
Abstract
Suicide is a frequent cause of death, often executed through a particular method or means, and also one of the foremost causes of mortality worldwide. Complex suicide refers to instances where more than one method is employed to achieve death and these can be either planned or unplanned. The present series of six cases emphasises the necessity of a comprehensive medicolegal death investigation, which must include not only the performance of a complete forensic autopsy and toxicological evaluation but also the collection of collateral information through interviews with relatives, friends, potential witnesses, suicide notes and digital information to ascertain the cause and manner of death accurately.
In this case series comprising six cases, the most commonly employed method of suicide was hanging, frequently in combination with self-smothering and self-inflicted incised wounds. This was followed, in order of frequency, by thermal burns and ingestion of corrosive substances. A combination of hanging and self-smothering was observed in cases one and six. Furthermore, cases two and six exhibited hanging associated with self-inflicted incised wounds, along with evidence of smothering. The remaining cases demonstrated varied patterns, including thermal burns in association with incised wounds. In one case, ingestion of corrosive substances combined with self-inflicted incised wounds was documented. All six cases involved male individuals, indicating male predominance in this series.
Introduction
The act of intentionally taking one’s own life continues to be a significant public health concern worldwide. Suicide remains one of the leading causes of death across all age groups. According to the National Crime Records Bureau (NCRB), suicide rates in India have steadily risen from 9.9 per 100,000 population in 2017 to 12.4 per 100,000 in 2022. 1 The incidence varies significantly by state, with Bihar reporting the lowest rate at 0.6 per 100,000, while Sikkim has the highest at 43.1 per 100,000.
In 2022, the cities of Vijayawada (42.6 per 100,000 population) and Kollam (42.5 per 100,000 population) in southern India reported the highest suicide rates. 2 The distribution of suicide fatalities reveals a community’s mental and personal health information.3, 4
According to NCRB data on suicide in India, there has been a notable change in the patterns of suicide deaths among men, contrasting with trends observed among women. In 2014, suicide death rates (SDRs) among men were twice as standard as those among women, a ratio that increased to 2.5 times by 2021 as depicted in Figure 6.1, 2 The age groups with the highest suicide deaths among men were 18–29, 30–44 and 45–59 years, whereas for women, the highest incidence was observed in the 18–29 years age group. Among daily wage earners, there was a significant surge of 170.7% in suicide deaths among men from 2014 to 2021, resulting in an SDR of 34.6 among men compared to 13.1 among women in 2021. Similarly, unemployed men and women showed very high SDRs of 48.2 and 27.8, respectively. 2
Suicide rates among women showed a decline across all education levels, whereas men experienced an overall increase. The most significant rise was observed among men with education up to class 9–12, where the SDR increased from 22.6 to 30.0, reflecting a 66.4% surge between 2014 and 2021. The sex ratio of suicide deaths has risen from 2.3 to 3.7 times among men compared to women during the period from 2014 to 2021. Hanging emerged as the most common method of suicide, showing a 77.4% rise among men and a 51.3% increase among women during this period.5–7
Most suicides involve a single method; there are instances where individuals employ multiple techniques simultaneously to end their lives. The term ‘complex suicide’ is used when a person uses more than one method to take their own life.8–15
In complex suicide, individuals may use multiple methods, that is, more than one method is used, 16 such as hanging, drowning, poisoning, firearm discharge, jumping from heights, cut-throat or other possible methods. Sometimes, these cases resemble homicide due to multiple injuries and varied causes of death. Therefore, an autopsy surgeon or expert may encounter difficulty in differentiating death by suicide or homicide. 17 So, a thorough forensic investigation—including crime scene investigation, autopsy findings, toxicology reports and interviews with family or acquaintances—is essential in differentiating suicide from homicide. Medicolegal death investigators, forensic pathologists or experts and forensic nurses play a crucial role in piecing together the circumstances surrounding these deaths.17, 18
In this article, we present six cases of complex suicide cases where individuals employed more than one method to end their lives and were discovered only during medicolegal autopsy. Most of them were pronounced dead on arrival after being brought to the emergency room of the hospital. At the same time, two out of six cases arrived at the hospital in critical condition and passed away after a few days despite proper medical care. So, in such cases, to establish the exact cause of death, a meticulous postmortem examination, coupled with forensic and other laboratory findings, plays a vital role.
Cases
Case: One
A 20-year-old male was brought dead to the emergency room of the hospital at 1:20 am with an alleged history of hanging inside his rented house. His face was covered with multiple loops of adhesive tape, below the level of the lower eyelid to the chin anteriorly and the occipital region posteriorly (Figures 1A and 1B). Adhesive tape size 48 cm × 9.5 cm and four loops of green-coloured rope were present over the front of his neck and the other end of the rope was tied over the ventilation window in iron grills (Figure 1A). Both hands of the deceased were found inside the pockets of his pants (Figure 1A).
(A) The Death Scene Where the Deceased Was Found. (B) Depicts Congestion Below the Chin and Above the Upper Margin of the Ligature Mark Over the Neck. (C) Showed a Pale, Moist and Wrinkled Area Underlying Adhesive Tape. (D and E) Depicts the Underlying Ligature Mark Under the Skin, Subcutaneous Tissue, Neck Muscles and Other Structures.
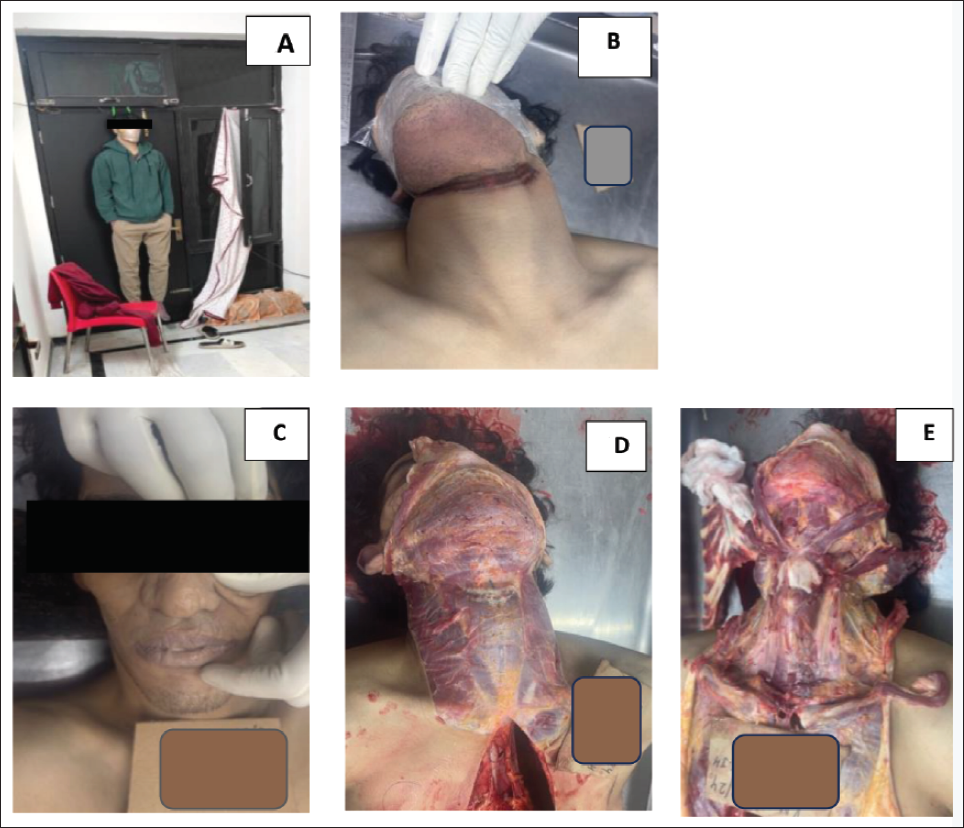
On postmortem examination, no evidence of external injury was found except for incomplete, brownish, abraded, parchment-like ligature marks on the front and both sides of the neck, which were placed obliquely and compressed by the multiple loops of adhesive tape. The area above the ligature mark to the chin (where the adhesive tape was present) is found to be congested and the area underlying the skin was pale, moist and wrinkled (Figures 1B and 1C). Conjunctivae, sclerae and face were unremarkable, with greenish discolouration noticed at the front of the abdomen. Postmortem staining was present in both upper and lower limbs, that is, gloves and stocking manner and was fixed; rigour mortis was subsiding. Internal examination revealed the congestion of all internal organs, such as the brain, lungs, liver and kidneys and petechial haemorrhages were found over the outer and inner lobar surface of both lungs in the interlobar region and inner coastal surface on both sides.
In the bloodless layer-by-layer dissection of the neck, the underlying skin below the ligature mark was pale and glistening. Underlying strap muscles, blood vessels, thyroid gland, thyroid cartilage, hyoid bone, cervical vertebrae, air passage and food passage were found normal and intact, as shown in Figures 1D and 1E. To rule out or detect any concomitant poisoning or intoxication, viscera and blood samples were preserved and the results were negative.
As per the crime scene investigation, next to the decedent, a roll of adhesive tape and a chair were found in front of his legs. Information provided by the police officials showed that the house doors were locked from the inside. The deceased was found hanged inside a room over another room door in a standing posture with his feet just above the ground level.
Upon further investigation, he had been staying alone in a rented house and had been observed alone several times since his disappearance, where he was found dead. His relatives or guardians said that recently, over a telephone conversation, he said his phone was broken for some reason and that he wanted to purchase a new one and the decedent’s father was provided the same recently.
Case: Two
A 31-year-old male was transported to the emergency room of the hospital at 1:05 am with a history of being found hanged on a ceiling fan inside the room of his house and was declared dead on arrival. The door was locked from the inside; her relatives saw him hanging through the window and the door was broken and opened with the help of neighbours. The corpse was shifted to the mortuary for a medicolegal autopsy. On external examination, the deceased was of average build, with multiple healed hypopigmented old scar marks suggestive of old incised or hesitation wounds present horizontally over the front of both forearms and wrist (Figure 2A). An oblique and incomplete, reddish-brown abraded ligature mark was present over the front and left sides of the neck, over and above the level of the thyroid cartilage, as shown in Figure 2C. The skin under the ligature mark was dry, hard and parchmentised.
(A) Multiple Old Healed Hesitation Scar Marks. (B) Depicts an Incised Wound on the Forearm, With the Underlying Effusion of Blood. (C) Shows the Ligature Mark.

Multiple Incised Wound on Image Depicting A. On Back of Right Hand; B. Left Forearm; C. Right Forearm; D. Front of Chest, E. Left Arm and Forearm, F. Inner Aspect of Left Forearm.

Two incised wounds of size 4 cm × 0.3 cm × subcutaneous tissue deep and 2 cm × 0.1 cm × subcutaneous tissue deep, respectively, present horizontally over the front of the left forearm with tailing towards the medial side, along with dried blood clots on adjacent sites as shown in Figure 2B.
Internal examination revealed congestion in all internal organs, such as the brain, lungs, liver, kidney, spleen, among others and subcapsular petechial haemorrhages were observed on the outer and inner lobar surface of both lungs. Around 300 mL of greyish liquid material without any peculiar smell was in the stomach. The cause of death was established as asphyxia due to antemortem hanging after a complete postmortem examination.
Case: Three
A 29-year-old male was transported to the emergency room of the hospital with a history of sustaining thermal burns injury due to a suicide attempt made using petrol and setting himself on fire (out of rage) on 3 July 2024 at 12:30 am. The fire was doused by his brother-in-law using a blanket. Initially, he was taken to a nearby district hospital and then to a tertiary care hospital, from where he took leave against medical advice and was brought and admitted to Safdarjung Hospital, New Delhi, on 6 July 2024 at 3:15 am. He died during treatment on 7 July 2024 at 2:40 am. The corpse was shifted to the mortuary for a medicolegal autopsy. On examination, the deceased was of average build. External injuries found on the body were the infected dermo-epidermal thermal flame burns with foul-smelling yellowish-green pus present all over the body, involving 65% of the total body surface area. There were multiple incised wounds of varying sizes ranging from 26 cm × 0.1 cm × 0.2 cm to 2 cm × 0.1 cm × 0.2 cm present vertically (mostly), obliquely and horizontally over the front and lateral aspect of bilateral upper limbs (five incised wound on the right upper limb and 54 incised wound on left upper limb), on front of the chest on both sides (34 in numbers) as shown in Figures 3A to 3F. Tailing towards the upper end in a maximum number of incised wounds, some of them on the lower and medial aspects. Internal examination revealed congestion in all internal organs, including the brain, lungs, liver, kidneys, spleen and others. The pleural cavity contained about 400 mL of coloured fluid on each side of the cavity and both lungs are congested and oedematous. About 300 mL of straw-coloured fluid was found in the abdominal cavity. Around 300 mL of greyish liquid material without any peculiar smell was in the stomach. The cause of death was established as septicaemia due to antemortem thermal flame burns after a complete postmortem examination.
Case: Four
A 65-year-old male was transported to the emergency room of the hospital with a history of sustaining thermal burns when the deceased lit himself on fire in the kitchen after cutting his abdomen with a knife on 6 August 2024 at 4:00 am. He was initially taken to the nearby district hospital and later to the City Super Speciality Hospital. He was brought and admitted to Safdarjung Hospital, New Delhi, on 9 August 2024 at 2:15 pm. He died during treatment on the sixth day of hospitalisation. The corpse was shifted to the mortuary for a medicolegal autopsy. On examination, the deceased was of average build. External injuries found on the body were infected dermo-epidermal thermal flame burns with foul-smelling yellowish-green pus present all over the body, involving 50% of the total body surface area and there were sutured wounds of length 17 cm present horizontally over the front of the abdomen, three cm above the umbilicus. On removal of sutures, the wound was abdominal cavity deep and the margins of the wound were regular, infected and smeared with yellowish pus. Internal examination revealed congestion in all internal organs, including the brain, lungs, liver, kidneys, spleen and others. The pleural cavity contains about 300 mL of straw-coloured fluid on each side of the cavity and both lungs were congested and oedematous. About 300 mL of straw-coloured fluid in the abdominal cavity. Around 50 mL of yellowish liquid material without any peculiar smell was in the stomach. The cause of death was established as septicaemia due to antemortem thermal flame burns after a complete postmortem examination.
As per the crime scene investigation, blood stains were found at places in his drawing room and blood stained knife was found at the crime scene; the rest of the crime scene was not disturbed. Information provided by the relatives to police officials that he was found sitting on the sofa when his son woke up early in the morning for the toilet. The house doors were closed.
Case: Five
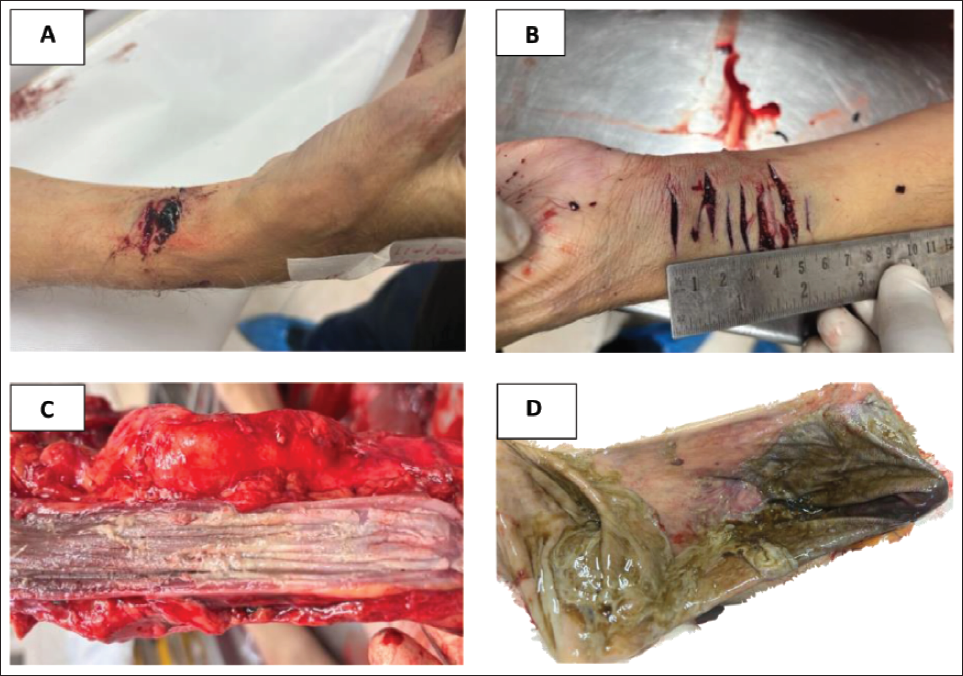
A 74-year-old male was transported to the emergency room of the hospital with a history of being found unconscious with injuries on both his hands at his residence and was declared dead on arrival. The door of his room was open. The corpse was shifted to the mortuary for a medicolegal autopsy. On external examination, the deceased was of average build and whitish froth was present in the mouth along with whitish discolouration of gums and teeth in patches. Dried blood stains were noticed over the front of both forearms with multiple incised wounds (four in number) of varying sizes ranging from 3.2 cm × 0.1 cm × subcutaneous tissue deep to 1.8 cm × 0.1 cm × subcutaneous tissue deep, were present horizontally over front of the distal right forearm with tailing towards medial side along with dried blood clots on adjacent sites as shown in Figure 4A. Multiple incised wounds (10 in number) of varying sizes, ranging from 3.7 cm × 0.5 cm × subcutaneous tissue deep to 1.5 cm × 0.2 cm × subcutaneous tissue deep, were present horizontally over the front of the distal part of the left forearm, with tailing towards the medial side, along with dried blood clots on adjacent sites as shown in Figure 4B. Internal examination of the mucosa of the oropharynx and the entire length of the oesophagus showed diffuse burnt areas with whitish discolouration, as shown in Figure 4C. Rupture of the stomach wall around the lesser curvature of the stomach, along with thinning of the wall. The consistency of the wall was firm and lathery; the serosal surface showed diffuse black discolouration of the entire wall, as shown in Figure 4D and loops of intestine, liver and spleen smeared with blackish stomach content. The cut section of all internal organs, such as the brain, lungs, liver, kidneys, spleen and others, was unremarkable. The cause of death was established as shock due to perforated peritonitis as a result of acid ingestion.
(A and B) Depicts Multiple Incised Wounds on Forearms, with the Underlying Effusion of Blood. Corrosive Acid Burn on the Entire Mucosa of the Oesophagus in Figure 4C and the Stomach in Figure 4D.
As per the crime scene investigation, blood stains were found at places in his room and a bottle of toilet cleaner was found near the body of the decedent; the rest of the crime scene was not disturbed. Information provided by the police officials showed that the house doors were open.
Upon further investigation, the decedent was staying alone and sent text messages to his son-in-law about his cremation by his daughter.
Case: Six
A 24-year-old male was transported to the emergency room of the hospital in an unresponsive state with a history of hanging at his residence and was declared dead on arrival. The door of his room was open. The corpse was shifted to the mortuary for a medicolegal autopsy. On examination, his mouth was covered with a loop of black cloth, tied posteriorly as shown in Figures 5B–5D. Four loops of red coloured electric wire were found around his neck and a knot was placed on the back of his head with one free end (Figures 5A and 5C). The deceased was of average build and had bluish discolouration of lips, both ears and nail beds of all fingers. Glove and stocking pattern hypostasis present over both upper and lower limbs. Dried blood stains were noticed over the front of both forearms and neck with underlying horizontally placed incised wounds (one in number on each site) of varying sizes measuring 4.5 cm × 1.3 cm (margins un-opposed) × subcutaneous tissue deep on front of left forearm distally, 4.1 cm × 1.2 cm (margins un-opposed) × subcutaneous tissue deep on front of right wrist as shown in Figure 5A and 7.1 cm × 0.8 cm (margins un-opposed) × muscle deep over front of the neck with exposed neurovascular bundle and muscles with tailing towards left side along with dried blood clots on adjacent sites. An oblique and incomplete, brownish abraded ligature mark was present over the front and left sides of the neck, over and above the level of the thyroid cartilage, as shown in Figures 5B and 5C. The skin under the ligature mark was dry, hard and parchmentised.
(A, B and C) Depicts Incised Wounds on the Forearm and Neck with the Underlying Effusion of Blood. Brownish Ligature Mark on the Neck in Figure 5B and Red Coloured Wire Around the Neck in Figure 5C. (D and E) Depict Crime Scene Pictures Showing a Black Coloured Rope in 5D and a Yellow Arrow Depicting a Phone with a Blood Stained Knife and a Red Arrow Depicting Blood Stains in 5E.

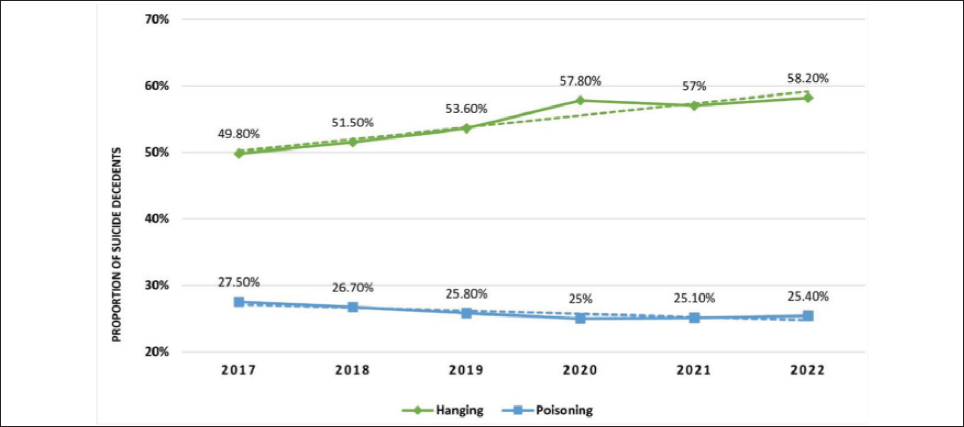
Depicting Trends in the Major Means of Suicide with the Time in India from 2017 to 2022.1,2
Internal examination revealed congestion in all internal organs, such as the brain, lungs, liver, kidneys, spleen and others and subcapsular petechial haemorrhages were found over the outer and inner lobar surface of both lungs. Around 150 mL of yellowish liquid material without any peculiar smell was in the stomach. The cause of death was established as asphyxia due to antemortem hanging after a complete postmortem examination.
As per the crime scene investigation, he was found hanged with the ceiling fan and blood stains were found on the mattress of the bed at places, black rope, phone and a knife were found on the bed near the body of the decedent; dried blood stains were present on knife and a suicide note was found on crime scene (Figures 5D and 5E). The rest of the crime scene was not disturbed. Information provided by the police officials showed that the room doors were closed.
Upon further investigation, the decedent stayed alone and was a student who had invested his money somewhere, which he lost.
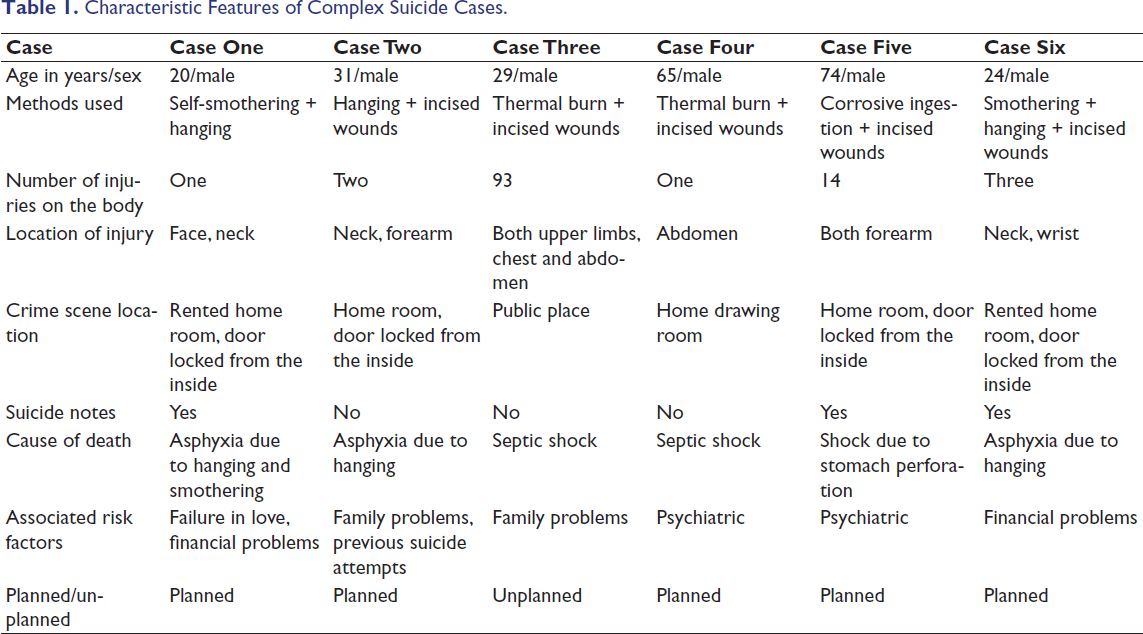
In brief, the details of all six cases are summarised in Table 1.
Characteristic Features of Complex Suicide Cases.
Discussion
Complex suicide occurs when a victim uses multiple (two or more) methods to end their life. 16 Studies have documented that complex suicides account for roughly 1.5%–5.6% of cases reviewed in forensic investigations.8, 15, 19–23 Complex suicide is mainly reported in males sex as compared to women, as per available literature.17, 19, 21, 24 In our case series, all of the decedents were male. The majority of complex suicides are committed at home. 19 In our study, five out of six complex suicide committed at home.
The method of suicide varies across different geographical regions and cultural backgrounds. Popularly used methods in complex suicides are gunshot injury, hanging, jumping from height, insecticide and drug poisoning, drowning, self-strangulation, cutting and stabbing.8, 21, 25–31 Road traffic accidents with vehicles, electrocution, foreign body and corrosive or plaster of Paris ingestion, self-burning and nicotine patch use were rarely reported cases.22, 32–40
The most frequently observed suicide method in this study involved the ingestion of one or more medications in toxic or lethal doses. Petković et al. documented a case of complex suicide in which the victim employed six different methods. 20 In our study, three different methods to commit suicide were employed together at the same time in one out of six cases; the remaining five cases employed two methods.
Hanging remains one of the most commonly employed methods, while poisoning, self-inflicted sharp-force injuries and jumping from heights are also frequently observed.41, 42 In cases of complex suicide, the individual often attempts an initial method that is less lethal before resorting to a fatal approach, either due to failure of the first attempt or an escalation in psychological distress. 43 In our study, the combination of methods used was self-inflicted injury with thermal burn in two cases, self-inflicted hesitation cuts with hanging, self-inflicted hesitation cuts with corrosive acid poisoning, self-smothering with hanging and self-inflicted hesitation cuts with self-smothering followed by hanging in one case (case six).
The lethality score refers to the proportion of completed suicides relative to unsuccessful attempts using a specific method. One of the most widely recognised lethality score assessments was developed by a group of American researchers who analysed over 4,000 cases of suicide and attempted suicide using 28 different methods over five years. 44 Their findings indicated that the lethality score for hanging is approximately 89.50 ± 4.38. In cases of unplanned complex suicide, the initial attempt often involves a method with a lower lethality rate compared to the subsequent method chosen after the first attempt fails. 45 Additionally, men are more likely than women to use techniques associated with a higher lethality rate. In our study, one case (case three) initially employed to make multiple incised wounds on the accessible parts of his body as a suicide method with a low lethality rate, followed by setting himself on fire.
Complex suicides are categorised into planned (primary) and unplanned (secondary) types.21, 46 Planned complex suicides involve premeditation, where the individual secures multiple high-mortality means of death in advance to end his or her life or leaves behind evidence of intent, such as a suicide note.17, 19, 21, 22, 36, 39, 40, 47–49 When one suicide method fails, another may be attempted to complete the act. The presence of multiple fatal techniques indicates strong resolve, though the deceased’s exact reasoning cannot be determined. In unplanned complex suicides, the individual may first attempt a less lethal method, such as self-inflicted cuts, also known as hesitation cuts, before switching to a fatal act such as hanging or jumping or other methods that the victim can adopt.8, 10, 14, 17, 18, 21, 27, 50 This escalation is likely driven by increasing physical pain and emotional turmoil. 11 Five out of six cases were planned and only one case was counted as an unplanned complex suicide in our study. The pattern observed in our cases suggests that individuals may initially attempt non-lethal self-harm before progressing to more fatal means.
Available literature depicts that, in planned complex suicide, toxic doses of hypnotic or other drugs are administered before hanging or suffocation by plastic or hanging with gunshot injury or gunshot injury with drowning in water, 18 incised wounds on the wrist with hanging, 24 insecticide poisoning with gunshot injury or jump from height, 19 hanging with gunshot injury. 21 Corrosive acid poisoning followed by cyanide poisoning and corrosive poisoning followed by jumping from a height has also been reported in a planned complex suicide. 51
In contrast, planned complex suicides often involved premeditated ingestion of lethal drugs, either as the primary method of suicide or to minimise pain before using another method.
Many individuals in planned suicides consumed sedatives or hypnotic drugs before using another method, possibly to ease the pain associated with a more violent act. Researchers have debated whether drug intake in such cases serves purely as a suicide method or if it is meant to reduce suffering from a secondary method. As per the available literature, stabbing or jumping from a height is unplanned, whereas ingestion of toxic drugs18, 51 is the most commonly used method in planned complex suicides. Use of toxic drugs such as sedatives or hypnotic drugs to get motivation or to reduce the pain of the second method is debatable. To clarify this distinction, some forensic specialists have categorised cases as ‘drug-related complex suicides’ and ‘drug-unrelated complex suicides’. 21 However, in most instances, evidence from toxicology reports and crime scene investigations confirms suicidal intent when high doses of drugs are present. 19
In suicide cases, the surroundings typically remain unchanged and objects used in the act are usually found near the deceased. 52 In our study, in five out of six cases, the surroundings remained undisturbed, a sharp weapon was used for self-inflicted injury and the objects used in complex suicide were found near the body. However, homicide investigations may reveal disturbances at the scene, signs of physical struggle or missing weapons, pointing to possible external involvement.
The present study demonstrates the dilemma faced by the forensic pathologist in distinguishing complex suicide from homicide cases where more than one type of injury was present. In case one, the methods involved were hanging and smothering, using adhesive tape. In case two, there was hanging with self-inflicted incised wounds; in cases three and four, there were incised wounds followed by fatal thermal burns; in case five, there was corrosive ingestion with incised injuries; and in case six, there was a combination of hanging, smothering and incised wounds. In all six cases, the presence of multiple injuries initially raised suspicion of homicidal assault.
On meticulous autopsy examination, the findings were suggestive of self-inflicted injuries, including hesitation cuts, as the injuries were limited to accessible body parts, the direction of incised wounds found on the body, the absence of defensive injuries and neck findings consistent with antemortem hanging.
Toxicological analysis did not demonstrate any underlying poisoning or intoxicating substances and, where applicable, supported the alleged mode of self-harm, except in case five, who consumed a corrosive substance with hesitation cuts. According to the crime scene examination report, no evidence of struggle or disturbance was found, with recovery of the materials used for self-harm, a suicide note and the room was found locked from the inside. Circumstantial evidence and information provided by the investigating officer, relatives and other witnesses, including a history of prior self-harm, psychosocial stressors or suicide notes, provided essential support. We determined the cause and manner of death after correlating the autopsy findings with toxicology results, crime scene findings and circumstantial history, highlighting the importance of a comprehensive and systematic forensic approach in cases of complex suicide.
Forensic experts analyse the content, handwriting and authenticity of a suicide note found at the crime scene to determine its credibility and its role in confirming the manner of death.19, 21, 49, 53 Studies show that in around 20%–50% of complex suicides, a note is left behind, either handwritten, typed or in digital form.19, 21, 49 In our study, suicide notes were found in three out of six cases (50%).
Suicidal behaviour typically follows a progression from thoughts of self-harm to actual self-inflicted injury and, in some cases, a fatal outcome. Studies have shown that individuals with a history of mental illness or prior self-harm are more likely to attempt suicide.23, 54 Hesitation wounds and repeated nonfatal self-inflicted injuries are vital signs that may indicate a higher risk of future suicide attempts.23, 54 In our study, we have found old hesitation or self-inflicted injury marks in one case (case two).
Psychiatric disorders such as bipolar disorders, schizophrenia, depression and borderline personality disorders were a significant factor in suicide, with emotional or physical pain often cited as a contributing cause.17, 19, 21, 29, 33–36, 39, 55, 56 However, distress alone is generally insufficient; feelings of hopelessness have been identified as a crucial determinant in the transition from suicidal thoughts to action. 23 In this study, two cases were found to be suffering from a psychiatric illness.
Research indicates that when a suicide attempt does not result in death, some individuals may make another attempt using a more lethal approach. 11 The progression from a less harmful effort to a more lethal one indicates a strong determination to end life rather than a momentary act of self-harm. Distinguishing complex suicide from homicide can be difficult, particularly when multiple injuries are involved. Forensic evidence plays a critical role in determining the manner of death, as self-inflicted injuries in suicide cases are usually found on easily reachable areas of the body, often accompanied by hesitation wounds in the form of shallow, parallel cuts. 11 As we found in our case study three, multiple, superficial and parallel incised wounds were found only on the accessible parts of the body by shaving the blade, followed by setting himself on fire and in case four, a deep incised wound on the front of the abdomen, followed by setting himself on fire.
Unlike self-inflicted wounds, homicidal injuries tend to be more forceful and uneven and frequently show signs of struggle, such as cuts or bruises on the hands and forearms.
Suicide investigations frequently uncover prior mental illness, earlier suicide attempts or deliberate drug or alcohol consumption. Toxicology screenings can verify self-administered substances. Distinguishing between suicide and homicide requires a comprehensive forensic investigation that includes an analysis of injury patterns, toxicology reports and crime scene findings. Investigators must carefully examine all aspects before determining the manner of death. 57
In our case series, four incidents began with a nonlethal attempt, followed by a fatal act. The presence of hesitation wounds, absence of defensive injuries and an undisturbed scene of crime, statements of relatives and available digital data strongly indicated suicide rather than homicide.
The primary causes of suicide include family conflicts, health issues, unknown reasons, substance abuse and financial distress, such as bankruptcy or sudden economic downturns, which together account for over 80% of cases. According to the NCRB data in India, bankruptcy or indebtedness (4.1%), marriage related issues (4.8%), failure in examination (1.2%), impotence/infertility (0.2%), family problems (31.7%) and illness (18.4%), death of dear person (1.2%), drug abuse/alcoholic addiction (6.8%), fall in social reputation (0.5%), ideological causes/hero-worshipping (0.1%), love affairs (4.5%), poverty (0.8%), unemployment (1.9%), property dispute (1.1%), suspected/illicit relation (0.5%), illegitimate pregnancy and physical abuse (0.0%), professional/career problem (1.2%), not-known causes (10.4%), other causes (10.5) are among the leading contributing factors to suicide (NCRB, 2022). 2 Additional risk factors often involve economic hardship, social withdrawal and a history of mental health disorders. 55
In complex suicide scenarios, such as in our case one and six, where the deceased was found both smothered and hanged by a ligature, interpreting the combined scene of crime evidence and autopsy findings becomes particularly challenging. Forensic pathologists faced a dilemma in determining the sequence of events or establishing whether the smothering was self-inflicted or inflicted by another person, as both mechanisms are independently capable of causing death. In such cases, close collaboration with crime scene experts, toxicologists, mental health professionals and law enforcement investigators is essential to arrive at a reliable opinion.
Forensic nurses with medical knowledge who are trained in forensic sciences play a vital role in death investigations by assessing injuries, documenting medical histories and providing support to the deceased’s family during the legal process. 58
Examining medical records and speaking with family members through psychological autopsies helps uncover details about the deceased’s mental health and possible stressors before death. 55
The complexity of cases in our study underscores the need for a comprehensive forensic examination, including toxicology analysis, scene investigation and a review of the deceased’s mental health history. Without these factors, differentiating between suicide and other causes of death remains difficult. Strong suicide prevention strategies should be adopted and focused on early detection, immediate care and community-driven support systems to help individuals through difficult times.
Conclusion
Identifying whether multiple self-inflicted injuries were part of a complex suicide or staged to mimic homicide requires expertise in forensic pathology and crime scene reconstruction. Forensic experts play a key role in understanding the cause of death while also contributing to suicide prevention through mental health awareness and crisis intervention efforts.
Understanding the forensic and psychological aspects of complex suicide is essential for accurate medicolegal evaluations and for informing public health strategies aimed at suicide prevention. A precise determination of the cause and manner of death depends on a comprehensive forensic examination involving scene investigation, autopsy and toxicology testing.
Footnotes
Acknowledgement
All the mortuary staff are gratefully acknowledged for the assistance provided during the autopsy and photography.
Authors’ Contribution
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed written consent was taken from the next of kin.