
Abstract
Though many studies have linked shared decision-making with positive patient outcomes and patient satisfaction, there is less research on the practicality and feasibility of such an approach, specifically, in India. Recent findings indicate that contextual constraints of the patients and family caregivers are fused with and inevitably shape their decision-making style. This study investigates the influence of individual (paternalistic and shared decision-making style) and contextual (financial status of the patients) factors on certain cultural aspects of decision process, namely, trust in doctors, patient’s agency, emotional distress and attribution of responsibility. Data were collected using a survey questionnaire from a sample of 306 participants. Linear mixed models were used to analyse the responses. The results indicate that a shift towards shared approaches does yield qualitatively superior outcomes in terms of increased trust in doctors and patients’ agency along with reduced emotional distress. The study also emphasises the role of cultural metaphysical beliefs in attributing responsibility for treatment decisions. Further, low financial status was found to be associated with higher trust in doctors, lower patient agency, and increased emotional distress for both patients and family caregivers. The move towards shared decision-making, considering the contextual realities of patients, could be instrumental in addressing critical issues, such as prevalence of collusion, superficial role of informed consent, and high reliance on doctors’ authority or expertise.
Introduction
With advances in technologies, both doctors and patients have huge amounts of information at hand. This information makes the decision process more complex (Lantos, 2021). In the literature on doctor–patient relationship and interaction, there is a move towards evidence-based, informed, and shared decisions (Gillman & Ferrer, 2021; Sankar et al., 2018). Though there are many studies that have linked such decisions with positive patient outcomes and patient satisfaction (Entwistle et al., 2012; Gillman & Ferrer, 2021; Sankar et al., 2018), there is less research on the practicality and feasibility of such an approach (Ozdemir & Finkelstein, 2018), specifically, in India (Gopichandran, 2019; Sankar et al., 2018). There are certain unique aspects that define doctor–patient relationship in India, such as reverence towards authority (Panda, 2023; Subramani, 2019), paternalistic family dynamics (where often the decision-maker is the head of the family) (Gopichandran, 2019; Subramani, 2019), lower agency of female patients than their male counterparts (Bhakuni, 2020; Gopichandran, 2019), power distance between doctors and patients (Jacob, 2014), substantially low levels of cancer awareness among public (Chandra et al., 1998), among others. Research exploring how doctors and patients communicate to reach shared and informed decisions during the treatment process given such conditions is conspicuously deficient (Bhakuni, 2020; Gopichandran, 2019; Panda, 2023; Sankar et al., 2018). The doctor–patient communication is also not immune to the sociocultural influences, such as beliefs of the patients and the family caregivers regarding full disclosure of information, attribution of decision responsibility to metaphysical factors, and the extent of trust in the medical fraternity (Chaturvedi et al., 2009; Chittem et al., 2021; Mathew et al., 2021; Victor et al., 2018).
Studies suggest that in India, the patients and their families often put the burden of the medical decision solely on the doctors’ expertise and remain a passive audience to the decision-making process (Jacob, 2014; Sareen & Dutt, 2019). Various factors such as high financial burden of cancer, low education and knowledge about the disease, and low financial status that renders the possibility of taking second opinions impossible, were associated with the high prevalence of paternalistic decision-making (Harding et al., 2022; Mathew et al., 2020). Conversely, patients with higher socioeconomic status and greater literacy levels were more actively involved in the decision process (Datta et al., 2017; Harding et al., 2022). Such findings indicate that contextual constraints of the patients and family caregivers are fused with and inevitably shape their decision-making style (Blok et al., 2023; Datta et al., 2017; Ram Prakash & Lingam, 2021; Zafar & Peppercorn, 2023).
The present study focuses on four crucial aspects of the decision process: trust on doctors, patients’ agency, emotional distress and attribution of responsibility. The study examines how individual (paternalistic and shared decision-making style) and contextual (financial status of the patients) factors influence certain aspects of decision process, namely, trust in doctors, patient’s agency, emotional distress and attribution of responsibility? The aim was not to assess the participants’ actual decisions or evaluate the accuracy/optimality/efficiency of the decision outcome or analyse the strategies/heuristics used to make the decision (Klein, 2017; Weiss & Shanteau, 2021), rather, through hypothetical vignettes simulate the experience of making decisions during cancer treatment, considering factors, such as socioeconomic status and decision-making style.
The Contradiction of Shared Decision-making
In the last decade, shared decision-making has emerged as the preferred approach for healthcare professionals, patients and policy makers, while paternalistic approach is increasingly perceived as outdated and potentially detrimental for patient care (Driever et al., 2021; Lantos, 2021; Thompson & Whiffen, 2018). In the shared decision-making approach, medical decisions are considered a collaborative outcome involving both patients and doctors and are therefore believed to be more aligned with the contextual realities and values of patients (Lantos, 2021; Pollard et al., 2015). However, recent studies have challenged the feasibility and effectiveness of shared decision-making (Driever et al., 2020, 2021; Hahlweg et al., 2017; Oprea et al., 2023).
In a cross-sectional survey of 785 doctors, Driever et al. (2020) found that though most doctors preferred shared decision-making, in their everyday practice they often leaned towards paternalistic decision-making (Oprea et al., 2023). Physicians level of support for shared decision-making was found to be associated with various factors such as uncertainty in evidence (Driever et al., 2021; Pollard et al., 2015), time pressure (Hahlweg et al., 2017), severity of treatment decisions (Pollard et al., 2015), patient characteristics, such that more active patients facilitated shared decision-making (Hahlweg et al., 2017; Pollard et al., 2015). In a subsequent study by Driever et al. (2021), it was found that medical residents often confused shared decision-making with obtaining informed consent and/or letting patients decide when faced with inconclusive evidence.
Research examining patients’ preferences for medical information and their desired role in decision-making has yielded inconsistent findings (Elkin et al., 2007; Josfeld et al., 2021; Sankar et al., 2018; Thompson & Whiffen, 2018). Josfeld et al. (2021) surveyed 220 cancer patients and found that participants desired more information than they received, often feeling overwhelmed with information or underinformed, particularly during consultations with doctors. The majority expressed a preference for shared decision-making over deciding alone, with none indicating a preference for doctors making decisions on their behalf (Josfeld et al., 2021). In contrast, Sankar et al. (2018) found that while most participants expressed a strong desire to know their diagnosis and prognosis, 97% (of the 133 cancer patients surveyed in India) wanted their doctors to make decisions regarding treatment. Another study involving 73 elderly cancer patients found that only 44% wanted survival-related information, with approximately half preferring a passive role in decision-making (Elkin et al., 2007). Recently, some researchers have challenged the Western emphasis on patient autonomy, suggesting that paternalism may hold value in other cultural contexts for delivering high-quality ethical care (Heidenreich et al., 2017; Papathanassoglou et al., 2012; Thompson & Whiffen, 2018).
With such mixed evidence regarding prevalence and feasibility of the shared decision-making approach, this study takes a step back to investigate whether the two decision-making styles indeed differ in their association with core aspects of the decision process. Further, the study incorporates the contextual dimension of patients’ financial status to further enrich the understanding of decision-making styles.
Core Aspects of Decision Process
The present study identified four core aspects of the decision process: trust in doctors, patient’s agency, emotional distress and attribution of responsibility. Previous literature suggests that as shared decision-making acknowledges patients’ autonomy (Guadalajara et al., 2022; Lantos, 2021), it fosters greater trust in doctors for both patients and caregivers (Entwistle, 2004; Lincoln et al., 2023) and elicits higher patient satisfaction (Oprea et al., 2023; Pollard et al., 2015). Financial toxicity is also found to be linked to higher emotional distress (Abrams et al., 2021; Carrera et al., 2018), lower agency in decision process (Boby et al., 2021; Prinja et al., 2023) and higher trust in doctors (Abrams et al., 2021; Boby et al., 2021; Zafar & Peppercorn, 2023). Studies examining cultural beliefs in the face of illness also suggest that patients often attribute the cause of their illness to metaphysical factors, such as god, fate or karma (Agrawal & Dalal, 1993; Dalal & Misra, 2006; Kohli & Dalal, 2016).
The following hypothesis was tested:
H1: Trust on doctors would be higher for conditions of the shared decision-making as compared to those of paternalistic decision-making.
H2: Patient’s agency would be higher for conditions of the shared decision-making as compared to those of paternalistic decision-making.
H3: Emotional distress for patients and family caregivers would be lower for conditions of the shared decision-making as compared to those of paternalistic decision-making.
H4: Attribution of responsibility to doctors, god and chance/luck would be lower and to patients and family caregivers would be higher for conditions of the shared decision-making as compared to those of paternalistic decision-making.
H5: Trust on doctors would be higher for conditions of low financial status as compared to high financial status.
H6: Patient’s agency would be lower for conditions of low financial status as compared to high financial status.
H7: Emotional distress for patients and family caregivers would be higher for conditions of low financial status as compared to high financial status.
H8: Attribution of responsibility to doctors, god and chance/luck would be higher and to patients and family caregivers would be lower for conditions of low financial status as compared to high financial status.
H9: There would be a significant interaction effect between decision-making style (shared versus paternalistic) and financial status (low versus high) on trust in doctors, patient’s agency, emotional distress and attribution of responsibility (doctors, patients, family caregivers, god and chance/luck).
Method
Study Design
A 2 (decision-making style: paternalistic, shared) × 2 (financial status: high, low) within-subject factorial design was used to examine the effect of the two independent variables on four dependent variables: trust on doctors, patient’s agency, emotional distress in patient and family caregivers, and attribution of responsibility. Hypothetical vignettes were constructed on the basis of the four conditions:
High financial status and paternalistic decision-making Low financial status and paternalistic decision-making High financial status and shared decision-making Low financial status and shared decision-making
The participants responded to all four vignettes and, therefore, a within-subject random error was introduced. Linear mixed models (LMMs) were used for analysis as the data had both fixed effects (decision-making style and financial status) and random effects (variation due to subjects). The design was fully crossed and balanced, subject × condition, such that all subjects were part of all four conditions. LMMs are often considered a more robust technique (as compared to repeated measures ANOVA) in accounting for such error variation (Walker et al., 2019).
Sample
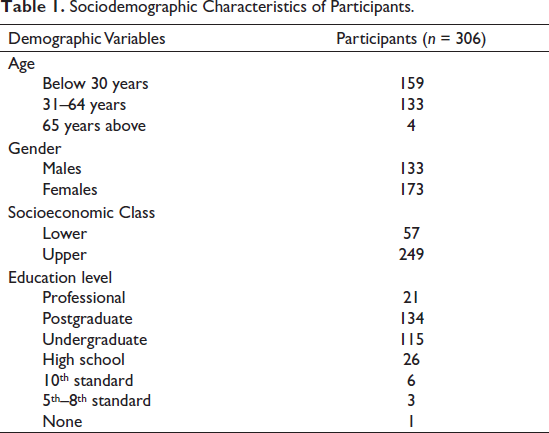
The sample consisted of 306 participants residing in various parts of India, mainly from, Delhi, NCR (National Capital Region), Uttarakhand and Haryana. The mean age of participants was 34.02 years with a range of 17–72 years. The demographic details are depicted in Table 1. Data were collected using a Google form that was circulated to the participants using a combination of convenience and snowball sampling.
Sociodemographic Characteristics of Participants.
Inclusion/Exclusion Criteria
Participants who had been diagnosed with cancer or had acted as a primary caregiver for a cancer patient were purposely excluded from the sample. It was because their previous experience of taking decisions under such conditions would have acted as a major confounding variable. Forty-eight such participants were identified and were excluded from the analysis, leaving a sample of 258 participants.
Measures
A survey questionnaire was constructed that consisted of a brief detail about the study with informed consent, followed by a section on demographic information and four hypothetical vignettes, each followed by the measures for dependent variables.
Demographic Information
The survey included a section seeking demographic information from participants regarding, age, gender, level of education, their perceived socioeconomic status, area of residence, and inclusion/exclusion criteria.
Hypothetical Vignettes
Four hypothetical vignettes were constructed based on the unique combinations of the independent variable. The vignettes were drafted meticulously to isolate the effects of the independent variables while maintaining rigorous control over extraneous factors. Gender-neutral language was consistently employed, and potential confounding factors such as age, place of residence and religious inclinations were deliberately excluded from the vignettes. Throughout, language was intentionally kept clear and free of technical jargon. The vignettes were constructed to reflect real-world variations.
To manipulate financial status, two scenarios were developed. In the high financial status conditions, the character ‘X’ was portrayed as employed in a big corporate company with more than sufficient savings. Conversely, in the low financial status conditions, ‘X’ assumed the role of a manual labourer, with their family’s savings being meagre. Importantly, all vignettes explicitly conveyed that ‘X’ lacked medical insurance, eliminating potential confounding effects.
To manipulate decision-making style, the different aspects of paternalistic and shared decision-making were included to capture their meaning. In the paternalistic decision-making conditions, ‘X’ and their family members pushed the physician to make treatment decisions, emphasising their trust in the doctor’s expertise. In contrast, the shared decision-making conditions depicted ‘X’, their family members and the doctor engaging in collaborative discussions to jointly determine treatment options.
Dependent Variable Measures
The measures for dependent variable were based on the findings of Study 1 and 2 of the thesis as well as previous literature.
Trust in doctors: This was assessed by developing a comprehensive measure consisting of six distinct dimensions. The first dimension, competence, evaluated the extent to which participants trusted the expertise and competence of the doctors (Hall, 2006). The second dimension gauged the level of respect for doctors’ authority (Gopichandran, 2019). The third dimension, fidelity, delved into the honesty of communication with patients and the respect for their agency (Gopichandran, 2019; Hall, 2006). Loyalty, the fourth dimension, focused on the loyalty exhibited towards doctors who had provided past treatment (Gopichandran, 2019). The fifth dimension, experience level, considered the seniority and experience of the doctors. Finally, the sixth dimension, global trust, captured a holistic sense of trust encompassing all dimensions (Hall, 2006). The measure thus included six items measured on a 5-point Likert scale, ranging from 1 (no trust) to 5 (complete trust). The total score for trust in doctors was computed by summing the scores for each of the six items.
Patients’ agency: This included a single item measured on a 5-point Likert scale, ranging from 1 (no agency) to 5 (complete agency): In the given scenario, how much do you think the patient has a voice or say in deciding the best treatment option?
Emotional distress: The perceived experience of emotional distress for both patient and family caregivers in the vignettes was operationalised in terms of five emotions: mental distress, helplessness, fear, anxiety and anger. The five items were measured on a 5-point Likert scale and the total score for emotional distress for both patient and family caregivers was calculated by summing the individual scores of all five items.
Attribution of responsibility: This variable was operationalised in terms of blame or accountability that would be placed on doctors, patients, family caregivers, god and chance or luck, in case the chosen treatment option in the vignette severely hampered the patients’ quality of life and was unable to eliminate cancer. The participants rated the amount of responsibility to each of the five factors on a 5-point Likert scale ranging from 1 (no responsibility) to 5 (complete responsibility).
Procedure
The survey questionnaire was translated into Hindi language and then back translated to English by an expert. A pilot study was conducted to ensure the clarity and coherence of the questionnaire on a sample of 14 participants. The age range of the participants was 26–60 years. In the pilot study, the participants demonstrated a satisfactory understanding of the questionnaire items; however, some participants expressed a need for enhanced clarity regarding the hypothetical vignettes. On the basis of this feedback, a color-coding system was implemented to accentuate the distinctions between the four vignettes. This visual enhancement aimed to facilitate participants’ comprehension and engagement with the scenarios, ensuring that the nuances of the experimental conditions were readily discernible. These Google forms were then circulated online to collect data.
Analysis
The statistical analysis was conducted using R program, version 4.2.3 (RStudio Team, 2022). LMMs were used to analyse responses to the four vignettes. There were two fixed effects (decision-making style and financial status) and one random effect (within-subject factor). The analysis aimed to calculate the main effects and interaction effect of the fixed effects on the four dependent variables while controlling for the random effect. Conducting LMM analysis included:
Understanding the model structure: The model was created as follows:
Model 1: Trust in doctors ~ Decision-making × Financial status + (1 + Decision-making + Financial status|Subject)
Decision-making style (DM) at two levels: paternalistic (P) and shared (S) Financial status (FS) at two levels: high (H) and low (L) Four conditions:
HP: High FS and paternalistic DM LP: Low FS and paternalistic DM HS: High FS and shared DM LS: Low FS and shared DM
Sum-to-zero Contrast for Linear Mixed Modelling.

Model 2: Trust in doctors ~ Decision-making × Financial status + (1|Subject)
To check goodness-of-fit, Akaike information criterion (AIC) was used to select the model. The lower the AIC, the better the model fit (Singmann & Kellen, 2019; Walker et al., 2019). Therefore, Model 1 with slightly lower AIC = 2,451 as compared to Model 2 with AIC = 2,474, was chosen.
These steps were followed for all response variables. In total, nine LMMs [trust in doctors (1), patient’s agency (1), emotional distress for patients (1), emotional distress for family caregivers (1) and five factors of attribution of responsibility (5)] were created and interpreted.
Results
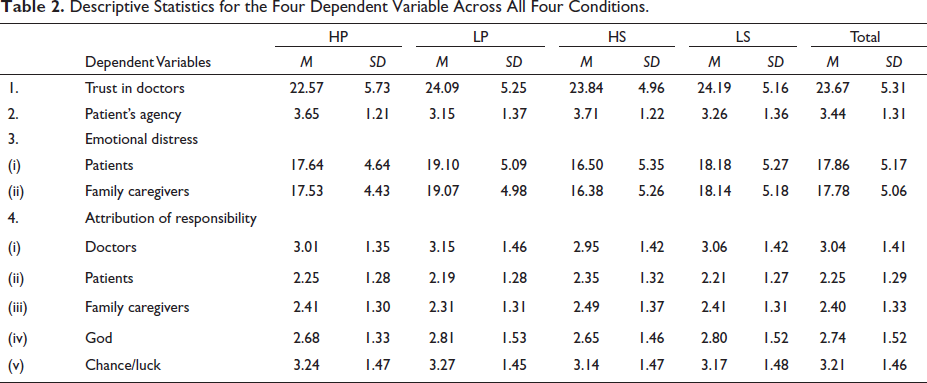
Tables 3 and 4 summarise the results of the LMMs for all four dependent variables.
Descriptive Statistics for the Four Dependent Variable Across All Four Conditions.
Summary of Linear Mixed Model for Trust in Doctors, Patient’s Agency and Emotional Distress.
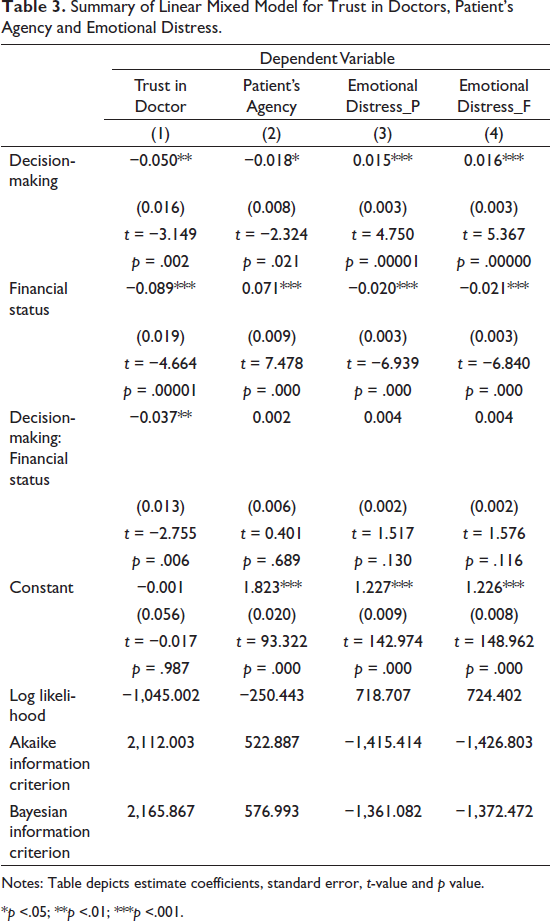
Notes: Table depicts estimate coefficients, standard error, t-value and p value.
*p <.05; **p <.01; ***p <.001.
Summary of Linear Mixed Model for Attribution of Responsibility.
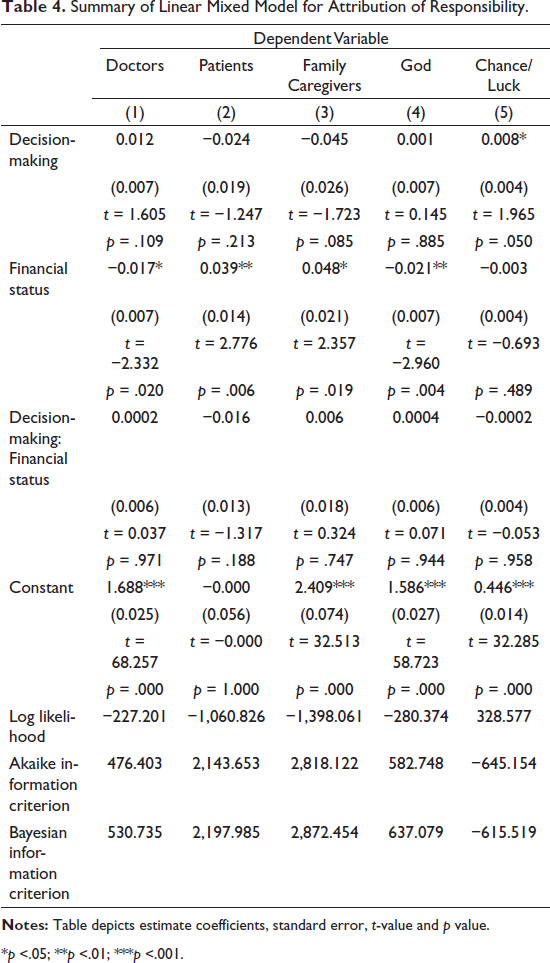
*p <.05; **p <.01; ***p <.001.
Trust in Doctors
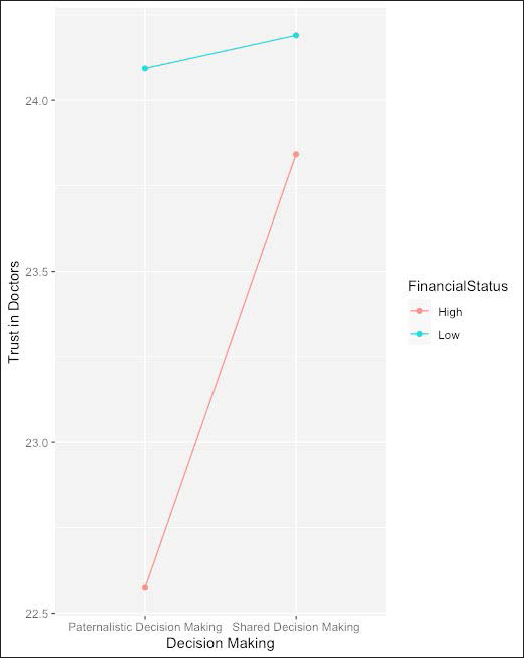
High significant main effects were found for both decision-making style (βˆ = −0.050, p = .002) and financial status (βˆ = −0.089, p = .00001) on scores of trust in doctors. The negative coefficient for decision-making style suggests that with a shift from paternalistic to a shared decision-making style, the trust in doctor tends to increase. Similarly, the negative coefficient for financial status indicates that with the decrease in financial status, that is, from high to low, trust in doctors tends to increase. A significant interaction effect for decision-making style and financial status was also found (βˆ = −0.037, p = .006). This means that the impact of both decision-making and financial status is modified by the presence of the other variable.
Further, post-hoc analysis suggests that the scores for trust in doctors in HP condition are significantly different from HS condition (t-value = −4.169, p = .0002), LS condition (t-value= −5.386, p <.00001) and LP condition (t-value = −5.583, p <.00001). This can be more clearly seen in Figure 1 which depicts the mean scores of trust in doctors when grouped by decision-making and financial status. The graph shows that overall trust in doctors is lowest for HP condition. The conditions for low financial status elicited higher trust in doctors’ scores as compared to conditions with high financial status. Similarly, conditions with shared decision-making elicited higher trust in doctors scores as compared to paternalistic decision-making conditions. The pseudo-R2 for the entire model was 0.825, and for fixed effects was 0.0115. It means that though the model is quite robust as it accounts for 82.5% of variation in scores for trust in doctors, only 1.15% of this variance is attributed to fixed effects.
Mean Scores of Trust in Doctors: Grouped by Decision-making and Financial Status.
Patient’s Agency
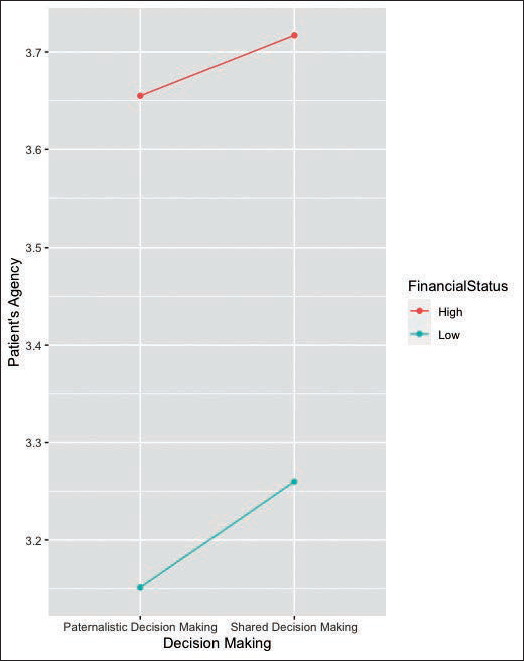
High significant main effects were found for both decision-making style (βˆ = −0.018, p = .021) and financial status (βˆ = 0.071, p = .000) for scores on perceived patient’s agency. The negative coefficient for decision-making style suggests that with a shift from paternalistic to a shared decision-making style, the patient’s agency tends to increase. The positive coefficient for financial status indicates that with the decrease in financial status, that is, from high to low, perceived patient’s agency also tends to decrease. No significant interaction effect for decision-making style and financial status was found (βˆ = 0.002, p = .689).
Further, post-hoc analysis suggests that the scores for patient’s agency were significantly different in four groups. Specifically, differences between: HP condition and LP condition (t-value= 6.482, p <.0001), HP condition and LS condition (t-value= 4.489, p = .0001), HS condition and LP condition (t-value= 6.975, p <.0001) and HS condition and LS condition (t-value= 6.059, p <.0001). Figure 2 depicts the mean scores of perceived patient’s agency when grouped by decision-making and financial status. The graph shows that patient’s agency was perceived to be much higher in conditions of high financial status as compared to low financial status. Further, patient’s agency was perceived to be lower for paternalistic decision conditions as compared to shared decision conditions. The pseudo-R2 for the entire model was 0.749, and for fixed effects was 0.0356. It means that though the model is quite robust as it accounts for 74.9% of variation in scores for patient’s agency, only 3.56% of this variance is attributed to fixed effects.
Mean Scores of Patient’s Agency: Grouped by Decision-making and Financial Status.
Emotional Distress
Patients
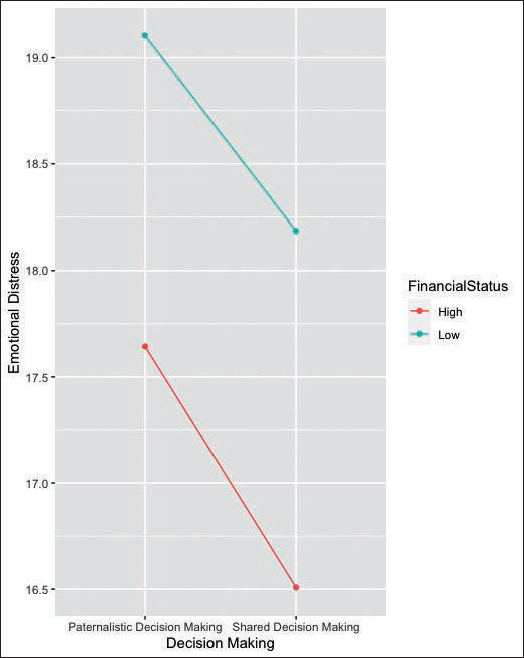
High significant main effects were found for both decision-making style (βˆ = 0.015, p = .00001) and financial status (βˆ = −0.020, p = .000) for scores of perceived emotional distress for patients. The main effect for decision-making style suggests that emotional distress for patients is higher in paternalistic decision condition as compared to shared decision condition. The negative coefficient for financial status suggests that with the decrease in financial status, that is, from high to low, perceived emotional distress for patients tends to increase. No significant interaction effect for decision-making style and financial status was found (βˆ = 0.004, p = .130).
Post-hoc analysis suggests that apart from the difference between HP condition and LS condition, all other groups had significant differences. Specifically, significant differences were found between HP and HS condition (t-value= 4.744, p <.0001), HP and LP condition (t-value= −4.461, p = .0001), HS and LP condition (t-value= −8.067, p <.0001), HS and LS condition (t-value= −6.360, p <.0001) and LP and LS condition (t-value= 2.975, p = .0162). Figure 3 depicts the mean scores of perceived emotional distress for patients when grouped by decision-making and financial status. The graph shows that emotional distress for patients was perceived to be much higher in conditions of low financial status as compared to high financial status. Similarly, emotional distress for patients was perceived to be higher for paternalistic decision conditions as compared to shared decision conditions. The pseudo-R2 for the entire model was 0.784, and for fixed effects was 0.0253. It means that though the model is quite robust as it accounts for 78.4% of variation in scores for emotional distress for patients, only 2.53% of this variance is attributed to fixed effects.
Mean Scores of Emotional Distress for Patients: Grouped by Decision-making and Financial Status.
Family Caregivers
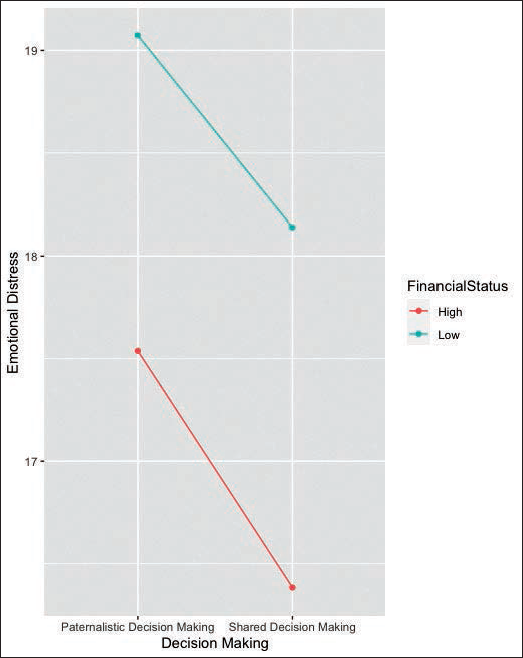
High significant main effects were found for both decision-making style (βˆ = 0.016, p = .0000) and financial status (βˆ = −0.021, p = .000) for scores of perceived emotional distress for family caregivers. The main effect for decision-making style suggests that emotional distress for family caregivers is higher in paternalistic decision condition as compared to shared decision condition. The negative coefficient for the main effect of financial status suggests that with the decrease in financial status, that is, from high to low, perceived emotional distress for family caregivers tends to increase. No significant interaction effect for decision-making style and financial status was found (βˆ = 0.004, p = .116).
Post-hoc analysis suggests that apart from the difference between HP condition and LS condition, all other groups had significant differences. Specifically, significant differences were found between HP and HS condition (t-value=5.140, p <.0001), HP and LP condition (t-value= −4.309, p = .0001), HS and LP condition (t-value= −8.244, p <.0001), HS and LS condition (t-value= −6.299, p <.0001) and LP and LS condition (t-value= 3.132, p = .0099). Figure 4 depicts the mean scores of perceived emotional distress for family caregivers when grouped by decision-making and financial status. The graph shows that emotional distress for family caregivers was perceived to be much higher in conditions of low financial status as compared to high financial status. Similarly, emotional distress for family caregivers was perceived to be higher for paternalistic decision conditions as compared to shared decision conditions. The pseudo-R2 for the entire model was 0.739, and for fixed effects was 0.0291. It means that though the model is quite robust as it accounts for 73.9% of variation in scores for emotional distress for family caregivers, only 2.91% of this variance is attributed to the fixed effects.
Mean Scores of Emotional Distress for Family Caregiver: Grouped by Decision-making and Financial Status.
Attribution of Responsibility
Table 4 depicts the results for LMMs for the five factors of attribution of responsibility for taking the decision in case the treatment hampered the patient’s life or is unable to eliminate cancer. For all the factors, except for the factor of chance or luck, a significant main effect for financial status was found (see Table 4). For the factors of doctor and god, the negative estimates reflect that as the financial status decreases from high to low, the attribution of responsibility to these factors increases. Conversely, for the factors of Patients and Family caregivers, as the financial status decreased from high to low, the attribution of responsibility to these factors also decreased. Apart from the factor of Chance, no significant main effect was found for decision-making (βˆ = 0.008, p = .050). This suggests that attribution of responsibility for only the factor of chance was higher in conditions of paternalistic decision as compared to shared decision. For all the other factors, there were no significant differences in attribution of responsibility due to decision-making conditions. No significant interaction effects were found for all five factors (see Table 4).
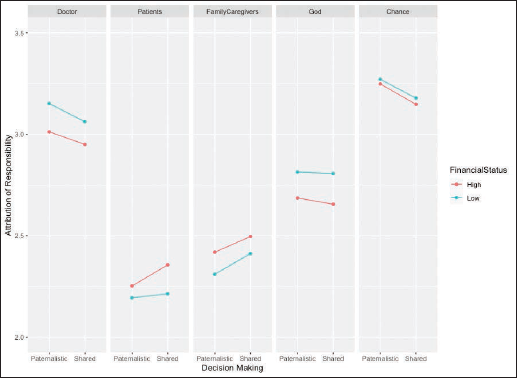
Post-hoc analysis suggests significant differences only between the HS and LP condition for attribution of responsibility to doctors (t-value= −2.589, p = .0496), patients (t-value= 2.604, p = .0477) and family caregivers (t-value= 2.976, p = .0168). No post-hoc differences were found for the factors of god and chance. Surprisingly, the pseudo-R2 for the fixed effects for all five factors were exceptionally low: doctors (0.22%), patients (0.24%), family caregivers (0.24%), god (0.23%) and chance (0.11%). This suggests that though the main effects are significant, they barely account for the variation in the scores of attribution to responsibility. However, Figure 5 helps in understanding the results of the attribution of responsibility scores across all five factors. It depicts that the highest attribution of responsibility is given to Chance, followed by doctors and god, whereas the lowest attribution of responsibility is given to patients. In condition of high financial status, patients and family caregivers are attributed more responsibility as compared to low financial status condition.
Mean Scores of Attribution of Responsibility: Grouped by Decision-making and Financial Status.
Discussion
The study aimed to explore the influence of individual (paternalistic and shared decision-making style) and contextual (financial status of the patients) factors on certain aspects of decision process, namely, trust in doctors, patient’s agency, emotional distress, and attribution of responsibility.
Influence of Paternalistic Versus Shared Decision-making on Decision Process
The findings support H1, H2 and H3, indicating that shared decision-making correlates with higher trust on doctors, higher patients’ agency and lower emotional distress for both patients and family caregivers when compared to paternalistic decision-making. Contrarily, the study does not support H4. While a lower attribution of responsibility to chance/luck was found for shared decision-making compared to paternalistic decision-making, no such significant differences were found for other factors, namely, doctors, God, patients and family caregivers.
Previous research on shared decision-making yields conflicting evidence regarding its potential benefits, with some studies suggesting positive associations with patient satisfaction and health outcomes (Bomhof-Roordink et al., 2019; Entwistle, 2004; Entwistle et al., 2012; Josfeld et al., 2021), while others express scepticism about its practical application (Gillman & Ferrer, 2021; Guadalajara et al., 2022; Ozdemir & Finkelstein, 2018). In this study, experimental conditions of shared decision-making were found to be linked to heightened trust, reduced emotional distress, and increased patient agency. A recent mixed-method study involving 369 surrogate family decision-makers identified five shared decision-making behaviours—‘discussing surrogate’s role, explaining medical condition and prognosis, providing emotional support, assessing understanding, and eliciting patient’s values and preferences’ (Lincoln et al., 2023, p. 1214). Each of these elements was associated with a 0.37-point increase in trust in the treating physician (Lincoln et al., 2023).
Regardless of contextual factors, the findings indicate that patient’s agency was consistently low for conditions of paternalistic decision-making, wherein doctors solely bear decision responsibilities (Davies & Parker, 2022). In a study, Blok et al. (2023) interviewed 40 family caregivers of patients undergoing life-assistive treatment. They found that ‘anxious family caregivers’ expressed distress due to ‘lack of information about health care system processes’ (Blok et al., 2023, p. 25). Similarly, those in borderline anxiety group reported that ‘not understanding the reasons for the medical team’s care decisions contributed to their distress’ (Blok et al., 2023, p. 26). Such studies suggest that since shared decision-making promotes open communication (Guadalajara et al., 2022), there is an increased patients’ and family caregivers’ participation in the treatment process (Lincoln et al., 2023) and lower treatment anxiety (Blok et al., 2023).
Surprisingly, there were no significant differences between the two decision-making styles in the attribution of responsibility for treatment decisions, except in case of chance/luck. Though paternalistic decision-making is associated with increased responsibility on the part of doctors compared to patients or family caregivers (Davies & Parker, 2022), in this study no such distinctions were found. Further, previous literature suggests the tendency of patients and family caregivers to relegate to metaphysical beliefs, for instance, beliefs in god, karma or chance/luck to explain the occurrence of illness (Kohli & Dalal, 2016). The current findings also indicate that specifically in paternalistic decision-making conditions, the attribution of decision responsibility was higher for the factor of chance/luck. This could so as the patients feel less in control of the treatment process; they tend to tilt more towards external locus of control for the treatment decisions (Kohli & Dalal, 2016; White et al., 2021).
Role of Low Versus High Financial Status in Decision-making
Financial toxicity remains a nascent area of investigation within the literature, with most studies primarily focusing on its prevalence (Abrams et al., 2021; Boby et al., 2021; Prinja et al., 2023), identifying high-risk groups (Boby et al., 2021; Lentz et al., 2019; Prinja et al., 2023), and establishing its connections with quality of life, well-being and physical health (Abrams et al., 2021; Carrera et al., 2018; Zafar & Peppercorn, 2023). However, its impact on decision-making in cancer treatment remains an understudied area. This study contributes to the evolving body of literature by elucidating the associations between financial status and crucial aspects of the decision-making process.
The findings of the study support H5, H6 and H7, indicating that conditions of low financial status elicited higher trust in doctors, lower patient’s agency and high emotional distress for both patients and family caregivers as compared to high financial status conditions. Previous studies link low financial status with lower awareness of cancer and treatment therapies and lower access to informational resources (Sahu et al., 2020; Singh et al., 2016). Moreover, studies on paternalistic decision-making have linked lower financial status with higher trust on doctors (Driever et al., 2021; Jacob, 2014; Ram Prakash & Lingam, 2021). Research indicates that patients from low financial status are often not able to complete treatment, lose their daily wages, go under tremendous financial debt, are not able to take second opinions and thus have lesser options as compared to patients with financial security (Abrams et al., 2021; Boby et al., 2021; Zafar & Peppercorn, 2023). In a qualitative study exploring gender barriers in utilisation of government insurance schemes, Ram Prakash and Lingam (2021) found that female patients’ financial dependence and lack of control over resources severely affected their health-related decision-making. They were mostly dependent on male members of the family for financing even outpatient consultations. Further, for male patients belonging to ‘very poor families’, treatment decisions such as hospitalisation and surgery were often delayed due to concerns about the potential loss of daily wages during both surgical and aftercare period (Ram Prakash & Lingam, 2021). Such studies indicate how crucial treatment-related decisions are inherently linked to the financial status of the patients. However, there are barely any studies that empirically illuminate the impact of the financial status of patients on the decision process in cancer treatment.
Further, H8 was partially supported. The findings indicate that attribution of decision responsibility in low financial status conditions was found to be higher for doctors and god, and conversely, lower for patients and family caregivers, as compared to the high financial status group. However, there was no significant difference between the two groups for the factor of chance or luck. Factors such as low knowledge and awareness among patients belonging to low financial status (Sahu et al., 2020; Singh et al., 2016), reduced agency in choosing healthcare facilities (Ram Prakash & Lingam, 2021) and a high reliance on doctors’ authority (Bhakuni, 2020; Subramani, 2019) could probably explain such an external locus of control—wherein god and doctors are attributed higher decision responsibility than patients and family caregivers.
Interaction of Individual and Contextual Variables
The study did not find enough evidence to support H9, such that, the interaction of decision-making style and financial status was found to be significant only for trust in doctors. For all other variables, patient’s agency emotional distress for patients and family caregivers, attribution of responsibility (doctors, patients, family caregivers, god and chance/luck), no significant interaction effect was found. Interestingly, the findings indicate that trust in doctors was lowest for the interaction of high financial status and paternalistic decision style, as compared to all other groups. In a study involving 606 patients, Kraetschmer et al. (2004) found that patients who preferred an autonomous role in decision-making exhibited relatively low levels of trust in physicians. Alternatively, those who preferred a shared role had moderate levels of trust, while those who preferred a passive role were more likely to have blind trust.
Bhakuni (2020) makes a cogent argument that the Supreme Court of India has cited poverty and trust in doctors as reasons to adopt a paternalistic view of informed consent, such that the doctors determine the amount of information to be given to the patient. Further, researchers like Gopichandran (2019), Subramani (2017, 2019), and Bhakuni (2020) have also commented upon the role of trust in defining the boundaries of doctor–patient relationship, emphasising how such trust is often at intersection of prevailing sociolegal conditions and the various social identities of the patient.
God, Fate, and Fatalism
Interestingly, the findings indicate pervasively high levels of attribution of decision responsibility to chance/luck and god, regardless of financial status or decision-making style. Previous studies suggest that belief in god, fatalism and doctrine of karma served as causal explanations for why the illness occurred, providing meaning to the patients’ suffering and facilitating acceptance of the reality of cancer (Kohli & Dalal, 2016; Sprik et al., 2021; Vardar et al., 2021).
There is scant literature that explores the role of attribution of decision responsibility in cancer treatment to god or chance/luck (Dalal & Misra, 2006; Kohli & Dalal, 2016). While most studies link belief in god or fatalism to positive physical outcomes (Sprik et al., 2021; Vardar et al., 2021), functional well-being (Leyva et al., 2014), sensemaking (Keeley et al., 2009), and positive coping (Vardar et al., 2021), few have investigated the role of belief in god and/or fate in cancer-related decision-making. For instance, Dopelt et al. (2022) using qualitative interviews explored cancer patients’ and family caregivers’ health locus of control with respect to clinical decision-making. They found that some patients relied on the belief in fate, leading them to adopt a passive stance in decision-making and refrain from asking questions. Few other researchers have explored cultural beliefs, such as fate, god and karma in relation to the attribution of cause of illness (Agrawal & Dalal, 1993; Dalal, 2000; Dalal & Misra, 2006; Kohli & Dalal, 2016). This study contributes to the limited literature as it investigates the extent of individuals’ attribution of responsibility to cultural metaphysical beliefs in cancer treatment decision-making.
Conclusion
Overall, this study deepens the understanding of how the individualistic decision-making styles (paternalistic versus shared) are linked to various crucial aspect of the decision process, particularly within the context of patients’ financial status (low versus high). Though shared decision-making is often characterised as a utopian concept (Gillman & Ferrer, 2021; Ozdemir & Finkelstein, 2018), the results indicate that a shift towards shared approaches does yield qualitatively superior outcomes in terms of increased trust in doctors and patients’ agency along with reduced emotional distress. The study also emphasises the role of cultural metaphysical beliefs in attributing responsibility for treatment decisions.
Further, it is crucial to acknowledge that the decision-making style is influenced by the contextual constraints of the patients. Given that a significant proportion of cancer patients in India come from financially disadvantaged backgrounds (Sathishkumar et al., 2022), this study makes substantial contributions by revealing that low financial status is associated with higher trust in doctors, lower patient agency and increased emotional distress for both patients and family caregivers. The move towards shared decision-making, considering the contextual realities of patients, could be instrumental in addressing critical issues, such as prevalence of collusion, superficial role of informed consent and high reliance on doctors’ authority or expertise. The shared decision-making approach promotes open communication between doctors, patients and family caregivers, offering a potential solution to mitigate these challenges.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.