
Abstract
Eagle’s syndrome refers to the symptomatic elongation of the styloid process (SP) or ossification of the stylohyoid ligament (SHL), typically presenting with cervicofacial pain, dysphagia or vascular compression. While often symptomatic, a large proportion of cases remain undetected in life and are diagnosed incidentally during imaging or autopsy. This study represents three cases describing incidental findings of elongated SP (Eagle’s syndrome) found during routine medicolegal autopsies. Three adult males were found to have unilateral and bilateral elongated styloid processes or ossified SHLs without any prior history suggestive of Eagle’s syndrome. In our study, the length of the elongated styloid processes observed ranged 4.1–8.0 cm. In none of the cases was the causal relationship between this anatomical variant and the cause of death established. These autopsy findings highlight the clinically uninvestigated nature of many Eagle’s syndrome cases. Awareness regarding this entity becomes essential for both clinicians and forensic pathologists, especially when evaluating unexplained oro-facial pain, dysphagia and neurological complaints in life and also during medico-legal autopsy.
Keywords
Introduction
The stylohyoid chain is an anatomical structure made up of three main components: The styloid process (SP) of the temporal bone, the stylohyoid ligament (SHL) and the lesser cornu (horn) of the hyoid bone. The term styloid is derived from the Greek word stylos, which means ‘pillar’. The tip of the SP is connected to the hyoid bone through a lesser horn by the SHL, forming a continuous anatomical chain that spans from the skull base to the upper neck region.1, 2
Ossification of the SP typically begins between the ages of 5 years and 8 years and progresses gradually until approximately 30 years, after which its growth generally ceases. 3 In adults, the average length of the SP is about 25 mm. Usually, it is classified as elongated when it exceeds this length.4, 5 According to Moffat et al., 6 the normal length of the SP can range from 15.2 mm to 47.7 mm. 7
Although the majority of individuals with an elongated SP or calcified SHL do not exhibit symptoms, only a small percentage of individuals (approximately 1%–5%) may develop a constellation of clinical features collectively referred to as Eagle syndrome or styloid syndrome.8–10 When symptoms do occur, they are most commonly observed in individuals over 40 years of age.9, 11 Several terms have been used in the literature to describe symptoms linked to an elongated SP. These include ‘Eagle’s syndrome’, ‘SP neuralgia’, ‘stilalgia’, ‘elongated SP syndrome’, ‘carotid artery syndrome’, ‘stylohyoid syndrome’ and ‘pseudohyoid syndrome’. Each term reflects different clinical manifestations resulting from the anatomical elongation or ossification of the styloid apparatus. 5 The presentation of this condition can vary widely, from mild cervicofacial discomfort to severe complications such as cerebral ischaemia, depending on the anatomical structures affected. 12
This case series is significant for the incidental findings of markedly elongated styloid processes identified during routine medico-legal autopsies in individuals who remained clinically undiagnosed during life. Out of three cases, we observed bilateral involvement with asymmetrical elongation and pseudo-articulation in one case; extremely long styloid processes measuring up to 8.2 cm were observed, far exceeding the commonly described anatomical range. From a forensic perspective, the close relationship between the elongated SP, the calcified SHL and the carotid bodies was of particular importance, especially in one case where cervical movements resulted in dynamic compression of these structures. These observations emphasise the need for meticulous, layer-by-layer examination of the neck during autopsy and indicate that pronounced stylohyoid chain variations, though frequently asymptomatic, may have potential neurovascular relevance in cases of sudden or unexplained death. Moreover, we aim to review the existing literature on the subject, focusing on the anatomical variations of the SP.
Cases
Case One
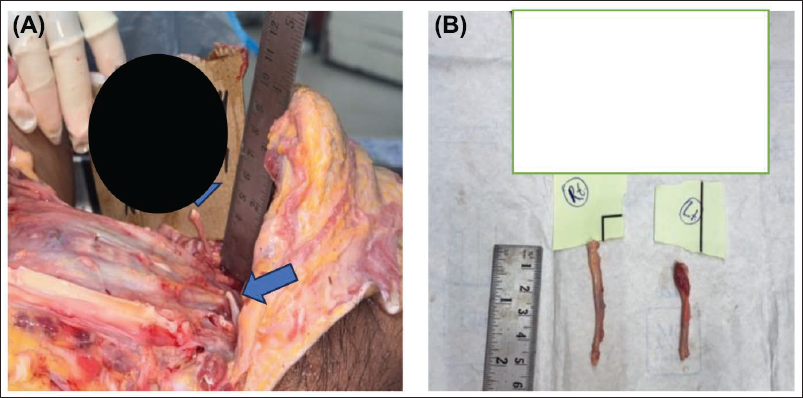
A 40-year-old male was brought to the hospital with a history of a self-fall at the workplace following an episode of dizziness and seizure, followed by a sudden loss of consciousness at home. He was managed conservatively and died during treatment. The corpse was shifted to the mortuary for a medico-legal autopsy. On autopsy, an external examination revealed multiple injuries on the head and face, which could have been caused by a fall. Cyanosis of the nail beds of both hands was present. Findings on internal examination showed a thick layer of subdural and a patchy thin layer of subarachnoid haemorrhage on the brain’s surface, and the rest of the other organs were unremarkable. The neck was examined in a modified-Y incision with a layer-by-layer dissection method under an avascular field, and the left styloid processes were elongated, directed forwards and downwards. The bony spines were six cm long and continued as calcified, stiff fibrous membranes, crossing obliquely downwards in the anterolateral aspects of the neck (Figure 1). It ran over the carotid bodies on the right side before attaching to the hyoid bone. Other structures in the neck were unremarkable. The cause of death given in this case was cerebral damage as a result of blunt force trauma due to a fall on a rough surface. History from family members suggests that he experienced neck pain followed by difficulty in neck rotational movement only sometimes, but he did not seek any medical checkup.
(A) Elongated Styloid Process with Stiff Fibrous Membrane on Left Side. (B) Dissected Out Elongated Styloid Process.

Case Two
A 40-year-old male was brought to the hospital with a history of a self-fall from the stairs of his house. Computed tomography (CT) showed haemorrhagic contusions in the bilateral frontal and temporal regions, with a subdural hematoma in the right frontal region and a frontal bone fracture. He was managed surgically (decompressive craniotomy), and despite all medical efforts, he died during the course of treatment. The corpse was shifted to the mortuary for a medico-legal autopsy. On autopsy, the external examination was unremarkable. Findings on internal examination showed signs of surgical intervention in the head with clean-cut margins, and the brain tissue was covered with clotted blood, gel foam and green-coloured pus. On the opening of the thoracic cavity, 500 mL straw-coloured fluid with oedema of both lungs was seen. The abdominal cavity contains one litre of straw-coloured fluid. The spleen was enlarged and congested. The rest of the internal organs were unremarkable. The neck was examined under an avascular field in a modified-Y incision with a layer-by-layer dissection technique, and both styloid processes were elongated, directed forward and downwards. The bony projections measured 5.4 cm on the right side and 4.2 cm on the left, extending as calcified, rigid fibrous bands that coursed obliquely downward along the anterolateral regions of the neck (Figure 2A). On the right side, the structure extended over both carotid bodies before anchoring to the hyoid bone. The right ligament was notably more prominent and, with movements of the cervical spine, such as flexion, extension and rotation, it caused slight compression of the right carotid sinus due to the thickened styloid-associated membrane (Figure 2B). The cause of death given was septicaemia in a case of cranio-cerebral injury as a result of blunt force trauma due to a fall from stairs. History from family members was inconclusive.
(A) Elongated Styloid Process with Stiff Fibrous Membrane on Both Sides. (B) Dissected Out Elongated Styloid Process.
Case Three
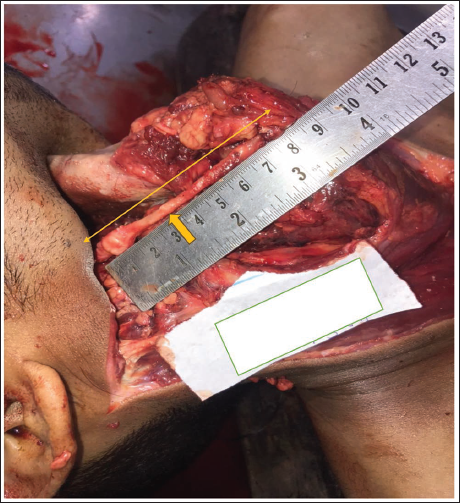
A 22-year-old male was brought to the hospital with a history of a road traffic accident (RTA). He was managed conservatively and died during treatment. The corpse was shifted to the mortuary for a medico-legal autopsy. On autopsy, external examination revealed multiple injuries all over the body, which were caused by RTA. Findings on internal examination showed a linear fracture of the skull vault and diffuse subarachnoid haemorrhage on the surface of the brain, and the rest of the organs were unremarkable. The neck was examined under an avascular field in a modified-Y incision with a layer-by-layer dissection method, and the left styloid processes were elongated, directed forwards and downwards. The bony spines were 8.2 cm long and continued as calcified, stiff fibrous membranes, crossing obliquely downwards in the anterolateral aspects of the neck (Figure 3). It ran over the carotid bodies on the right side before firmly attaching to the hyoid bone. Other structures in the neck were unremarkable. The cause of death given in this case was cranio-cerebral damage and its sequelae as a result of blunt force trauma. History from family members suggests that he sometimes complained of headaches and difficulty swallowing, but did not seek any medical checkup.
Elongated Styloid Process with Stiff Fibrous Membrane on the Right Side.
Discussion
Eagle’s syndrome is a rare clinical entity. It was first described in 1937 by Eagle. Eagle distinguished three groups: The first is the classic syndrome associating cervicalgia, otalgia and pharyngeal discomfort, the second is characterised by pain along the external carotid artery, and the third is asymptomatic. Palpation of the tonsillar fossae allows the diagnosis to be suspected. 13
The SP is a slender, pointed, bony projection originating from the inferior aspect of the petrous part of the temporal bone, situated just below the external auditory canal and anterior to the stylomastoid foramen and continues downward to attach to the SHL.3, 14 The tip of the SP is located within the pharyngeal wall, lateral to the tonsillar fossa. It is closely related to several critical neurovascular structures, including the internal carotid artery, internal jugular vein and cranial nerves X (vagus), XI (accessory) and XII (hypoglossal), which lie along its medial aspect.15–17 The SP is the point of origin for two ligaments, the stylohyoid and stylomandibular and three muscles: The styloglossus, stylopharyngeus and stylohyoid. These structures play a crucial role in stabilising the hyoid bone during various oropharyngeal activities such as swallowing and speaking.5, 18, 19
The entire stylohyoid chain, including the SP, SHL, lesser horn of the hyoid bone and the upper segment of the hyoid body, originates from Reichert’s cartilage, 20 which is derived from the second pharyngeal (branchial) arch during embryonic development.3, 20–22 The SP and lesser cornu of the hyoid bone are laid down in hyaline cartilage. 23 According to Steinman’s theory of anatomical variation, elongation of the SP is attributed to developmental anomalies arising during embryogenesis.3, 4, 24
Additionally, calcification of the SHL may occur following a tonsillectomy or trauma-induced scarring. Steinman explained this phenomenon through three theories: Reactive metaplasia, reactive hyperplasia and anatomical variation.3, 4, 24 Dwight suggested that mineralisation in the region of the SHL results from the ongoing development and ossification of the second branchial arch cartilage rather than being attributed to degenerative changes or the natural ageing process. 25 The underlying cause of SP elongation or SHL calcification remains a topic of debate.
Several theories have been proposed to explain the induction of ossification, including congenital factors, reactive metaplasia following local trauma, calcification associated with the ageing process, subtle neck trauma triggering an unregulated inflammatory response, callus deposition from subclinical styloid fractures and anatomical variations. 5 Ectopic calcification could play a role in the elongation of the SP. In patients with end-stage renal disease, disturbances in calcium, phosphorus and vitamin D metabolism are common and calcification associated with these abnormalities is often seen in this condition.2, 11
Variations of the SP include elongation, duplication, incomplete ossification, complete absence and calcification of the SHL. 26 Langlais et al. categorised elongated styloid processes into three types: Type I, an uninterrupted, elongated SP; Type II, an elongated process with a pseudo-articulation; and Type III, a segmented or discontinuous SP. 27 Cases one and three of our study correspond to Type III, characterised by a segmented SP. In this form, the normal SP is connected to adjacent ossified or cartilaginous segments of the SHL through fibrous or cartilaginous tissue, giving the overall appearance of an elongated SP on gross examination. 28 Case two of our study corresponds to Type I on the left and Type II on the right, as the elongated SP made a pseudo-articulation with SHL due to mild calcification.
Studies have shown that the incidence of an enlarged SP is higher in rural Indian populations. 11 The reported incidence of elongated SP ranges from 1% to 32% in the literature. However, the presence of an elongated SP is not enough to diagnose Eagle syndrome. Only a small percentage, approximately 4%–10.3% of individuals with an elongated SP experience the symptoms associated with Eagle syndrome. This highlights that the condition is relatively rare and requires further clinical evaluation beyond just the presence of elongation. 20
Elongation of the SP has been observed to occur more commonly in females.29, 30 Clinical studies have reported that women with this anatomical variation exhibit more noticeable symptoms than men. 31 Furthermore, a higher occurrence has been documented in postmenopausal women, suggesting a possible link between hormonal changes and the progression or symptomatic expression of the condition. 32 However, in our study, all cases were male, where we found elongation of the SP.
The literature identifies two distinct forms of Eagle syndrome: The classic and the stylo-carotid type variant. Classic Eagle syndrome results from irritation or compression of the glossopharyngeal nerve. It is typically marked by recurring throat and facial pain, a persistent sensation of a foreign object in the throat and difficulty swallowing (dysphagia).11, 12 Stylo-carotid syndrome is the vascular form of Eagle syndrome, characterised by pain and neurological symptoms along the course of the carotid artery, resulting from its compression by an elongated SP. 12 Interestingly, this syndrome may also occur without a visibly elongated SP, indicating that vascular impingement can happen without significant anatomical elongation.24, 33 In our study, cases one and three sometimes experienced symptoms, but they ignored them as they did not cause any substantial change in their daily routine.
Medially or laterally, deviated styloid processes can lead to carotid artery compression.21, 24, 33 When elongated, the SP may exert pressure on nearby structures, potentially irritating the carotid bodies and the vagus nerve and producing vagally mediated symptoms, which give rise to Eagle’s syndrome. 10 This can result in episodes of low blood pressure or reflex cardiac inhibition. 12 There are documented cases where an elongated SP has caused dissection of the carotid artery. 34 This serious condition can lead to cerebral infarction or subarachnoid haemorrhage, both of which may be fatal.
Three-dimensional CT scanning of the neck remains the primary tool for diagnosing Eagle syndrome. The surgical excision of the elongated SP may be considered for individuals with significant symptoms. 34 Because the syndrome can be influenced by head and neck posture, further evaluation using dynamic imaging, such as CT, magnetic resonance angiography or digital subtraction angiography, should be performed in different positions to observe potential compression or displacement of neurovascular structures. 35
Conclusion
In clinical settings, when patients present with unexplained, recurrent symptoms such as headaches, neck pain or stiffness, vertigo, episodes of low blood pressure or transient loss of consciousness, the possibility of Eagle syndrome should be considered as a differential diagnosis once more common causes have been excluded.
In forensic investigations, the presence of an elongated SP discovered during autopsy, particularly in cases of sudden and unexplained death, warrants careful evaluation of its potential role in neurovascular compression as a contributing or primary cause of death where no apparent cause of death is found after detailed autopsy and laboratory investigations. Additionally, a fracture of the elongated SP may be a significant finding for neck trauma. Such a finding can support the possibility of direct trauma or mechanical neck compression and may help establish the cause of death in cases where hanging or strangulation is suspected.
Footnotes
Acknowledgement
All the mortuary staff are gratefully acknowledged for the assistance provided during the autopsy and photography.
Authors’ Contribution
Munesh Kumar: Conception, design and drafting of the article.
Divyam Jain, Vijay Sharma, Shashank Tyagi and S. K. Tandon: Critical revision and approval of the version to be published.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed written consent was taken from the next of kin.