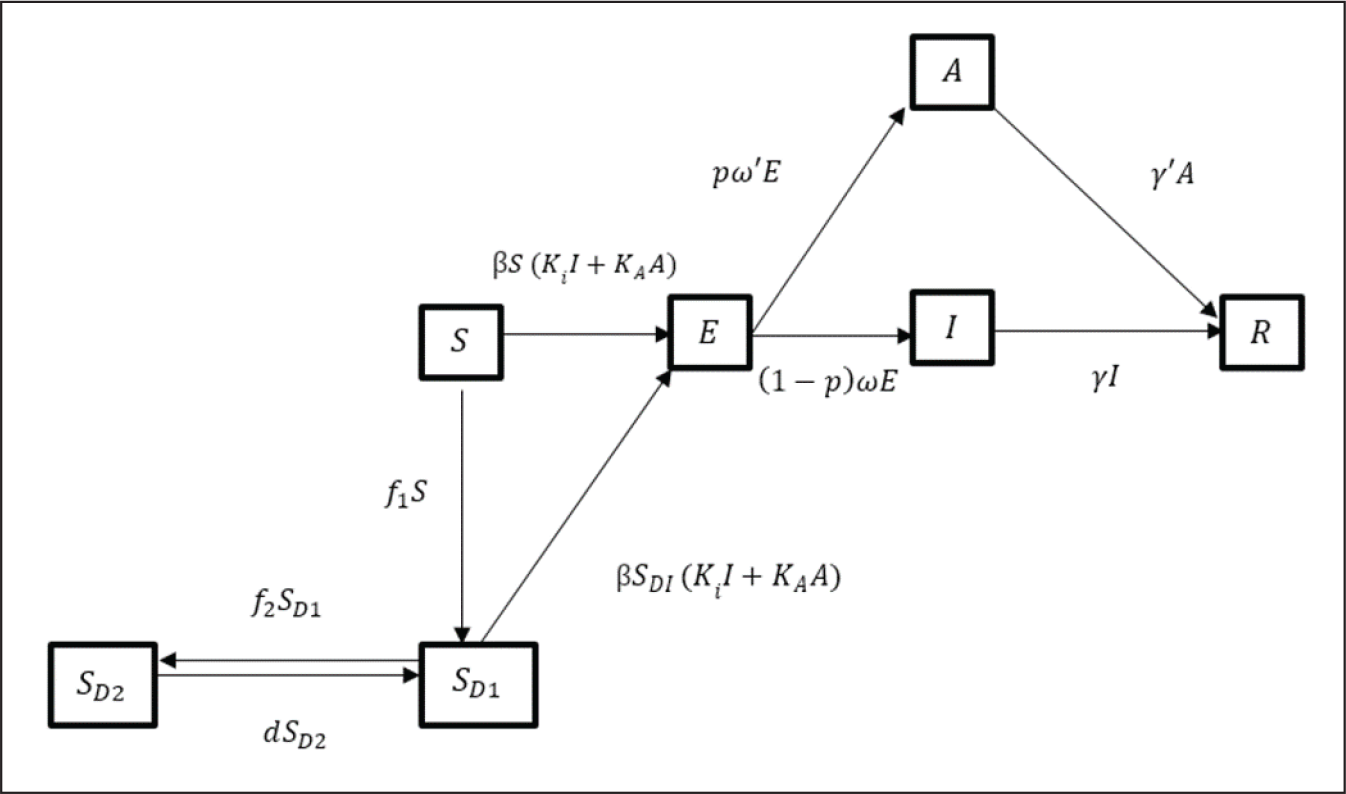
The SEIAR-SD model (Figure 1) is an extension of the SEIAR model that includes one variable, social distancing. The susceptible individuals are further categorised into two groups, one that strictly practised social distancing and did not come in contact with infected persons (SD2) and the other with no or loose social distancing norms, with the risk of exposure to the infection (SD1). The model assumed that once an infected individual is introduced into a virgin population where it is implied that all are susceptible, each infected person would transmit the infection at a rate β to susceptible individuals who come in contact. The basic reproduction number (R0) determines the progression and rate of new infections (Tomie, 2020). If R0 > 1, then the infection assumes an epidemic form. The epidemic dies out when R0 < 1. Figure 1 outlines the transmission and progression of disease.
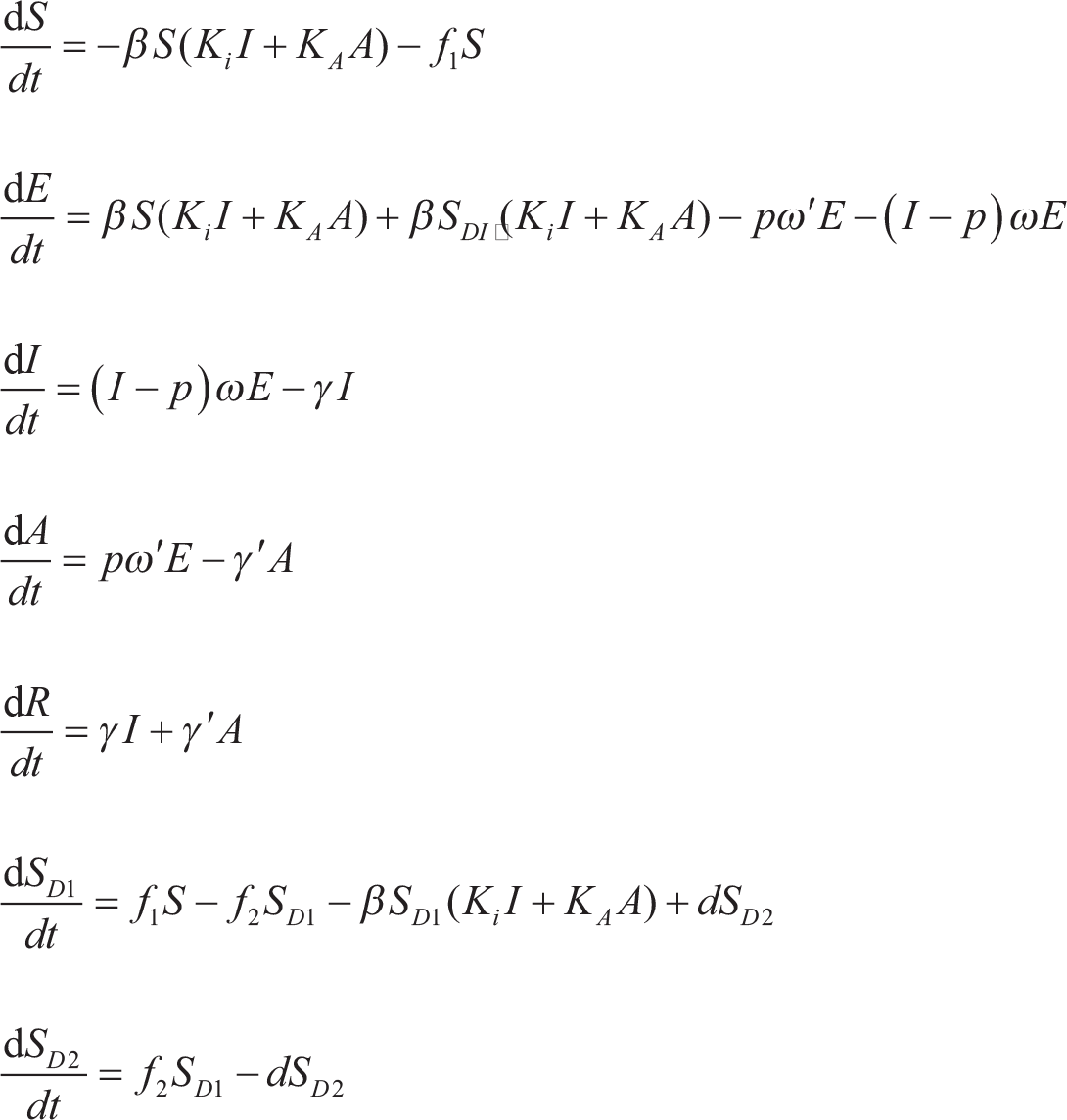
The SEIAR-SD model is expressed in the following differential equations:
where
S = susceptible population;
E = exposed to risk of infection;
I = infected individuals (symptomatic cases assumed to be infectious);
A = asymptomatic cases assumed to be infectious;
R = removed from the susceptible population (recovered/dead);
SD = social distancing; and
dS/dt, dE/dt, dI/dt, dA/dt and dR/dt, respectively, represent changing rates in population at time t, in S, E, I, A and R. β is the transmission rate of infection from an infected person to susceptible individuals coming in contact. ω and γ represent transfer rate from E to I and that from I to R, respectively, and ω′ and γ′ refer to transmission rates from exposed to asymptomatic and from asymptomatic to R. p is the proportion of asymptomatic infections, and KA and Ki represent relative risk of infection among asymptomatic and symptomatic individuals, respectively. d refers to transfer rate from social distancing to no social distancing (SD2 to SD1), and f1 and f2 are transfer rates from S to SD1 and SD1 to SD2, respectively.
Results
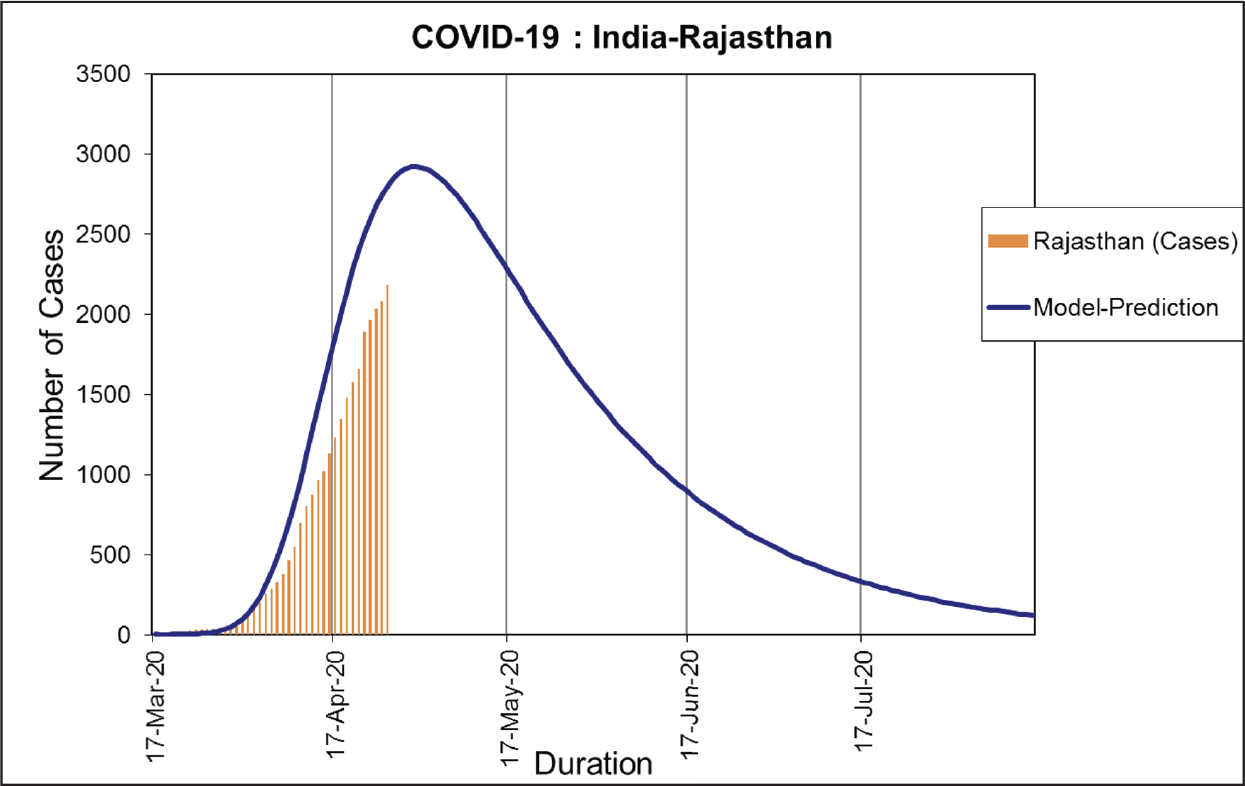
Incidence and Time Distribution of COVID-19 in Rajasthan
A total of 2,800+ cases of COVID-19 laboratory-confirmed by reverse transcription polymerase chain reaction (RT-PCR) were detected in Rajasthan up to 20 April 2020. The state of Rajasthan came under national lockdown from the mid-night of 24 March 2020. On that day, only 45 RT-PCR-confirmed cases were reported.
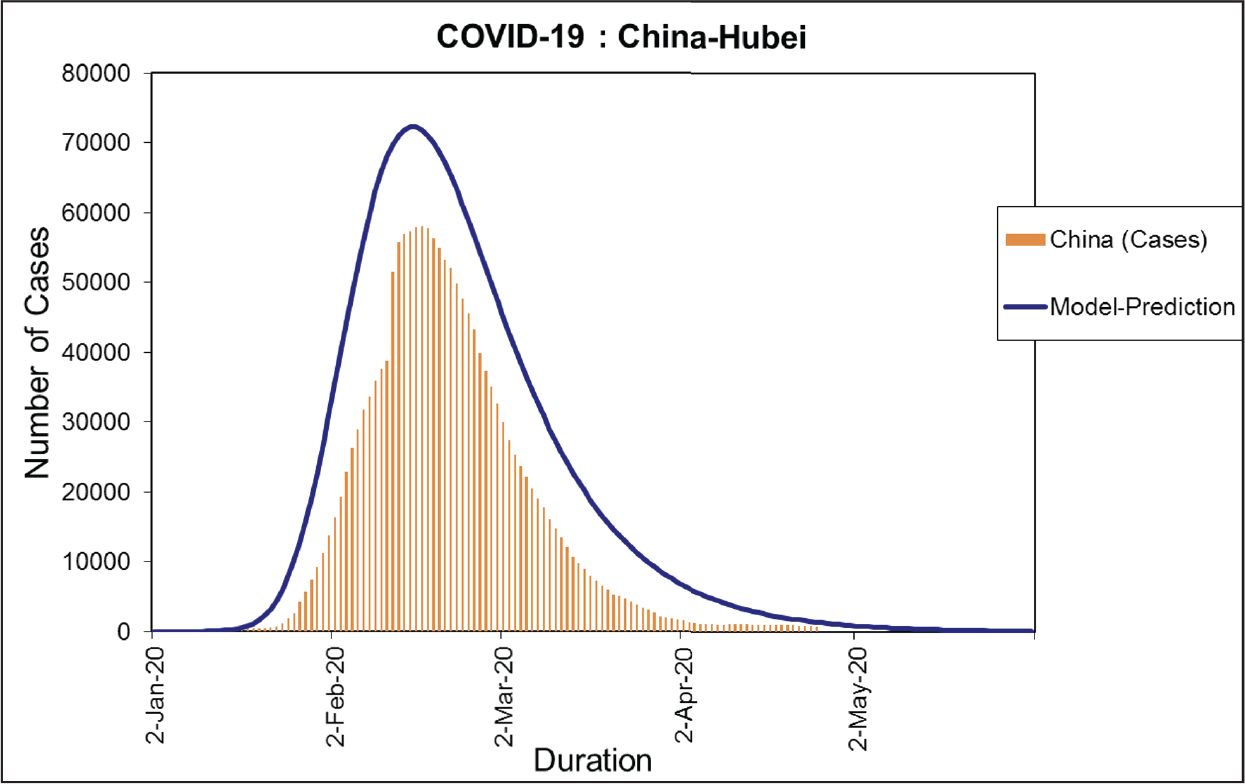
To validate our prediction model, we also modelled the actual data from the COVID-19 spread in China and found a good synchronicity between the predicted pandemic curve and the actual reported data (Figure 3) (Germany, 2020).
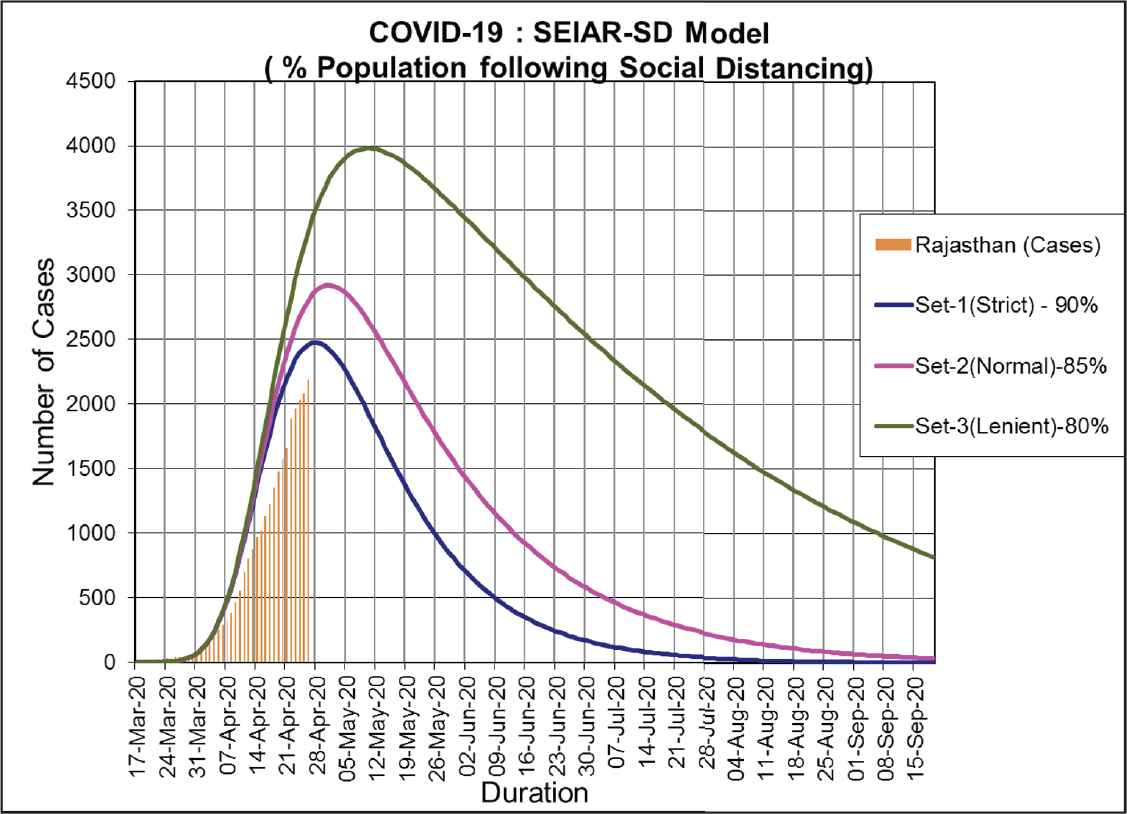
If social distancing is strictly followed, that is, 90 per cent, the expected number of infections would be 21,492 (symptomatic 6,448; asymptomatic 15,044). If lenient social distancing is practised (80%), the number of estimated total cases would rise to 61,000 (symptomatic 18,531; asymptomatic 43,240). The number of estimated cases would rise geometrically if the social distancing norms are loosened and person-to-person contact increases.
The peak would remain identical in varying social distancing norms, but the duration of the pandemic will be prolonged with relaxing social distancing norms.
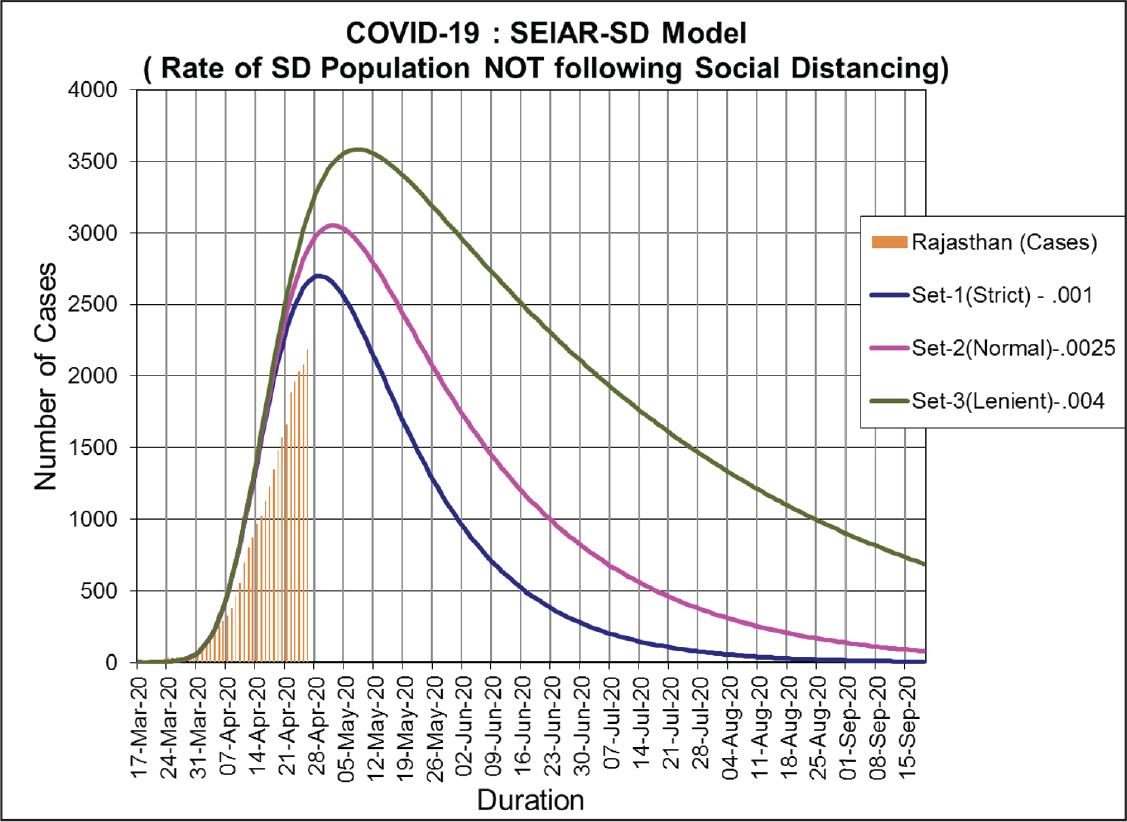
In the case of extreme mixing of the population, d = 0.004, the number of cases, both symptomatic and asymptomatic, would rise astronomically to beyond 127,000, the peak of the pandemic curve would be heightened, and the duration of the pandemic would be prolonged. But if, as in a good case scenario, the population is mixing at d = 0.001, the total number of cases will continue to be low, at about 34,000, with one-third symptomatic cases, the peak will be shortened, and the duration of the pandemic will be reduced.
Discussion
Various mathematical models are in circulation to predict the number of COVID-19-infected persons in India, a country with 1.34 billion people, during the current pandemic. COVID 19 infection reproduction rate (R0) may influence size and progression of the pandemic in the world. Mathematical models could be used as tools of studying the dynamics of disease transmission and behaviour of pandemics of acute infections like the COVID-19 and the success of social and public health interventions (Oliveira, 2020). We used an extension of the SIR model developed by Kermack and McKendrick. We factored in social distancing and asymptomatic cases in the model equation. The model can be used as a tool to study the effect of social distancing on the spread of the disease and public health interventions to control the pandemic.
However, the SEIAR-SD model has inherent limitations. It assumes that the mixing of the population is random and that the population size is unchanged. It also does not account for migration. The lockdown following the outbreak of the pandemic led to a massive exodus of millions of labourers for their hometowns across the states in India. The present model could not adjust for this unprecedented phenomenon that continues till date, and no data is available on this mass displacement of population. We could not evaluate the effect seasonality. The pandemic started in winter and is continuing through the summer with the same vengeance. The model predicts that the pandemic might tail off during the rainy season, but it is anybody’s guess. Changing strains of the coronavirus have been reported, but the model does not account for changing antigenicity and virulence. We have assumed social distancing to the extent of 80 per cent during the lockdown, but it can never be measured in real terms. Hence, keeping in view these limiting factors, modifications in the model are required to arrive at more refined estimates.
The feasibility of reining in the pandemic would critically depend on the changing value of R0. Greater the value of R0 > 1, greater would be the spread of the infection (Hébert-Dufresne et al., 2020). Our model suggests that strict social distancing measures, such as a lockdown, would significantly decrease the number of COVID-19 infections. We have validated our model on data from China, available in the public domain, and found a good fit, which gives an assurance that our assumptions and model are truly reflective of the magnitude of the coronavirus infection and its spread among the population of Rajasthan. We restricted our modelling to the population of Rajasthan, as India is a geographically and socially diverse country and any single model for the entire population of the country may not represent the true behaviour of the pandemic.
Behavioural interventions, such as social distancing, confinement in homes and the continuous use of personal protective measures, may prove to be effective at controlling the spread of the infection (Tyson et al., 2020).
Efforts are on to develop a vaccine effective against the new coronavirus strain. However, it will not be available in the market for the next 10–12 months. Until then, social and behavioural interventions, and classical public health measures of isolation, prevention and control of infectious diseases, are the only weapons against COVID-19.
Mathematical models should be used with a word of caution for an interpretation of the disease estimates. These predictions are based on mathematical modelling and certain assumptions regarding disease transmission rates, effectiveness of social distancing/lockdown and public health measures of epidemic control and prevention, such as early detection, isolation and treatment of affected persons and containment measures. Human behaviour, human biological response and characteristics of the causative organisms may not be captured completely by mathematical numbers and equations.
Mathematical modelling is a continuous and an evolving process. It will require in-depth analysis to evaluate the effectiveness of various social distancing methods, the effect of a partial lockdown, geographic distribution and socio-economic determinants on the future mathematical modelling of outbreaks and epidemics.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.