
Abstract
From politicians to physicians, the opening years of India’s plague epidemic (1896–1900) have conventionally been treated as a male-dominated sphere of activity. This article argues for the centrality of female actors—as doctors, nurses and ‘ward ayahs’—and across the social spectrum from dalits to Europeans. Photography demonstrates the prominence and diversity of women’s plague roles; it helps to complicate a text-based narrative of plague at the intersection of gender, race, class and colonialism. Images augment and not merely document. The value of combining visual and textual sources is underscored by focusing on a single institution, the General Plague Hospital in Poona (Pune) and on a woman doctor, Marion Hunter, whose photographic presence and whose views in and after India highlight the tensions and contradictions of a gendered as well as racialised imperial presence.
Introduction
Before the coronavirus of 2019–2020 and apart from the influenza of 1918–1919, India’s single most devastating encounter with disease in modern times was the pandemic of bubonic plague that struck the country in 1896. Deadly from the time of its arrival in Bombay (Mumbai), the pestilence spread into most parts of the subcontinent and resulted in 12 million deaths before it began to wane in the 1920s. In recent decades the Indian plague episode has been widely discussed by scholars and many aspects of its demographic, social and political history have been critically examined (Arnold, 1993; Chandavarkar, 1998; Catanach, 1984; Echenberg, 2007; Klein, 1988). There is, however, one respect in which the plague episode has been insufficiently addressed and that is in relation to gender, or more exactly, the interplay of race, gender and medicine at the height of British rule in India.
Epidemics in India, as elsewhere, are generally written up in terms of the heroic male and dynamic masculinity; or, as in case of India’s plague, in terms of women’s bodies as a site of contestation for both Indian and European men. Yet what is remarkable about the plague episode in India is the prominence and diversity of women’s roles and women’s voices—women as factory workers and hospitalised victims in Bombay; women as propitiators or avatars of the female plague deity; women, Indian and European, as an articulate and active public presence in ways not evident in earlier epidemics of smallpox and cholera (Arnold, 2022, pp. 91–97). Moreover, apart from elite and middle-class women (whether critical observers like Pandita Ramabai, Sister Nivedita and Lakshmibai Tilak, or as doctors and nurses), dalit women were extensively employed in plague hospitals and segregation camps as ‘ward ayahs’ or assistants; they, too, have a neglected, subaltern, history deserving to be told.
In the medical and sanitary publications of the time, as in more recent historiography, it is men who dominate the narrative. They are the doctors, administrators, researchers and politicians who make the decisions or dispute the intrusive power of the state; it is men who seek to enforce the new sanitary order or who, in laboratories and research institutes, committees and commissions, pioneer new medical research or commend policy initiatives. It is a man—the Russian-born bacteriologist Waldemar Haffkine—who devised the prophylactic against plague that became such a central feature of colonial attempts to control the disease (Schama, 2023). It is a man—Brigadier-General W. F. Gatacre—who chaired the Plague Committee in Bombay in 1897–1998 and sought to stem the tide of contagion in India’s worst affected city; it was again a man—Bal Gangadhar Tilak in Poona (Pune)—who most powerfully articulated the nationalist critique of colonial plague policy, and likewise a man—W. C. Rand, Poona’s plague commissioner—who was assassinated in June 1897 for his heavy-handed attempt to rid the city of plague. In all this male-centred narration, we risk overlooking the pivotal role of women in the early plague years and the way in which issues of gender, in conjunction with race ideology and class privilege, complicated the plague story. Recent commentaries (e.g., Bhattacharya, 2022) have begun to pick away at this male façade; the issue, however, merits further enquiry.
Much of the evidence for female engagement and experience lies in archival records and other textual material. But it is to be found, too, in visual sources, for women in all their roles were a highly visible presence in the extensive photographic documentation on plague in western India between 1896 and the early 1900s. As Sumathi Ramaswamy has argued, ‘no history of imperialism is complete without heeding the constitutive capacity of visuality… Images interrupt and realign the flows of a textually driven colonial and postcolonial scholarship’ (Ramaswamy, 2014, pp. 11–12). One of the ambitions of this article is, accordingly, to bring the visual and the textual into line, to suggest ways in which photographs augment or contest other sources, and, through a combination of image and text, to bring into focus one central figure, Dr Marion Hunter, at Poona’s plague hospital.
Plague as Women’s Work
Rather than conceiving of bubonic plague as a bacteriological bolt from the blue, we can think of the early plague years as occurring at an important juncture in the history of women, medical education and female health workers. Since the 1860s, the women’s medical movement had gained strength in India. A growing number of qualified women from outside the country had taken up posts there, whether in the service of missionary organisations or in civil hospitals and local health services. The establishment of the Dufferin Fund in 1885 to finance the provision of women doctors in India was a seminal moment in an already ongoing development; so, too, was the opening up of educational opportunities to women in India’s medical colleges (Balfour & Young, 1929; Lal, 1994). In 1895, the fund’s management committee reported that it was supporting nearly 90 medical women in India, including 18 ‘lady doctors’ as well as assistant surgeons and hospital assistants, with more than a million patients treated in its many subsidised institutions. Bombay was one of the provinces where the movement was most successful (Countess of Dufferin’s Fund, 1896, pp. 9, 15, 68–70). Although the formation of a Women’s Medical Service to complement the exclusively male Indian Medical Service (IMS) was more than a decade away, by the time of the outbreak of plague in Bombay in 1896, these initiatives had begun to bear fruit in the number of women doctors, nurses and midwives and the specialist medical institutions catering specifically for women, and, led by Bombay’s Cama Hospital, staffed primarily or exclusively by women.
Photography attests to this growing female presence. Since 1884, women had been admitted to Grant Medical College in Bombay as students and an album of photographs of the college and associated hospitals from the early 1900s shows female doctors and medical students as well as women nurses, alongside their male counterparts (Dimmock album, 311/2: 22–26, 28–33). To judge both by the images and by enrolment records, these women were drawn from a diversity of ethnic backgrounds only possible at the time, among Indian cities, in Bombay—‘domiciled’ Europeans, Anglo-Indians, Indian Christians, Jewesses, caste Hindus and Muslims (Countess of Dufferin’s Fund, 1896, p. 212). Women were entering other professions, too, by the 1890s, especially education, and as social reformers were an increasingly conspicuous and articulate presence (Forbes, 1996). Plague arrived, in other words, at a time when women, for all the many obstacles and discriminatory practices they still encountered, were more active and visible in public life and professional roles than they had been even a few decades earlier.
Just as purdah and the cultural sensitivities surrounding the medical investigation and treatment of female bodies by male physicians gave impetus to the women’s medical profession in India, so did colonial plague policy contribute to the gendering of medicine and public health. Under pressure from the international sanitary conference at Venice in early 1897, as well as its own fears about the loss of overseas trade and internal revenues, the Government of India moved with unprecedented speed and severity to contain the spread of bubonic plague. Its primary response, the Epidemic Diseases Act of 1897, imposed stringent measures on the people and places affected, or threatened, by plague. These included house searches, compulsory hospitalisation of the sick, enforced removal of suspected cases and contacts to segregation camps, the destruction of infected homes and property, and the physical examination of rail and boat passengers—all measures that in one way or another impinged directly on women’s lives and women’s bodies. First in Bombay, then in Karachi and Poona, sanitary officers and British soldiers were brought in to enter homes and search for plague suspects or concealed corpses. Most provocatively of all, women travellers were physically examined at railway junctions, turned out of their carriages to have their temperature taken or their neck, armpits and groin searched for buboes and other signs of the disease. Such interventions, often conducted in an aggressive and culturally insensitive manner, caused an outcry. Inflamed by wild rumours, spread by word of mouth and newspaper reports, there was mounting anger among many sections of the Indian population at the way in which women were being ‘violated’—in their homes, in hospitals, on railway platforms, in segregation camps (Arnold, 1987). The general alarm fuelled intense opposition to colonial plague measures—including attempts to stop women being taken to hospital or carted off to segregation camps. In May 1897, Pandita Ramabai alleged that a girl from her refuge for widows and orphans had been ‘seduced’ while in Poona’s plague hospital (Bhattacharya, 2022; Ramanna, 2012). Her claim aroused considerable controversy since it constituted a wholesale indictment of the hospital and its treatment of women, not just because it highlighted an alleged attack on a single female patient (ToI, 15 September 1897, p. 4; 7 October 1897, p. 4). Gopal Krishna Gokhale took up this cause, but the authorities strenuously denied the allegation and he was forced to retract (Nanda, 1999, pp. 110–114). 1 Even so, the rumours and claims of mistreatment persisted.
The regime appreciated, almost from the outset, that its highly interventionist plague policy would significantly impact on women. One of its first measures, taken as early as February 1897, was to deploy European or Eurasian women doctors and nurses to examine female passengers (especially those in purdah) at the main railway junctions or arriving by sea. 2 One of the photographs in the album compiled for General Gatacre (the ‘Gatacre album’) to document the work of the Bombay Plague Committee in 1897 shows two ‘lady doctors’ examining women arriving from an infected plague port. 3 One of these was almost certainly Miss Da Cunha, who had recently qualified with a Licentiate in Medicine and Surgery degree from Bombay University. First engaged in February 1897, she was reappointed the following year for as long as the emergency lasted. 4 Contemporary images also show nurses or nuns attending the sick in general hospitals or on plague wards. In the Gatacre album, almost half of the photographs show women, including a white woman participating in house-searches in Bombay. Other images show Indian women as plague patients (or corpses) or, occasionally, as a female relative sitting alongside a hospital patient (Jennings, 1903, plate 12). But, viewed within the wider context of colonial visual culture, this was a racial repertoire of images, an optic conversation about Indians rather than a dialogue with them, even when colonial plague policy was modified to allow for greater Indian participation. It is Indian women who are sick or are ministered to, just as it is European (or Eurasian) women who do the inspecting, the nursing, the feeding and supervision of ‘native’ plague victims.
It was decided in London and Calcutta that the local recruitment of plague auxiliaries was insufficient to meet the severity of the rapidly unfolding crisis and to convince India and the world that the British were earnestly seeking to suppress the epidemic. Given the regime’s racial assumption that Indians were not disciplined or resolute enough to perform such exacting tasks, from March 1897, scores of additional doctors and nurses were recruited from Britain.
5
As a Bombay despatch regarding the employment of plague doctors stated in August 1899:
Natives of India [currently resident in Britain], though qualified, [are] not recommended, as they command no more respect than medical practitioners with local qualifications. Those who have been studying in England for years are nearly as much out of touch as the English doctors who have not been in India before. The influence of the English gentleman in carrying out plague work is what is wanted.
6
As far as women were concerned this recruitment drive principally meant enlisting nurses, more than 50 of whom were rapidly selected from British hospitals and colleges for service in the worst affected towns and cities of India. 7 This influx of British medical personnel was an extraordinary act of intervention, characterised by some critical commentators as an ‘invasion’ (ToI, 10 October 1899, p. 4). It ran counter not just to the increasingly anti-colonial mood in India, but also to the growing Indianisation, or at least localisation, of India’s medical services. The great majority of the white doctors recruited were men, but at least three were women. In its 1895 report, the provincial committee of the Dufferin Fund had doubted that more European women doctors would be needed for Bombay (there were already eleven at Cama Hospital alone); they were too expensive for a poor country like India to afford and anyway life in an Indian town was ‘a very severe trial to the health of most English women’ (Countess of Dufferin’s Fund, 1896, p. 86). A year later, plague seemed to have changed all that.
One of the doctors recruited was Alice Corthorn, aged 38. Having qualified with an MB degree, at the time of her appointment in January 1898 she was a demonstrator in physiology at the London School of Medicine for Women. On arrival in India, she worked at Cama Hospital, then in the southern Deccan, Poona and Karachi, only leaving India in 1902. 8 Corthorn wrote a much-cited report on plague operations and inoculation procedures in Dharwar in late 1898; her observation that plague might be transferred by squirrels and monkeys as well as rats became a significant footnote in ongoing plague research (Corthorn, 1899; Corthorn & Milne, 1899; Schama, 2023, pp. 293–295). Another woman doctor appointed at the same time was Margaret Christie, 30, an MD from London, sent to Bengal, about whom I have no further information. 9 The third, Marion Hunter, we will return to shortly.
English Nurses
The nurses were chosen from a wide range of medical institutions in Britain, most having no previous experience of India. They were sent to India on short-term contracts and on highly favourable terms. Those appointed by the Secretary of State for India in March 1897 were given an outfit allowance of £10, a generous luggage provision, and a second-class return passage to Bombay, conditional on completing a year’s service. They were to be between 28 and 35 years old, with at least three years’ hospital training; they were required to sail within a week of being notified of their selection. Their pay was two or three times that of locally trained nurses (ToI, 14 October 1899, p. 4). As well as working in hospitals and on plague wards, nurses were assigned various other gender-specific duties: one, for instance, was deputed to examine female plague corpses in Broach (Condon, 1900, p. 157). Some fell sick from various causes; three died from plague—one in Bombay, the others in Poona and Belgaum (ToI, 18 February 1898, p. 5; 24 February 1898, p. 3; 6 September 1899, p. 5). But most completed their terms of service; several were permitted to stay on at the expiry of their contracts and join the Indian Nursing Service. 10
The nurses frequently appear in plague photographs, at work in the wards or posing for the camera outside their hospitals, smartly turned out in starched white uniforms, wearing caps or straw boaters. But, however keen their commitment, their practical value was questioned. To some extent they were a conciliatory political gesture—to show that Britain cared about India and acknowledged its women’s need. Their unfamiliarity with India, and perhaps a degree of racial arrogance towards their Indians patients, did not make them popular either with many resident doctors or among the public they were intended to serve. J. P. Barry, one of the medical officers overseeing plague operations in Poona, was scathing about the English nurses, remarking that they were enthusiastic but of little practical use. ‘Ignorance of the people, their speech, their tastes, their food, handicapped the nurses insuperably’, he wrote. ‘The language of pantomime is wearying to patient and nurse. Their presence was glorious, but it was not nursing’ (Supplement to the account of plague administration, 1897, p. 23). The nature of the nursing required was itself a matter of debate. A correspondent of the Times of India remarked, perhaps in a reference to patients’ often violent delirium or resistance to treatment, that ‘plague nursing is … of a kind that needs strong men rather than gentle women’ (ToI, 18 February 1898, p. 5). Conversely, Dr Lloyd Jones at the farewell event held for Marion Hunter in Poona observed: ‘success in the treatment of plague depends largely on nursing … nursing was three-fourths of the battle in plague’ (ToI, 18 February 1898, p. 3).
There was a further issue. By the 1890s, there were many trained nurses in India already—including ‘domiciled’ Europeans, Anglo-Indians and Indian Christians—and many of these were outraged at being denied such well-paid positions and resentful of what they saw as their exclusion in favour of what one indignant nurse described as ‘imported English hands’ (ToI, 5 November 1897, p. 5; also, 9 October 1899, p. 3; 11 August 1900, p. 7). A correspondent writing to the Pioneer newspaper in May 1898 complained that English nurses might be ‘ever so clever in other ways, but India is India; they arrive inexperienced in her ways, ignorant of the language and with an imperfect knowledge of all those methods for plague treatment with which their Indian trained sisters, who have borne the heat and burden of the day, have long been familiar’. They could, the writer continued, ‘only gain practical knowledge at the risk of valuable human life’ (ToI, 17 May 1898, p. 6). Writing on behalf of the Anglo-Indian Association in July 1898, James Cleghorn protested at the way in which ‘local talent of suitable quality’ was being overlooked to the detriment of Eurasians and domiciled Europeans in favour of doctors and nurses who had no experience of tropical diseases, knew nothing of local languages, customs and religious ‘prejudices’. This, he too warned, was ‘a serious mistake’. 11
Some of the newcomers were themselves unhappy with the circumstances in which they found themselves. A correspondent for the Lancet, writing from India in May 1899, referred to the ‘many complaints’ made by the doctors and nurses recruited from Britain for plague work. Nurses were confronted by an unhelpful bureaucracy and faced ‘official difficulties’ even in getting their pay, their accommodation was ‘inadequate’, and there was ‘unreasonable opposition’ to a few days’ casual leave. Further, there was ‘bad management with respect to duties, and insufficient subordinate native assistance’. The article concluded: ‘as far as the English medical men and nurses are concerned there seems to be an official passive resistance against them’ and ‘an entire want of liberality of treatment … unnecessary difficulties are continually being placed in their way’ (Lancet, 27 May 1899, pp. 1458–1459).
Ward Ayahs
There were many tasks nurses in India preferred not to perform. They seemed happy to dispense medicines, take temperatures, tidy beds and prepare patients for examination. But, given the choice, they wanted nothing to do with the more unpleasant side of nursing—emptying bedpans, clearing up diarrhoea and vomit, and all the other chores that might make a plague ward—or any hospital—an unpleasant place to work in. This was a source of long-running controversy, as can be seen from a dispute at Cama Hospital in 1913 when Hindu, European and Indian Christian student nurses protested against the Lady Superintendent’s insistence that they perform such ‘obnoxious’ duties as removing soiled bedpans and cleaning up patients’ vomit. This, they declared, was the duty of matheranies (mehtaranis or women of the sweeper caste), not nurses. 12 Indian nursing needed an underclass.
Particularly informative in this regard are a series of photographs taken at Poona’s plague hospital in 1897–1898. 13 The pestilence had reached that city in December 1896 and by late May 1897 had caused 1,481 known deaths (officials estimated the true figure to be double that number). But the appointment of Walter Rand as plague commissioner and the ‘stringent measures’, he adopted created widespread ‘distrust and alarm’ among the city’s Indian population (Supplement to the account of plague administration, 1897, pp. 1–7). In February 1897, a General Plague Hospital, consisting of tents and chhappar (thatched) huts (some roofed with corrugated iron), was erected at the Sangam, an open space just outside the city. More accurately described as ‘a camp’, it was reputedly the largest plague hospital anywhere at the time with accommodation for 500 patients. 14 Plague patients from Sassoon Hospital were transferred there, Dr Lloyd Jones, IMS, took charge, and in April the first ‘English nurses’ arrived (Supplement to the account of plague administration, p. 29).
Sassoon Hospital was viewed by at least a section of Poona’s population as a place where patients were taken only to die, to be poisoned or killed (Mahratta, 20 December 1896, p. 1; Hunter, 1898, p. 1013). But the new hospital, devoted only to the treatment of plague, was an attempt to create a sanitary enclave, a more controlled and disciplined environment than was considered possible in the crowded, rat-infested city. Photographs taken of the spacious site reinforce the Foucauldian impression of colonial biopower in action, with a guard-post at the entrance, neat rows of single-storey huts, and (seen from an elevated vantage point) the open spaces between the wards, the observation and isolation tents, the cookhouses and disinfecting apparatus. The hospital was intended to ‘gain the confidence of the natives’, to reassure them that they would be well looked after and their religious, caste and gender concerns respected; it had caste cooks and separate caste and communal wards (Hunter, 1898, p. 1013). There were, though, almost from the start complaints in the local press that caste observances were being ignored. In the words of Tilak’s Mahratta (5 December 1897, p. 3), the hospital ‘fills the hearts of the patients and their relatives with dismay’. Poona’s high-caste residents were urged to use the Hindu plague hospital instead, where female patients were treated more respectfully and in accor- dance with their ‘habits and customs’ (Mahratta, 16 May 1897, p. 1; 23 May 1897, p. 5).
Colonial photography is both partisan propaganda and empirical evidence. The ‘work’ photography was required to do during the epidemic was extremely varied and did not represent a single perspective (Arnold, 2021; Sarkar, 2021; see also Jennings, 1903). Many photographs may simply have served the owner’s desire for a record of his or her years of Indian service (hence their incorporation into personal albums); others more clearly served a public, propagandistic purpose. Some photographs appear, in the new age of handheld Kodaks, to have been snapshots taken by amateurs, while a substantial number, including several of the hospital staff in Poona and of plague operations in Bombay, were the work of F. B. Stewart, a professional photographer based in Poona’s cantonment. In one of the images Stewart took at the plague hospital, in early 1898, Europeans sit at the centre of a wide panorama—two white male doctors (Drs Lloyd Jones and Adams), but also a woman doctor (Dr Marion Hunter), with a Eurasian medical officer (Dr Erasmus Dias) between her and the Nursing Superintendent, Mrs Wheatley (Figure 1).
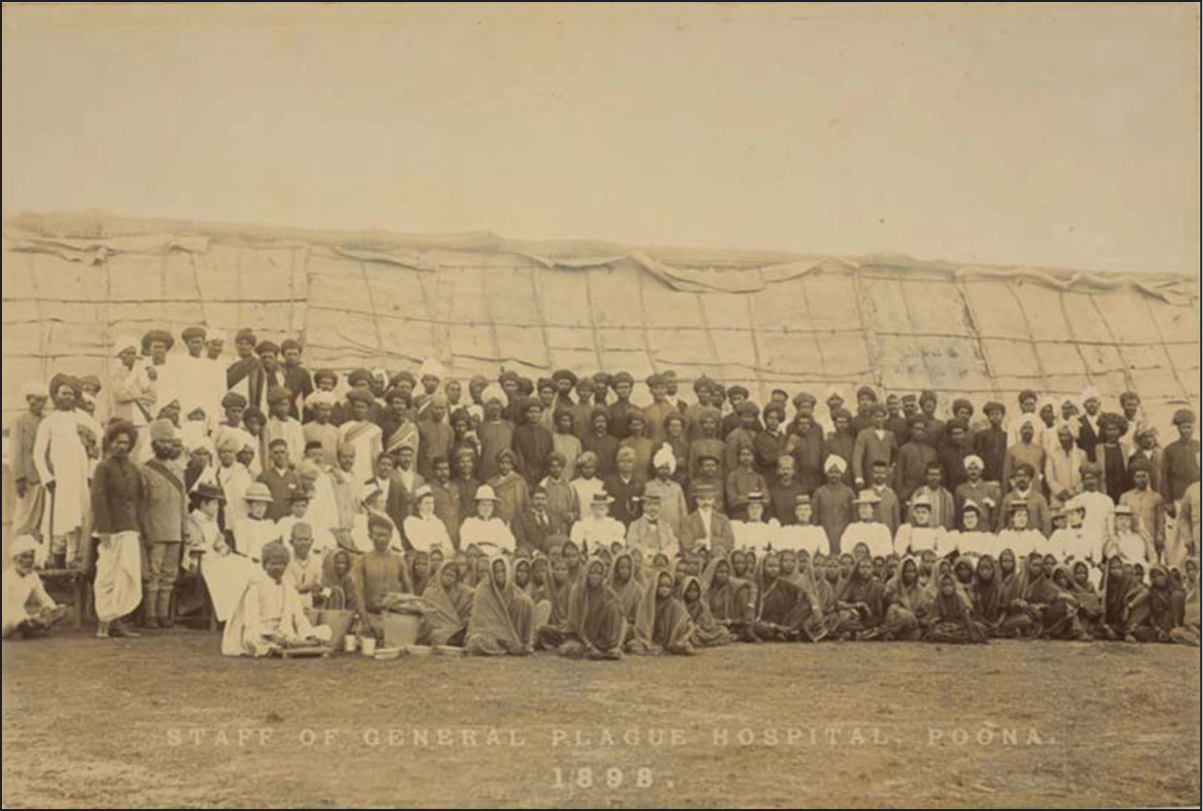
Ranged on either side of them to the left and right are the English nurses: like the doctors, they are individually named in some copies of this image. Behind them and at the sides are the Indian subordinates—from clerks and compounders to the cook with his rolling-pin, the dhobi (washerman) with his buckets, the chowkidars (watchmen) and so on. In its composition, this photographic image is akin to many other group photographs then and since—some sit on chairs, some stand, some perch on benches at the back, others occupy the ground in front. But in the context of British India, the composition evokes another visual idiom—the conventional photograph of the European household, with sahib and memsahib seated at the centre and their Indian servants arranged around them with the uniforms or objects that signify their respective functions. 15
The iconography of the plague hospital thus resonates with the photographic conventions of colonial domesticity, suggesting, contra Ranajit Guha, that the British were ‘at home’ in empire (Guha, 2009), or that the orderliness and domestic harmony of the plague camp stood in implicit contrast to the chaos and confusion, the dirt and disease, of the ‘native town’. Perhaps, too, at a time when Poona was in almost open revolt against colonial anti-plague measures and the city’s plague commissioner had only recently been shot, such images offered reassurance (if only to the British themselves) that not all Indians were antagonistic to their rule and to the rationality of the colonial sanitary order. But this was also an optical articulation of an idealised colonial hierarchy: it is clear who (defined by race and occupation) is in charge, who is peripheral or subordinate. White women (15 nurses and one doctor) occupy the same central position and superior status as their male colleagues (two white doctors but also, this being the 1890s, a Eurasian doctor).
But there is more to be gleaned from this photograph. Seated on the ground at the front of the picture are a row of Indian women, the faces of some barely visible from the saris drawn over their heads, sitting barefoot or in sandals, and in many cases openly returning the camera’s scrutinising gaze. If it were not for the photographs and the way in which they are composed, we might have little sense from textual sources alone of these women’s presence or the significant role they occupied. They have no utensils or instruments to signify their function, nor are they named individually or by caste. 16 But, from other sources, we know that these unnamed women, 60 in number, made up more than half of the hospital establishment and four times the number of English nurses, and that they were Marathi-speaking ‘ward ayahs’ or ‘ward women’. They almost certainly came from one of the dalit castes of the region, probably Mahars. 17
Were they therefore mehtaranies? Nowhere were they officially designated ‘sweepers’ (Hunter, 1898, p. 1014). Indeed, the use of the term ‘ayah’ is, like the composition of the image itself, more suggestive of the European household and the Indian ‘nurse’ assigned to look after white infants. The ward ayahs appear in several of the snapshot photographs of the hospital as well; their presence was clearly no accident. They evidently command less status than the male ‘ward assistants’, who, with their watchchains and buttoned-up jackets, appear immediately behind the doctors in this photograph. The position of the ayahs was surely closer to that of the ‘ward boys’ who stand at the rear. Hunter (1898, p. 1012) observed that each ward was under the supervision of an ‘English nurse, who had two or more ward-women under her to keep the ward clean, wait upon the patients, and do all the rough work’. A more patronising account, published in the British Medical Journal, indicated that these ‘native women’ were present at the hospital from start, administering medicines, applying poultices and doing ‘the rough work’ (British Medical Journal, 1899). Despite their initial ignorance and lack of understanding of hygiene, in time ‘these ward women … showed admirable qualities. Although they often did stupid things, it was marvellous how much good work was got out of them’ (‘Personal Experiences’, 1899, p. 25).
Because we know so little about them, it is impossible to say how the women were recruited. Had they previously worked at Sassoon Hospital? Were they already ‘ayahs’ in European service? Were they the wives and daughters of the male Mahars at the plague hospital who dug graves and performed other essential tasks? Nor do we know what became of them after they stopped working in the plague wards. But perhaps the conspicuous presence, to which these photographs so visibly allude, of two sets of ‘polluting’ women—English nurses and dalit ayahs—from opposite ends of the colonial spectrum of race, caste and class but here brought into close proximity, further accounts for high-caste antipathy to the plague hospital.
Dr Hunter
Marion Hunter appears in several of the Poona plague hospital photographs and in both the Adams and Jones albums (Figure 2).
She generally looks anxious (not at home in empire after all, perhaps), even out of place. She seems less confident than many of the nurses and even the ayahs who assist her in the wards. In the group photographs, she sits somewhat awkwardly, as if in a limbo of race, class and gender, between the white nurses and the male doctors, between the dalit women at her feet and the male hospital assistants behind her. Parachuted, as it were, into Poona, she is perhaps doubly an outsider—a stranger to India and a solitary woman doctor in a male-dominated medical domain.
Who was Kate Marion Hunter? In her early 30s, Hunter had qualified as a Licentiate of the Society of Apothecaries before attending the London School of Medicine for Women, where she enrolled for a Diploma in Public Health—‘doctor’ was therefore a courtesy title but one Hunter used of herself. A star pupil, she was singled out in the school’s annual report as being ‘foremost’ among its 26 present or former students. Other graduates became practitioners in Britain or missionaries overseas, but she had been ‘chosen by the India Office to go to Bombay to assist in dealing with the plague outbreak’ (London School of Medicine, 1898, p. 16). However, one likely reasons why, despite her lack of practical experience, she was selected ‘as a special case’ was because she had an influential uncle. She was the niece of Sir William Hunter, one of the leading administrators of nineteenth-century British India (Skrine, 1901), a man of considerable clout at the India Office, and who, one might reasonably assume, was keen to recommend his niece’s name for consideration. Much was made in London and India of her family connection: one newspaper report of her arrival in Bombay at the end of October 1897 (along with other doctors and nurses) mentioned the fact of her being Sir William’s niece twice in a single column (ToI, 1 November 1897, p. 3). What Marion herself made of this emphasis on her privileged family status is unclear. It is possible that she found it an embarrassment; it could, as we will see, be used against her. Certainly, she made no mention of her family in her speeches and writings, and after she left Poona in March 1898 she never returned to India. Before her departure, she wrote of establishing a fund for the widows and orphans left by Poona’s plague, but there is no evidence that it materialised. 18 Her subsequent work back in London concerned the hygiene and health education of pre-school children (Times, 9 January 1909, p. 9).
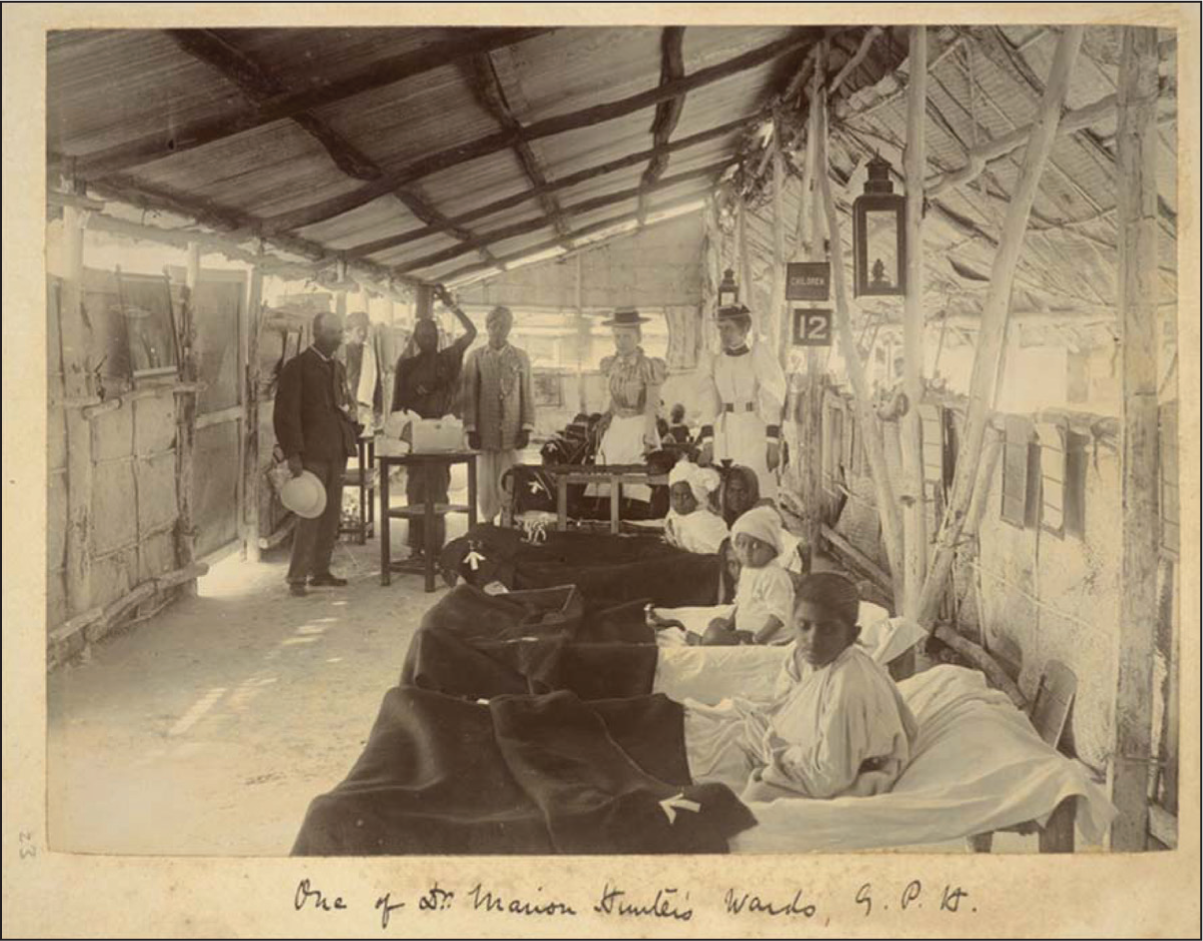
When Hunter reached Poona in November 1897, the city was experiencing a second deadly wave of plague; mortality was soaring (ToI, 25 December 1897, p. 5). The plague hospital was flooded with more than 400 cases, among them ‘Portuguese’ (Eurasians, for whom there was a separate ward), Indian Christians, low- and high-caste Hindus. Hunter was given charge of the children’s wards and some of the women’s, and it is in these that she appears in several photographs. By the time she left the following March, the epidemic had largely abated, and the number of patients had fallen significantly (Marsh, 1899); by then, too, the hospital seems to have been more positively regarded by leading citizens of Poona, including Gokhale (ToI, 2 April 1898, p. 5). So favourably was her work viewed by her superior, Dr Lloyd Jones, that it was proposed that a separate hospital should be established under her supervision for women and children alone. 19 This did not materialise but at the farewell party held in her honour in March 1898 her contribution was warmly praised. In an address one of the hospital assistants said she had taken ‘a keen interest’ in her work and ‘exerted herself to save the lives of the plague stricken’. Lloyd Jones described her as ‘an agreeable colleague’, ‘hardworking and conscientious’. She was, he said, ‘unremitting in her attention to her wards, and her ward ayahs reached a high state of efficiency’, a further indication of how closely doctors, nurses and ayahs worked together in the sanitary enclave. In response, Hunter thanked her colleagues, including the Indian hospital assistants ‘who were always willing to get up day and night to do what was wanted’. She further commended the ayahs, ‘who had been devoted in their care and attention’, only regretting that, knowing nothing of their language, she ‘could not thank them all as she would wish’. Her remarks were then translated into Marathi for the benefit of the hospital assistants—the ayahs were not present (ToI, 7 March 1898, p. 3).
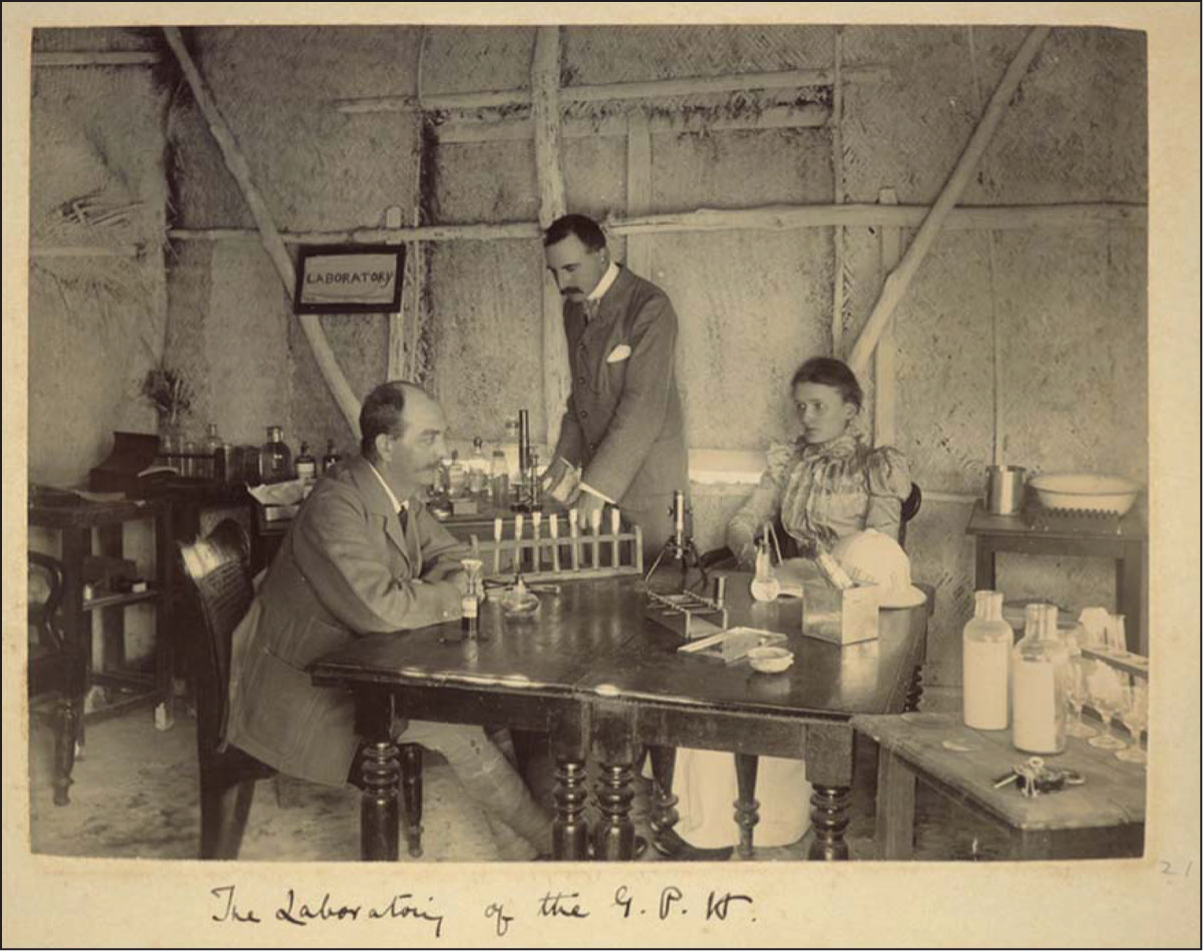
But not everything was as harmonious as the speeches might suggest. In her farewell speech, Hunter frankly admitted that in Poona ‘she found herself as a female medical officer rather awkwardly placed. It was difficult to get known. In the case of a male doctor he had his club and could soon make friends’ (ToI, 7 March 1898, p. 3). Further, not all her colleagues valued her presence. There is a photograph of Hunter in the hospital’s rudimentary bacteriological laboratory (Figure 3). She is elegantly dressed, her topi for once laid aside, and she looks less anxious than in some of the other photographs; she sits with two male colleagues, Drs Marsh and Lloyd Jones. The copy of this photograph in the Jones album (578/4: 21), in which Hunter looks directly at the camera, is simply labelled ‘The Laboratory of the G[eneral] P[lague] H[ospital]’. In a slightly different version of this image in the Adams album (photo 12), she looks towards Lloyd Jones, and, after referring to the two male doctors in the picture, Adams has written underneath, ‘Miss [sic] Hunter doesn’t seem to be doing much’. Below another photograph in his annotated album (photo 8), Adams notes: ‘This was my babies ward till Miss Marion Hunter L.S.A. (niece of Sir W. Hunter) came to the Hospital when I gave over charge to her much against my will’. In a further caption (photo 9), Adams remarks, ‘This is my children’s ward & Miss Marion Hunter L.S.A. & Dr Lloyd Jones are seen, together with a table on which are antiseptics ready for Miss Hunter to open up an abscess.’ It is clear Adams deeply resented that she had been put in charge of wards for which he had previously been responsible. He evidently felt that he, a real doctor rather than a licentiate, trained at Edinburgh University and Middlesex Hospital, and an IMS officer, was far better qualified than Hunter. He was, however, ordered to leave the Poona hospital (perhaps he was a difficult colleague) and transferred in January 1898 to a remote corner of Sind (ToI, 4 February 1898, p. 5). After Poona, it must have felt like a punishment posting.
Hunter’s empathy for India and Indians—if empathy there ever was—seemed to have evaporated once she left India. On returning to London, she gave several talks on ‘fighting the bubonic plague in India’. In one of these, held in a Bayswater drawing-room in March 1899 under the auspices of the Women’s Industrial Council, she was extravagantly introduced as the ‘health commissioner in charge of the women’s hospital’ in Poona. In her speech, Hunter observed that ‘like all Eastern cities’, Poona was ‘badly built, with little or no attempt at efficient drainage’. On the outbreak of plague, first in Bombay, then in Poona, the ‘panic-stricken’ ‘natives’ either ‘fled in terror’ or ‘resisted all the precautionary and remedial measures that were adopted’. By the time she left, Poona had been ‘overhauled and cleaned as it never had been before’, and in effecting this transformation, to her mind, European agency was clearly paramount (Times, 22 March 1899, p. 7). An extended version of her talk was published later that year in the Nineteenth Century. The article repeated and enlarged upon many of her most prejudicial remarks. One paragraph, for example, asserted that ‘in dealing with the natives’,
it has to be borne in mind that an Englishman [sic] meets with innumerable difficulties on account of: (1) caste prejudices; (2) superstition and fatalism; (3) native ignorance and distrust of all sanitation; (4) the dishonesty of many native officials, combined with a perfect genius for misrepresenting Government’s orders to suit their own ends; (5) the existence among natives of a freemasonry, which enables them to conceal sick or dead friends in a truly wonderful manner. That they themselves keep the epidemic alive by their conduct never seems to occur to them. (Hunter, 1898, p. 1009)
Such sentiments might almost have been penned by her uncle at his most censorious, or by one of the European civil and medical officers in Poona—Barry, perhaps, or Rand—so hostile was its description of the sanitary condition of the city, so flagrant its assertion of Indian fatalism, so insistent its claim to the indispensability of Europeans in rescuing Indians from their miserable plight. Even allowing for the linguistic conventions of the time, her resort to the phrase ‘an Englishman meets…’ seems to deny her own female experience and to replicate the assertive masculinity and racial cliches of colonial rule. However, when she turns to describing her own experiences, there is a partial shift of tone. She mentions that women doctors and nurses carried out checks on female rail passengers and in house-searches, signals that both nurses and ayahs played important roles in the plague camp, refers regretfully to the death of two of the English nurses, and observes that in Poona Hindu women ‘suffered most from the disease’, possibly because they were ‘more constantly indoors than men’ (Hunter, 1898, p. 1013). But nowhere in the article are we given a sense of her social isolation as a white woman doctor, the closeness of her engagement with the ayahs and other Indians, or the hostility she experienced from the resentful Dr Adams. Had all this been quickly forgotten, or did it appear of lesser consequence once back in the imperial metropolis?
Conclusion
Dr Hunter spent barely four months (November 1897 to March 1898) at the Poona plague hospital. Her experiences of the epidemic and of the prophylactic and remedial measures taken against the disease were even more limited than those of Alice Corthorn who stayed in India substantially longer (four years). During Hunter’s time in Poona, thousands died of plague but even this was only a fraction of the millions who eventually perished from the disease. In that sense to refer to ‘Dr Hunter’s plague’ in the title of this article is an absurdity. But I have done so for a purpose. As we can see from her Bayswater talk and Nineteenth Century article, she was taken, despite her limited experience, as having an authoritative voice, a position on India, empire, disease and medicine that warranted attention and commanded respect. I have no evidence that the photographs of the plague camp circulated widely in Poona or had any impact on Indian opinion there. But when reports of her talks appeared in the press or in medical journals, when a photograph of the hospital staff appeared in a London illustrated paper, with her seated at the centre, she became—to the imperial metropole—the female face of the heroic fight against India’s bubonic plague. 20 Sometimes the grand ideologies of empire were built on such slender foundations and on such selective acts of appropriation.
That aside, Hunter’s brief incursion into health and disease in India generated historical evidence that crosses the conventional divide between visual and textual material. She did not take photographs herself, but, as the subject of a number of them, her presence there (and the comments made by Dr Adams) help to give meaning and context to the Poona plague hospital and to the situation and experience of medical women in British India; read alongside textual sources, they testify to the intimacies and antipathies of race and gender in the colonial sanitary enclave. Certainly, there is no uniformity here, no complete congruity between the discursive and visual evidence. Rather different conclusions can be drawn from her farewell speech, from her published article, from newspaper reports and the official archive. There are many tensions, incongruities and enigmas in Dr Hunter’s plague. But, at the same time, the ensemble effect, the coming together, in photographs as in lived reality, of dalit ayahs, a white woman doctor and English nurses makes for a striking demonstration, not just of the merits of a conjoined use of visual and textual material, but also of the overlapping complexities of race and gender.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.