
Abstract
COVID-19 forced many nations, including the largest country in the Arabian Gulf region, Saudi Arabia, to fast-track the adoption of new technologies and work practices to cope with the pandemic. We find the Saudi Ministry of Health (SMoH), in less than a year, introduced several innovations to transform healthcare planning, management and delivery. We reflect on these changes in the Saudi Arabian context and suggest what needs to be done next to retain the developmental momentum generated in the innovation system beyond the pandemic for sustainable and positive impact on the healthcare system. To do so, the Ministry should regularly assess the appetite for change, prioritise problems and areas of intervention, collect evidence of need and impact, build confidence by educating the public and healthcare professionals about the importance of adapting to new ways and methods of healthcare delivery, collaborate with the private sector to efficiently sustain these advancements and gain the public’s trust through stakeholder participation.
Introduction
Healthcare systems around the world are generally slow to adopt innovations (Berwick, 2003). This can be due to many factors, including privacy concerns and the ways in which patients and clinicians interact with technology. Public health, particularly, has been slow to adopt digital innovations but this pattern of rejecting new technology can be nullified during a public health crisis, as evidenced by the proliferation of digital technologies during COVID-19 (Budd et al., 2020). In many Middle Eastern countries, including the Kingdom of Saudi Arabia, the COVID-19 pandemic accelerated the process of change. The Saudi Ministry of Health (SMoH) used digital innovations to communicate with the public, to deliver information and announcements, to mitigate the disease by implementing contact tracing and to manage service provision through tele-medicine and healthcare prioritisation. Although this was done to cope with the immediate health crisis, several changes might be retained to develop the innovation system further and make the healthcare system more sustainable for the long-term. Based on the aim of this special issue to identify the guiding principles of government innovation and development policy to overcome pressing challenges (Wu & Sheikh, 2021), this paper sets out to explore Saudi Arabia’s response to the COVID-19 pandemic and how the country can continually improve its national innovation policy. This will help it to better solve its most pressing problem: how to diversify its economy for a sustainable, equitable future.
The Arabian Gulf region is resource-rich with extensive healthcare infrastructure. However, the growing population, which has more than doubled in the last 30 years in Saudi Arabia, low oil prices and the increasing rate of non-communicable diseases have together put developmental pressure on resources and the infrastructure capacity throughout the region. The national strategic framework ‘Saudi Vision 2030’ has been designed to diversify and grow the economy and develop public service sectors, such as health. It coincides with the United Nation’s global 2030 Agenda for Sustainable Development Goals. Although the pandemic had a negative effect on several sectors of the economy―particularly religious tourism―we posit that the pandemic also accelerated local innovation activity in the country to make it more capable of achieving some of the goals in Saudi Vision 2030 with respect to healthcare transformation.
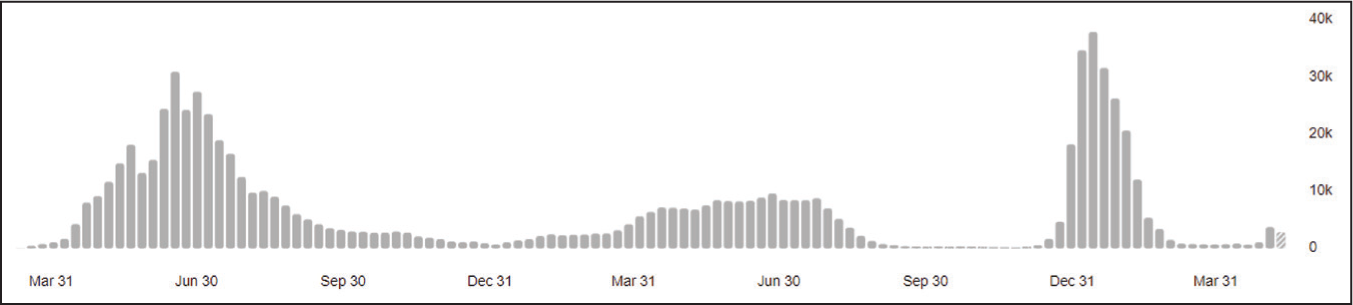
The first case of COVID-19, the infectious disease caused by the coronavirus SARS-CoV-2, in Saudi Arabia was reported by the SMoH on 2 March 2020. About a year later, by the end of February 2021, the total number of cases had exceeded 377,000 (COVID-19 Dashboard, 2021). As can be seen in Figure 1, there are three broad peaks (WHO, 2022). The first one followed the first reported case in the Kingdom. The second peak was much lower, a year after the first peak, and this could be attributed to a nationwide vaccination drive complemented by widespread use of digital tools. By November 2020, digital tools were widely mandated and by January 2021, vaccination drives began with gradual approval of Moderna, Pfizer/BioNtech, Janssen and Oxford/AstraZeneca. It is this period of first year that we are particularly interested in exploring what digital healthcare innovations were pursued. The third peak overlaps with the spread of the Omicron variant, which was first reported to the WHO on 24 November 2021.
Prudently, before the first case was caught, the Saudi Centre for Disease Prevention and Control was hard at work preparing protocols and precautionary measures to equip the medical system to deal with the looming threat. It was not the first time that Saudi Arabia had faced a coronavirus threat; the Middle East Respiratory Syndrome (MERS) was first reported in Saudi Arabia in 2012. This helped the country to be better prepared to deal with another coronavirus threat (Al-Gaissi et al., 2020). Many of the new protocols implemented during the current pandemic were based on existing technologies that the medical system had previously failed to integrate widely, such as telemedicine, medication deliveries and medical prioritisation protocols to grant medical access to the more critical patients first.
As of 20 May 2022, the reported COVID-19 fatalities globally were 808.2 deaths per million of population, while in the KSA, it was significantly lower at only 255 (Worldometer, 2022). The outcome was that the country faced a lower incidence of COVID cases and deaths, and at the same time, it was able to re-open its economy faster than several other well-resourced and developed countries. According to Google mobility data cited by Bloomberg (Nereim, 2021), workplace visits in Saudi Arabia’s major urban areas were down only 6% when compared to a pre-pandemic baseline, versus 50% in Greater London. Saudi Arabia is the largest of all Gulf region countries and its cultural context makes it an interesting case to explore the speed with which it acted to minimise impact of COVID. This led us to our research question: How can the accelerated pace of healthcare innovation and development brought on by a public health crisis in Saudi Arabia be maintained in the future?
In exploring this research question in Saudi Arabia, our paper aims to offer policy recommendations for the country as it pursues a national policy of transformation outlined in the Vision 2030. As a result of the country’s national response to the pandemic, policy lessons are drawn based on what was done during the pandemic and what could next be done post-pandemic. Essentially, this paper suggests that to ensure the pace of innovation remains high and that its impact on healthcare remains positive, the appetite for change among the public and healthcare professionals needs to be managed carefully by prioritising problems and interventions, gathering evidence of need and impact, and by building confidence and trust through education, collaboration and stakeholder participation.
Methods
We conducted an exploratory case study of Saudi Arabia’s response to the COVID-19 pandemic as an ‘innovation in practice’. Our theoretical basis is one of phenomenon-driven research (Ployhart & Bartunek, 2019) to understand what was done during the one-year period following 2 March 2020. We reviewed the SMoH websites and the communications sent out through various channels, including press releases and social media – mainly Twitter and WhatsApp. Additional material from published articles as well as grey literature was identified through a search of international databases, mainly PubMed, EBSCO and Google Scholar, and the local Saudi Digital Library, which documents scholarly output from universities in the country. Most of the local material was in the native Arabic language, although it was also complemented by English language material to cater to the large expatriate population working in the country. Three of the co-authors are medical doctors practising in different public hospitals in the three major regions of the country – Western, Capital City and the Eastern regions. Their personal experiences and interactions with both patients and policymakers helped our understanding of policies and practices in the local context. We thematically organised the data and insights from the secondary material by focussing on the areas of intervention identified by the SMoH, the solutions developed for each area, and the actors involved. We did this from an innovation systems perspective, whereby prioritising domains, around which the various actors and institutions in a country are willing to coalesce, is the main challenge in supporting the innovation system in developing countries (Natera et al., 2019).
Results and Discussion
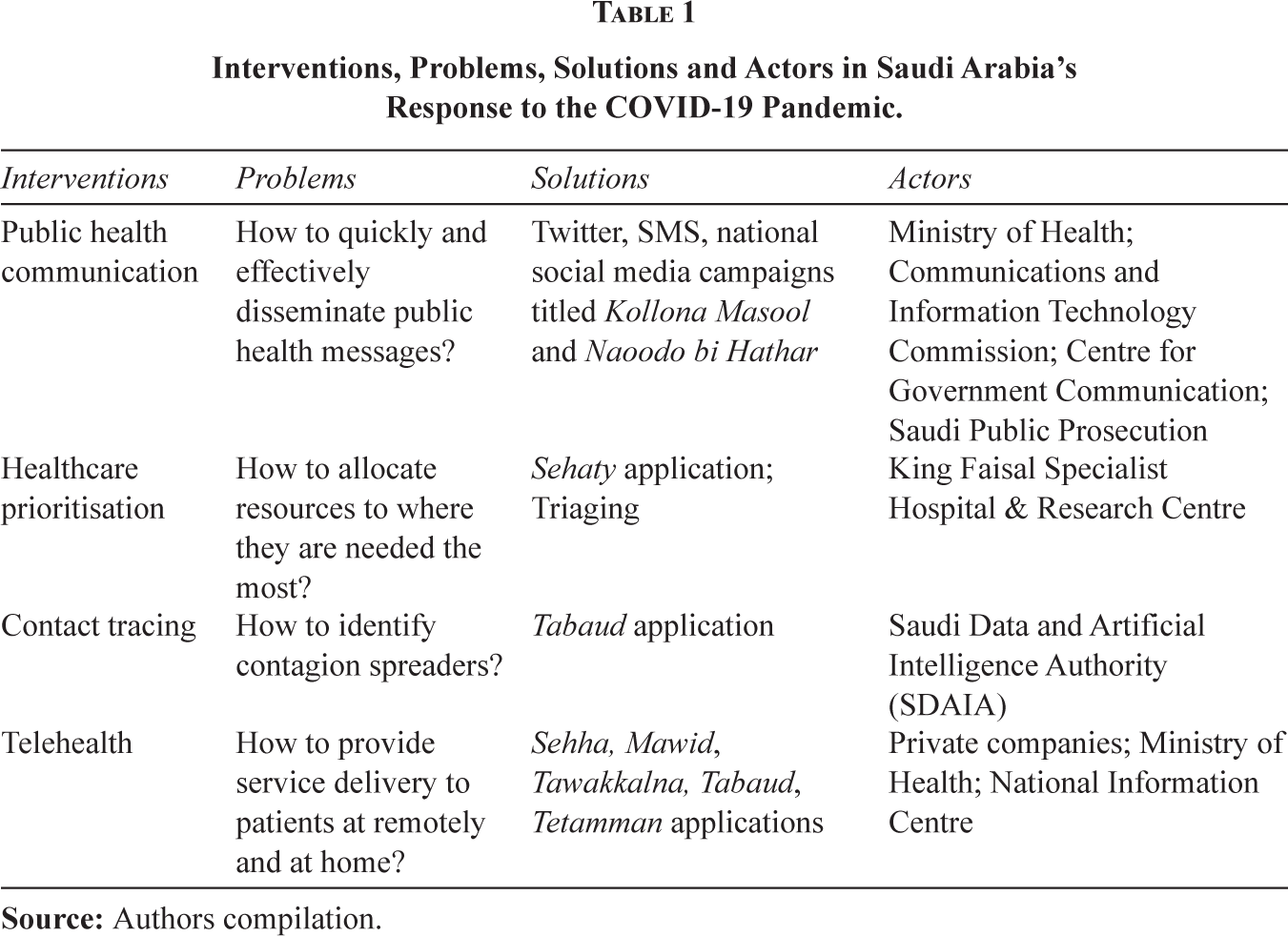
Although many of the initiatives by the SMoH reflect the use of digital innovations, we find the adoption of these science- and technology-based innovations relies on mobilising the country around specific areas of intervention and the developmental agenda and vision that characterise its institutional framework. We find the pandemic, as a public health crisis, helped to identify four areas of intervention in the Saudi Arabian healthcare system: public health communication, health prioritisation, contact tracing and telehealth. This categorisation of interventions focussed strategic action and resulted in transformation at a much faster rate than had been previously witnessed in the country. Table 1 outlines the interventions, problems, solutions and actors we identified.
Interventions, Problems, Solutions and Actors in Saudi Arabia’s Response to the COVID-19 Pandemic.
The COVID-19 public health crisis offered clear areas of intervention and resulted in an accelerated pace of healthcare innovation and development. This in turn benefitted from a reciprocal willingness and appetite among the public and healthcare professionals to adopt these innovations. Technological and digital innovations have served to complement the more important social innovations needed in society to contain the pandemic, such as healthy lifestyles, social distancing and basic hygiene. The leaps made in technological, behavioural and workflow practices in one year would otherwise have taken many years. Some of the delays in adoption are less about patients’ needs and more about testing and auditing by medical firms and institutes who want to protect themselves against liability claims. Other delays are due to reticent providers and users. Both concerns were in large part set aside due to the urgency of containing the pandemic. Based on what we found was done in Saudi Arabia for each of the four areas of intervention, we suggest lessons on how the high rate of change and adoption of innovations could be maintained beyond the pandemic to continue to advance the national innovation and healthcare system towards achieving the Saudi Vision 2030.
Public Health Communication
In 2011, the SMoH joined the Twitter platform to communicate with the public and disseminate information. By 25 December 2020, it had 4.4 million followers, up from 3 million on 25 June 2020 (SMoH Twitter, 2020). Its following had grown by 50% in six months and accounted for almost a quarter of its roughly 20 million citizens. From the time the pandemic started, the SMoH has used its website, social media platforms such as WhatsApp and standard SMS text messages to spread health information and education. Smartphone penetration in 2020 was estimated at 87.4% of the population (Statista, 2020). The topics cover COVID-19, its mode of transmission, prevention and latest updates. These messages have been translated into other languages to ensure the greatest spread of the information among the country’s large expatriate population, which roughly accounts for a third of the total population (SMoH News, 2020).
By April 2020, the SMoH, in cooperation with the Communications and Information Technology Commission (CITC), had broadcast more than 2 billion awareness and information messages (Saudi Press, 2020). The SMoH used Twitter to increase awareness about the COVID-19 vaccine campaign and its benefits. According to the World Health Organisation (WHO), the best method of dealing with rumours and misinformation is to act promptly when rumours occur (WHO, 2018). The SMoH retweeted rumours and negated the false information with correct evidence-based information (Al-Barqawi, 2020). The SMoH also emphasised the importance of retrieving information from reliable sources, mainly official websites and social media accounts. Another major step the SMoH took to contain Internet rumours and false information was to collaborate with Saudi Public Prosecution, whereby spreading or sharing rumours about COVID-19 that cause panic and disruption among the society is deemed an electronic crime. The penalty could be as high as five years of imprisonment or a fine of SR three million (approx. US$800K) (Riyadh Daily, 2020).
Although the threat of a penalty acts as a deterrent, making the public own the problem and its solution is preferable. Social media-based public health campaigns have been effective in generating awareness and bringing about a sense of collective responsibility for managing the pandemic. When restrictions were applied in several major cities, the Centre for Government Communication introduced a national social media campaign titled Kollona Masool, meaning ‘We Are All Responsible’ (Al-Hadhira, 2020). The campaign’s main concept was that people should meet their obligations to their country and society by staying at home. The population, businesses and government entities on Twitter and social media have responded to the campaign by incorporating the Kollona Masool logo into their images. Without social media, it would not have been possible to execute this national campaign in such a short period of time. Once the lockdown eased, this campaign changed to Naoodo bi Hathar, which means ‘Return Carefully’. As society and the economy normalise, the SMoH might continue to mobilise public sentiment and collective responsibility to promote healthy lifestyles. In a third phase, for instance, it could revert to the Eish be Seha or ‘Live Well’ campaign, which was launched only two months prior to the commencement of the pandemic (SMoH e-Platform, 2020).
Healthcare Prioritisation
A relatively new problem that arose during the COVID-19 pandemic is how to distribute limited healthcare capacity. It is accepted that during public health crises, such as influenza outbreaks, human, technical and material resources must be rationed (Challen et al., 2007). Even during normal times, though, resource-rich countries such as Saudi Arabia are beginning to realise that limitless and expensive healthcare provision is no longer a reality. For instance, the bottleneck in the global supply of the COVID-19 vaccine calls for a phased approach to roll-out. Here, the Sehaty app, developed by King Faisal Specialist Hospital & Research Centre, is being used to register and prioritise vaccine distribution. Healthcare capacity must be distributed in such a way that those who need it most have access to it. In Saudi Arabia, the first priority was given to life-threatening cases, second to those who were at risk of normal function being affected and third to those requesting elective interventions that could wait. This process, however, revealed a hidden fourth category: those who did not need healthcare attention to begin with. This final group of patients is given the lowest priority and in some clinical settings, even loses treatment eligibility totally. This frees up space for those who are more in need and offers healthcare centres breathing room to handle the COVID disaster more effectively. However, this fourth category cannot be ignored indefinitely, and alternative means for catering to the needs of all groups should be investigated.
In May 2023, the WHO declared that the COVID-19 is no longer a public health emergency of international concern (PHEIC). A balanced approach to prioritisation might continue after the COVID era. Those who are presumed to be healthy and do not actively seek out healthcare service should be encouraged to come in for regular health assessments, but during periods of surplus capacity. With vaccines having been approved, healthcare systems need to prioritise national vaccination campaigns in rank-order of susceptibility and vulnerability to the coronavirus. The lessons healthcare systems draw from these prioritisation activities should make national systems more resilient in the face of crises. There is some evidence that public opinion about health prioritisation can be favourable (Li-Vollmer, 2010). For any post-pandemic continuation of health prioritisation policies, though, there needs to be greater stakeholder participation. This will require a prolonged effort to decipher and to shape public opinion. Such engagement provides the SMoH an opportunity to manage the expectations of its citizens and offers healthcare providers the means to treat patients better by matching their needs.
Post-pandemic demographic and behavioural trends will define prioritisation and identification of areas of intervention. The census of 2022 will help provide this necessary data to align priorities to the National Vision 2030 transformation agenda for the healthcare sector. During the pandemic, non-communicable diseases (NCDs) and elective procedures were de-prioritised in favour of containing the spread of the virus and releasing capacity in the healthcare system to cope with potential outbreaks. Then, generally healthcare providers, such as in dental healthcare (Javed et al., 2021), were worried about the risk of exposure to themselves and of spreading the virus to friends and family. Although in post-pandemic, attention will need to revert to NCDs and elective procedures and to increase capacity to overcome any backlog. When expectations remain high or remain unmet by the national system and public organisations, the SMoH might collaborate with the private sector to secure added provision of service delivery. These partners might or might not be physically located within the country. For over a century, the dominant model of innovation has been premised on large investments in the physical infrastructure of science and technology; however, the pandemic has made the world more open and more willing to collaborate flexibly (George et al., 2020). In line with the focus of Saudi Vision 2030 to diversify the economy to a knowledge-based economy, there is now an opportunity for the country to reformulate how to develop indigenous science and innovation infrastructure and capacity by collaborating virtually within the country and across the world.
Contact Tracing
Contact tracing is a public health strategy for reducing or even stopping the spread of an infectious disease. It has been a pillar of managing transmissible diseases for a long time. In the past, the steps were: identify an index case; interview the index case to determine movements and then isolate possible further cases. An early example is the case of the typhoid fever epidemic, involving Mary Mallon (‘Typhoid Mary’), a cook who moved to Manhattan in the early years of the 19th century. Authorities found her by tracking down all those who fell ill, and then the circles in which those identified interacted; they did what epidemiologists today would call ‘contact tracing’ (Brockell, 2020). Contact tracing was also used for the eradication of smallpox in the early 1950s through isolation of cases and vaccination of everyone who lived close by. At the time, a major obstacle faced by the WHO team was the insufficient reporting of smallpox cases and coordinated efforts by public health officials. This effort intensified until smallpox was finally defeated by 1980 (Langer & Lane, 2020).
The basic mechanisms of contact tracing have not changed very much. Starting with overlaying the data points on a map of Manhattan during the typhoid epidemic, manual contact tracing progressed to follow-up phone calls from healthcare officials, and finally to what we have today: automated contact tracing using mobile or cellphone apps to warn people when they have encountered someone who has been infected. When faced with COVID-19, the Saudi Data and Artificial Intelligence Authority (SDAIA) launched the Tabaud application to support government and SMoH efforts in tracing COVID patients. The aims of IT-based tracking are to ‘flatten the curve’ faster, optimise case management and decrease the burden on the healthcare systems.
Some would argue against contact tracing through digital means, on ethical and legal grounds, with respect to privacy and restriction on freedom of movement. In the Tabaud app, the use of Bluetooth, instead of GPS, estimates relative distance rather than absolute distance, meaning that no geolocation or personal data are stored or attributed to a user. This has mitigated some of the privacy concerns and helped to increase the take-up of the app. Laws and regulations, particularly during a crisis, can also levy mandatory behavioural changes in how citizens interact with the health infrastructure. However, while the Tawakkalna app was made mandatory to show vaccination status before entering any public space, the contact tracing Tabaud app was highly recommended, not required. A study showed that the number of active daily cases in one major city decreased by 61% between November 2020 and March 2021 following the implementation of the Tawakkalna app (Khan et al., 2021). The Tawakkalna app won the United Nations Public Service Award 2022 in the category of institutional resilience and innovative responses to the COVID-19 pandemic (Arab News, 2022). In moving towards gaining more public confidence and trust, authorities should formulate a transparent policy that outlines who has legitimate access to the information and how data are used at the individual, anonymised and public levels.
Telehealth
The higher demand for medical services due to COVID-19 also increased the risk of infection transmission from patient to healthcare staff and vice versa. This led to the closure of many non-emergency based medical services in Saudi Arabia, including out-patient clinics. Many patients, however, and particularly those with diabetes, cardiac illness, cancer and many other diseases, need periodic health assessments. These patients also happen to be those among the population with the highest risk of developing COVID-19 complications (CDC, 2020). Therefore, there was, a need to accelerate the SMoH e-Health strategy and advance the utilisation of telehealth technology (SMoH E- Health, 2018). ‘Telehealth’ and ‘telemedicine’ are broad terms that refer to remote medical consultation clinics, remote health education, electronic prescriptions and even remotely administered robotic surgery (Mermelstein et al., 2017). The utilisation of this technology in Saudi Arabia came in several forms. Inside hospitals, medical professionals shifted their priorities in the clinic to see critically ill patients or patients that required clinical procedures, while following up with other chronic patients – especially children and vulnerable people – by phone. This has helped to lower the number of nonessential visits to hospitals, reducing the chance of infection for patients and healthcare professionals. Healthcare systems around the world have struggled to remain fully operational on account of staff being overworked and stressed and having to isolate themselves following a COVID-19 breakout. Although staff in Saudi Arabia have also experienced depression and stress during the pandemic, we have not observed significant loss of healthcare provision on account of staff absence due to COVID-19 infections among healthcare professionals (Arafa et al., 2021).
A suite of mobile applications enables users to book appointments, refill prescriptions, book a COVID-19 swab and easily self-diagnose and report to authorities about their condition (Hassounah et al., 2020). Some of these apps, such as Sehha and Mawid, were already in use but updated to cater to COVID mitigation and management. Other apps such as Tawakkalna, Tabaud, Tetamman and Sehaty were developed and launched during the pandemic. For instance, both Tetamman and Tawakkalna were launched in April 2020 and by February 2021, the latter was begun to be used to gain access to public places. The apps were developed by the SMoH, the National Information Centre and private companies. They are used for symptom checking, self-management, tele-consultation, e-prescription, contact tracing, travel permits for exceptional circumstances during curfew and lockdown and for COVID-19 vaccination. The digital applications were used by both genders throughout society, and we did not see evidence of any significant differences regarding availability to or adoption by different genders. The Tawakkalna app has moved on, however, by becoming a general status report for each resident and visitor to the country. General information about an individual’s residency status and health status, such as blood group, allergies, emergency contact and insurance provider, are readily available. Its other features can be adapted to enable access to health services beyond COVID-19 testing and tracing. The application’s permit system for visiting the Grand Mosques in Makkah and Medina, for example, can be retained to avoid congestion and provide ease to elderly and vulnerable visitors to gain priority access to religious sites and to healthcare facilities.
These technologies have not only helped improve the quality of healthcare and make it easier for patients to access them but have also significantly lowered the cost of providing services (Al Otaibi, 2019). The introduction of these technologies to the healthcare system in Saudi Arabia can be considered a frugal innovation because it offers a new way of delivering healthcare at a much lower cost (Harris et al., 2020). As Saudi Arabia struggles to balance its budget and make its economy more sustainable and less dependent on oil, it will find merit in managing its healthcare resources more efficiently. Therefore, the use of these technologies is likely to continue even after the pandemic ends. Saudi Arabia is the 13th largest country in the world in terms of area. In such a vast country, many traditional tribes and families choose to retain their nomadic Bedouin roots. Hence, a hybrid healthcare delivery model may be retained drawing on the accessibility offered by telehealth.
Policy Lessons
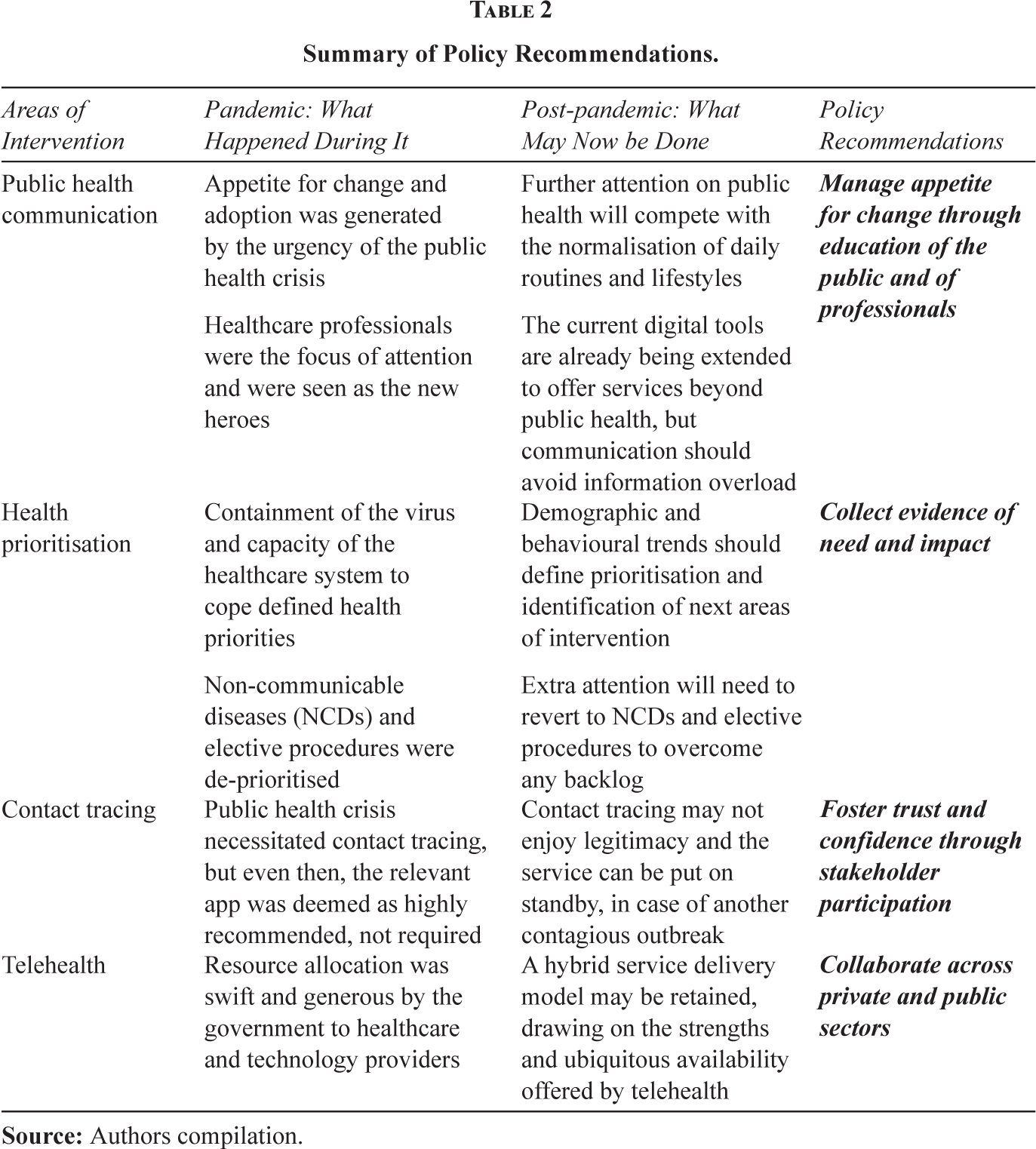
Although the paper began with a focus on digital innovations as technological in nature, we eventually discussed the relationship of these technologies to the institutional and organisational conditions in the society. With the gains made in developing and diffusing several digital innovations into the healthcare system as well as the into the public, the focus of the government should now be to ensure that national innovation activity is sustainable and that the impact on healthcare remains positive. We have outlined above potential improvements for each of the areas of intervention in the Saudi healthcare system: public health communication, health prioritisation, contact tracing and telehealth. In this section, we suggest policy lessons for Saudi Arabia, which might also be relevant more generally for the Middle East. Innovation policy could assess the appetite for change among the public and healthcare professionals, manage it carefully through evidence gathering of need and impact, prioritise problems and areas of intervention, and build confidence and trust through education, collaboration and stakeholder participation. Table 2 presents a summary of the policy recommendations as they stem from how the four areas of intervention were dealt with during the pandemic and how they may now be addressed post-pandemic.
Summary of Policy Recommendations.
Manage Appetite for Change Through Education
During the crisis, the general population was largely receptive to instruction and guidance from government authorities on how to deal with the pandemic, and therefore, people downloaded many digital applications. Healthcare professionals were the focus of attention and were seen as the new heroes. However, that high degree of public acknowledgement and receptiveness might not retain the same intensity. People forget and move on, and the pandemic is one thing humanity is all too ready to move on from. The educational campaigns during the pandemic disseminated valuable information on collective responsibility among all residents. A continuation of such national campaigns that educate the public and professionals of the value of innovation and change should keep the momentum alive for continued adoption of new technologies. With many of the digital tools we have outlined here already installed by most of the population, it is a positive step that these tools are already being extended to offer services beyond the public health. This will help to retain user engagement and serve as a conduit to push through to the public new solutions.
Collect Evidence of Need and Impact
The SMoH developed dashboards to monitor the spread of the virus and its impact. These dashboards collect real time data from integrated sources. These efforts tie in with the SMoH’s national telehealth strategy, which, as part of the Saudi Vision 2030, seeks to improve the availability and quality of healthcare in Saudi Arabia by utilising healthcare technologies, including telehealth (SMoH E- Health, 2018). Big data mining and artificial intelligence can be applied to the huge amount of data that have already been collected, to pre-empt other public health emergencies and to prioritise health services to where they are needed the most. Plans are underway to restructure the health system into a more devolved structure (SMoH, 2021). The gathering of evidence on the performance of the transformed health system through the national dashboards is necessary, however, to ensure that greater effectiveness is being achieved. Further developments in implementing the national telehealth strategy can be accomplished by evaluating user satisfaction and the impact on health outcomes on a regular basis. For instance, there is a risk that the elderly population, which is also most vulnerable to COVID-19 complications, might not be using the applications to their full potential. Therefore, we need more evidence on how COVID-triggered apps were perceived and used based on local expectations and cultural norms and which health outcomes can be afforded for the various priority problems and areas of intervention. At the same time, data collection and data mining efforts should be balanced against privacy concerns of patients in particular and the population in general. Insights gathered by digitalisation and big data not only offer profound benefits to society and to individuals, but also put both at risk of fraud, theft and intrusion into personal rights (Cherif et al., 2021). Progressive societies should be inclusive but also respectful and mindful of the boundaries between family and work. For instance, the contact tracing technologies may no longer enjoy legitimacy beyond the pandemic and the service can be put on standby, in case another contagious outbreak occurs. Culturally, Saudi Arabia and the Middle East have long been both very ‘private’ and ‘public’ societies, with a clear demarcation between the two. Maintaining this balance during the transition to greater digitalisation will be tricky, but necessary for long-term success of any innovation and change initiative.
Foster Trust and Confidence Through Stakeholder Participation
Collaboration and stakeholder participation improve innovation, as posited by advocates of open innovation (Wayne, 2012). In Saudi Arabia, the prevailing producer or supply-driven innovation paradigm has worked for dealing with the crisis, but it might consider a shift toward a user-driven paradigm (Gambardella et al., 2017). New product and service development relies on user input, feedback and iterative testing (Bosch-Sijtsema & Bosch, 2015). We have not come across evidence of wider stakeholder involvement in the development of the digital innovations during the pandemic. This is understandable during a crisis, when a rapid response is essential (Bhatti et al., 2020). However, any strategic, long-term transformation effort can be more sustainable by developing a culture of trust, confidence and ownership through stakeholder participation and collaboration. In moving towards long-term innovative activity and healthcare transformation, the greater the involvement from the public and the general user, the greater the likelihood of better outcomes and the sustainable adoption of innovation (Ayuso et al., 2011). Neither have we seen in the Middle East region – which is not to suggest that it is not there – homegrown, community-led efforts to innovate, as evidenced elsewhere (e.g., Ramadi & Nguyen, 2021). Our analysis of the actors involved suggests that resource allocation was swift and generous by the government to healthcare and technology providers, but mostly to large companies and that too public ones. An excessive reliance on institutionalised or specialised decisions might discount the benefits that innovation affords from ideas based on experimentation and adaptation (Sørensen et al., 2010). The pandemic gave the Middle Eastern region an opportunity to rely less on resource extraction, importation of externally developed solutions and supply-driven offerings. The Middle Eastern resource-rich countries have populations among those with the highest proportions of youth; in Saudi Arabia, children and people under 35 accounted for 67% of the population in 2020 (General Authority of Statistics, 2020). Globally, the youth have confidence in their abilities to contribute and are calling for more democratised innovation models that promote sustainability (von Hippel, 2005; Han & Ahn, 2020). Therefore, it becomes even more imperative to include the youth as stakeholders in the future towards which they will lead the country.
Collaborate Across Private and Public Sectors
The development of innovations is easy, but diffusion is hard (Berwick, 2003). Given the political structure and cultural norms in Saudi Arabia, it is not difficult for the authorities to mobilise the population to adhere to policy guidance and rules. The Middle Eastern population, in general, looks up to the leadership and follows through in line with government decisions. That is a strength of the region’s cohesiveness and its collective drive to develop and prosper. Consequently, the deployment of several digital healthcare innovations in the Saudi Arabian context has been facilitated by the society’s acceptance and observance of the policies set out by the country’s monarchy-based leadership. Also, the use of various communication channels including social media helped to spread the message throughout society. Deployment and adherence to the digital applications stemmed from awareness campaigns as well as regulatory fiat. At the same time, when this mobilisation is done from the bottom-up, through grassroots initiatives and behavioural nudges, there is evidence that the uptake of new practices can be more sustainable (Smith et al., 2018). Bottom-up approaches can also lessen the onus of innovation on the government and make innovation less costly, such as through frugal innovation (Bhatti et al., 2017). Throughout the region, governments, such as that of Saudi Arabia, have exhibited an entrepreneurial spirit to transform the public sector (Weiss, 2021) during this crisis. The impetus for many of the digital innovations that we have discussed in this paper came from the SMoH; but, in order to enhance the data and tele-communication infrastructure and to sustain these advancements efficiently, it might explore the possibility of delegating future management and improvements to the private sector. As the region looks to diversify its economy and make the population less reliant on government jobs, entrepreneurial activity and, therefore, innovative activity from the private sector working closely with the public sector should become a core lever of diversification.
Conclusion
The COVID-19 pandemic accelerated healthcare transformation in Saudi Arabia at a faster pace than that was perhaps planned for in the Saudi Vision 2030 policy. In many countries around the world, the uptake of medical innovations prospered during difficult times and regulatory authorities were quick to enforce change around key needs and areas of intervention. The focus of innovation here is the speed with which the pandemic needed to be contained and managed. We have outlined Saudi Arabia’s experience in terms of the speed and widespread implementation of the digital tools, discussed the challenge of maintaining this success and have offered policy recommendations for the country to leverage this fast pace of development and adoption to develop its national innovation system. Drawing from Saudi Arabia’s experience, this paper concludes that to ensure the impact on healthcare remains positive, the current appetite for change in the public and among healthcare professionals needs to be managed carefully through problem and intervention prioritisation, evidence gathering, confidence and trust building measures, collaboration and stakeholder participation. What remains to be seen is whether this appetite for change in the public and the authorities will carry on into the future. Nevertheless, Saudi Arabia and other countries should look to maintain this momentum, while taking into consideration the behavioural and cultural expectations of the public and determining how best its institutions can meet those expectations. The opportunity for innovation brought about COVID-19 should continue and become part of the ‘new normal’ for future development.
Footnotes
Authors’ Contribution
Conceptualisation, design of the article, initial research, and first draft (AAA, AMA, ASA, FNA, MSA); additional research, revisions, and final drafts (YAB, AAA, MAR); Approval of final draft (All).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research received no external funding, but the article processing charge for open access was paid for by the MBS College of Business and Entrepreneurship, Saudi Arabia.