
Abstract
Drowning is one of the most significant causes of unintentional death in developing countries and also one of the most grave causes of concern globally about injury-related fatalities in all autopsy cases. Drowning is a preventable cause of death and in recent times, the fatalities in drowning cases have been decreased due to community education, safety training and standard treatment protocols. The present cross-sectional retrospective study was conducted for four years from 2015 to 2019 in the Department of FMT at LSLAM Government Medical College, Raigarh, Chhattisgarh, to know the pattern of drowning cases with the distribution of cases according to year, season and activity of victims in all age groups and both sexes. In our study, out of a total of 2,244 autopsy cases, 3.61% of cases were of drowning. The maximum number of cases occurred in the rainy season, which is 41.98%. The maximum number of victims were males (74.07%), followed by females (25.93%) and the most commonly affected age group belongs to 21–30 years in 23.46% of cases. Maximum death occurred in ponds (32 cases, 39.51%), followed by rivers and dams. Most of the victims, that is 53.09%, were taking baths and in most cases (i.e., 58.02%), no significant history of the deceased was found. In our study, the maximum victims were identified (92.59%). About 25% of total drowning cases were found in the decomposed state. Accidental drowning cases are largely preventable, therefore by promoting educational awareness and training, swimming preferably in safe places under the observation of known and skilled persons may reduce the fatalities in drowning cases.
Introduction
Drowning is the process of experiencing respiratory impairment from submersion/immersion in water or any other fluid medium. Any submersion or immersion incident without evidence of respiratory impairment (aspiration) should be considered a water rescue rather than drowning.1, 2 Drowning is amongst the leading causes of death, which has been attributed to unintentional injury-related fatalities globally. According to the World Health Organization (WHO) report (2014), drowning is the leading but highly preventable global health issue in middle- and low-income countries, where data collection is limited, hampering the planning, implementation and monitoring of preventive measures. The same global report (WHO, 2014) also states that ‘every hour of every day, more than 40 people lose their lives to drowning’. 3 According to the Global Burden of Disease Study (2013), in 1990, the number of deaths due to drowning was 545,000 and in 2013, it was estimated to have resulted in 368,000 deaths. This accounts for 7.5% of all accidental deaths. 4 As per the National Crime Records Bureau—Accidental Deaths and Suicides (2013), in India, drowning was the third major contributor, which accounted for 7.5% of all unnatural causes of accidental deaths, to be superseded only by ‘road accidents’ (34.3%) and sudden deaths (7.8%). 5 In 2013, there were 29,456 deaths by drowning. 6 The present retrospective study was carried out to analyse and evaluate the incidences of morbidity and mortality in drowning cases with the scope of comprehensive research work in the future to lower the burden of disease-related deaths. It was also aimed to help investigating agencies and the judiciary in dealing with cases of drowning.
Materials and Methodology
The present cross-sectional retrospective study was conducted in the Department of Forensic Medicine and Toxicology at Late Shri Lakhiram Agrawal Memorial Government Medical College, Raigarh (Chhattisgarh). Permission from the institutional ethical review committee was taken before the commencement of the study. All the post-mortem records of drowning cases autopsied at the mortuary of Kirodimal Government Hospital (KGH), Raigarh (Chhattisgarh), had been considered for the research study. All cases other than drowning and cases with doubtful history were excluded from the study. People of all age groups from both sexes were included in the study. The study was conducted from 1 April 2015 to 31 March 2019 (four years). All the drowning cases were arranged after applying different variables such as year and season-wise distribution, age and sex wise distribution, location of recovery of body, the activity of the deceased before death, presence or absence of significant history, identification, state or condition of body during recovery and presence or absence of injuries in bodies of victims. The whole data was collected and then tabulated in Microsoft Excel sheets and then statistical analysis was done using SPSS (Statistical Package for the Social Sciences version 25.0, IBM Corp., Armonk, NY, USA).
Observations and Results
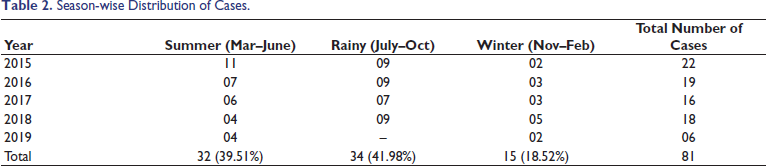
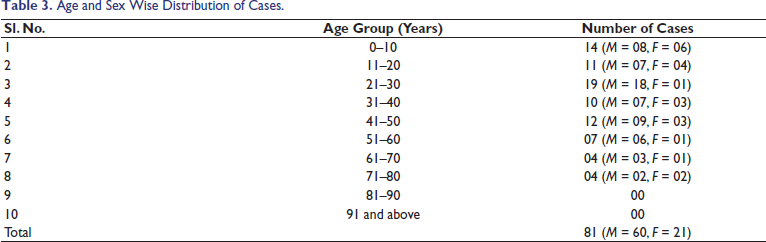
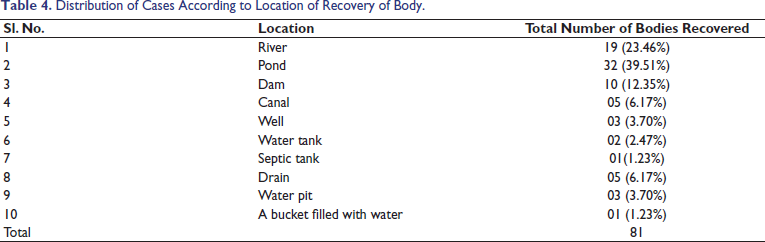
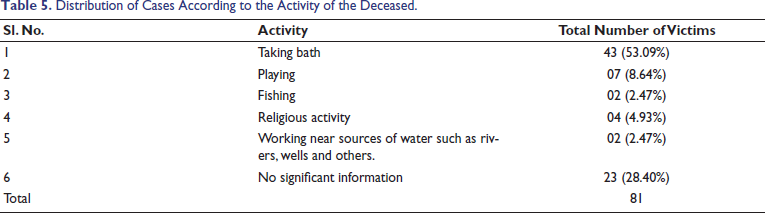
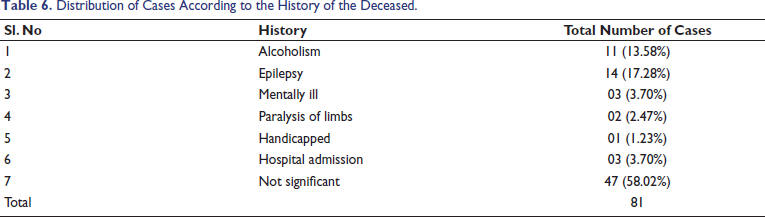
In our study, out of a total of 2,244 autopsy cases, 3.61% (81) of cases were of drowning. We have found the maximum number of cases of death due to drowning in the rainy season, which is 41.98%. The maximum number of victims were males (74.07%), followed by females (25.93%) and the most commonly affected age group belongs to 21–30 years in 23.46% of cases. In the maximum cases, death occurred in ponds (32 cases, 39.51%), followed by rivers and dams. While analysing the activity of the deceased before death, we found that most of the victims, that is 53.09% were taking baths. In most cases (i.e., 58.02%), no significant history of the deceased was found. In our study, most of the victims were identified (92.59%). About 25% of total drowning cases were found in the decomposed state. In about 16% of cases, antemortem injuries were reported, while in 12.35% of cases, signs of post-mortem injuries in the form of aquatic animal bites were also found. Table 1 shows the year-wise distribution of cases. In a four-year study, total drowning cases were 3.61% of total autopsied cases. Table 2 shows the season-wise distribution of drowning cases. The study shows that the maximum number of cases was recorded in the rainy season (34 cases, i.e., 41.98%), followed by the summer season (32 cases, 39.51%). The least number of cases were reported in the winter season (15 cases, 18.52%). Table 3 shows the distribution of cases based on age and sex. According to the table, the maximum deaths occurred in the 21–30 years age group (19 cases, 23.46%). In our study, among the total number of deceased males were 74.07% and females were 25.93%. Male-to-female ratio was 2.86:1. The predominance of male victims was observed in all age groups except in the 71–80 years. The table also shows that no death case was recorded after the age of 80 years. Table 4 shows the distribution of cases according to the location of the incidence and recovery of the body of the victim. The table shows that the majority of deaths occurred in ponds (32 cases, 39.51%), followed by rivers (19 cases, 23.46%) and dams (10 cases, 12.35%). Table 5 shows the distribution of cases based on the activity of the deceased prior to death. While analysing the activity of the deceased before death, we found that most of the victims were taking baths (43 cases, 53.09%) and in 28.40% cases, no significant information about the activity of the victim was found. Table 6 shows the distribution of cases based on the history of the deceased. According to the history of the deceased, in 37% of total cases, a significant history of the deceased was found (i.e., alcoholism, epilepsy, etc.) while in most cases (i.e., 58.02%), no significant history of the deceased was found. Table 7 shows that most of the deceased (75 cases, 92.59%) were identified and in 7.41% (06 cases) of cases, identification was not established. Out of total drowning cases, 25% of cases were found in a decomposed state, while 61 (75.31%) cases were recovered in normal condition. In 71.60% of cases, no injuries were found in the body during autopsy. In about 16% of cases, antemortem injuries were also reported, while in 12.35% of cases, signs of post-mortem injuries in the form of aquatic animal bites were also found.
Year-wise Distribution of Cases.
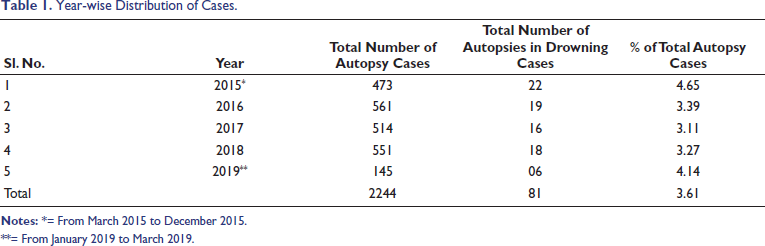
**= From January 2019 to March 2019.
Season-wise Distribution of Cases.
Age and Sex Wise Distribution of Cases.
Distribution of Cases According to Location of Recovery of Body.
Distribution of Cases According to the Activity of the Deceased.
Distribution of Cases According to the History of the Deceased.
Distribution of Cases According to Misc. Information.

**** = Post-mortem injury due to aquatic animal bites.
Discussion
The data collected and correlated in the present study reveal several interesting facts related to the mortality rate in drowning cases and the status of drowning in the Raigarh region of Chhattisgarh. In our four-year study, total drowning cases were 3.61% of total autopsied cases, which closely matches the study of Kuchewar et al. (2013) 7 and Radhakrishna et al. (2017), 8 where the authors respectively found 5% and 5.24% of total autopsy cases of drowning. From a medicolegal perspective, while this percentage aligns with regional trends, the autopsy surgeon must remain vigilant for atypical findings such as ‘dry drowning’ or vagal inhibition, where the absence of classic frothing or voluminous lungs can lead to a misinterpretation of the cause of death. Maximum cases were found in the rainy season (34 cases, i.e., 41.98%), followed by the summer season (32 cases, 39.51%). Similarly, the study of Phad and Dhawane (2018), 9 where 44% of total drowning cases were found in the rainy season. The seasonal surge during monsoons is often linked to flash floods and overflowing water bodies, which complicates cases between accidental slip-and-fall cases and intentional acts. This necessitates a careful distinction between accidental deaths due to environmental hazards and potential homicidal acts disguised by turbulent water conditions, as high-velocity water can produce artefacts that mimic traumatic injuries. Maximum death occurred in the 21–30 years age group (19 cases, 23.46%), which closely matches the study of Kuchewar et al. (2013), 7 Radhakrishna (2017), 8 Phad and Dhawane (2018), 9 Mukherjee et al. (2016), 10 and Mohanty et al. (2016). 11 Since this demographic data represents the peak productive age, these autopsies often carry significant legal weight regarding life insurance claims and civil liabilities, demanding precise documentation of any incapacitating factors. In our study, male victims were 74.07% and female victims were 25.93%, which closely matches the study of Mukherjee et al. (2016), 10 where males were 71.42% and females were 28.58%. The finding also nearly matches the study of Phad and Dhawane (2018), 9 where 72.02% victims were males and 28.98% were females. Even the studies of Sreekumar et al. (2021) 12 and Gorea et al. 13 showed that males are more prone to die by drowning. The high male-to-female ratio reflects greater outdoor exposure and risk-taking behaviour, but it also warrants mandatory toxicological analysis for alcohol or drugs to determine if the victim’s judgement was impaired, which is a vital factor in legal defence and determining the nature of the incident. In our study, the maximum number of deaths was recorded in ponds (32 cases, 39.51%), which matches the study of Rahman et al. (2009), 14 where 42.5% of total drowning cases occurred in ponds. Because ponds are relatively stagnant water sources, the application of the diatom test becomes a gold-standard medicolegal tool; the presence of site-specific diatoms in the bone marrow can act as crucial corroborative evidence to confirm that the drowning occurred at the recovery site and was not a case of post-mortem submersion to hide a homicide. In our study, the identity of the victim was established in 92.6% of cases, while the victims remained unidentified in only 7.4% of cases. This finding nearly matches the study of Radhakrishna et al. (2017),8 where 86% of cases were positively identified and 14% of cases were not identified. In the remaining 7.4% of unidentified cases, the medicolegal responsibility shifts toward forensic identification; failing to use scientific methods such as dental charting or Deoxyribonucleic Acid (DNA) analysis can result in a ‘corpus delicti’ challenge in court, hindering the justice process. Furthermore, antemortem injuries were reported in 16% of cases. These injuries are critical medicolegal ‘red flags’ that require a meticulous examination to distinguish between struggle marks from an assault and accidental injuries sustained during the drowning process.
Conclusion
Drowning is one of the serious causes of accidental asphyxial death. The present epidemiological autopsy record-based study pointed out several demographic parameters, including the decomposition, position and state of the body. Out of 81 cases, 20 cases were of decomposed bodies, which is around 25% of total autopsy cases. Though in medicolegal practice the diagnosis of drowning in decomposed corpses is often difficult to ascertain, the analysis of diatoms in putrefied corpses may reveal a fairly sound conclusion related to drowning as a mode of death. 15 Yet the quantitative and qualitative identification of diatoms in experienced hands provides the most reliable proof of drowning. 16 Apart from that, there are several examples where non-sending of the decomposed body to an anatomy expert to ascertain whether the hyoid bone and/or cervical vertebra was/were fractured or not was held fatal for the prosecution.17–19 Therefore, in cases of highly decomposed bodies and in all suspected cases apart from thorough autopsy examination, the opinion of the anatomy expert focusing on neck structures should preferably be considered to rule out any foul play. In Joshinder Yadav v. State of Bihar, 20 the Division bench of the Supreme Court of India, comprising Ranjana Prakash Desai and J. Chelameswar JJ., at paragraph 23, had observed the paramount importance of scientific evidence to counter the effect of a hostile witness. Therefore, it is also expected that the investigating agencies should increase the use of more scientific techniques/methods to achieve a higher conviction rate and help the judiciary in the process of achieving justice.
Confidentiality
The identity of the deceased and the autopsy surgeon was not disclosed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The Institutional Ethics Committee of Late Shri Lakhiram Agrawal Memorial Government Medical College had conferred its permission vide S. No/Med./Ethics Commi./2021/67, Raigarh, Chhattisgarh, India, dated 24 March 2021. All data were anonymized and handled in accordance with the ethical standards.
Sample Collection
Not required.