
Abstract
The COVID-19 pandemic, like other highly contagious outbreaks, has forced us to rethink and adjust many aspects of daily life. In the medical world, most fields have quickly developed new methods or adapted existing ones to reduce the risks posed by the virus. Forensic pathology, which often involves high-risk aerosol-generating procedures (AGPs) during autopsies to investigate deaths from unknown causes, faces the same challenge. The need to protect healthcare workers in this area has become more critical than ever.
In light of this, the authors present an alternative method for removing the brain during autopsies in post-craniotomy cases, eliminating the need for the traditional approach of sawing through the skull. This technique reduces the risk of generating aerosols, which are a primary mode of transmission for airborne infections. Importantly, the method can be applied to all cases, regardless of whether the deceased is suspected of carrying an infectious disease, making it a versatile and safer option.
This innovative approach shows how forensic pathology can evolve to meet the safety demands of the pandemic without sacrificing the quality of the investigation. By reducing the risk of exposure to infectious agents, forensic pathologists and other professionals involved in post-mortem procedures are protected. In a time when infection control is a top priority, such changes to traditional practices help ensure that crucial medical examinations can continue safely.
Keywords
Introduction
It is not advisable to perform an autopsy on the COVID-19 case, even for diagnosis, let alone the academic interest.1–4 However, this recommendation may not be feasible in all circumstances in the practice of forensic pathology, as one gets to see unexpected sudden deaths, suicides, custodial deaths, homicides, and other high-profile cases with either a confirmed or suspected COVID-19 diagnosis. Here, it becomes an obligation for the pathologist to perform a complete medicolegal autopsy. Still, there remains a potential risk that the virus could persist on the bodies of the deceased, as viable SARS-CoV-2 has been shown to survive on surfaces for several days.5, 6 A complete autopsy on a COVID-19 body needs a team of highly trained forensic pathologists and infrastructures such as a negative-pressure Biosafety Level 3 autopsy suite, which is not available at many autopsy centers, especially in resource-constrained nations.3, 7 Hence, minimal invasive autopsy techniques have been recommended in all such cases to minimize unnecessary hazardous procedures.8, 9
Skull vault opening using an electric saw is one such aerosol-generating procedure (AGP) that increases the possibility of transmission of COVID-19. 10 Even though the electric saws are complemented with vacuum units, they are still considered unsafe because of their inefficiency to completely collect the bone dust and other tissue fragments emanating from high-speed sawing. 11 Though these AGPs are inevitable in cases where the brain is the organ of interest, the authors still believe that there should be some workaround for brain removal, at least in autopsies where surgical craniotomies have already been done. Many methods are being tried to overcome the negative effects of conventional autopsies in these COVID times. 12 It is in the same context; a new method has been developed and adopted by the authors and discussed in this case study.
Craniotomy, Types, and Indications
Craniotomy, a procedure involving the temporary removal of a section of the skull to access the brain, has a long and evolving history. Its earliest forms can be traced to prehistoric times, where it was believed to serve ritualistic or spiritual purposes, such as releasing malevolent spirits. Ancient Egyptians adapted the fire-making bow drill for cranial procedures as early as 1400
A craniotomy is the surgical removal of part of the calvarium (skull) to expose the brain. This removed portion of the bone is called the bone flap. The bone flap may be temporarily removed and replaced after the neurosurgical intervention. The bone flap, after removal, may be stored in the abdominal wall or a bone bank.16, 17 In cases of compound fractures, where the bone is fragmented, multiple pieces may need to be discarded during the procedure, as they cannot be effectively replaced.
Craniotomy surgeries are performed for a variety of traumatic and non-traumatic skull and brain pathologies, including brain tumors; clipping or repairing an aneurysm; removing arteriovenous malformations; evacuating blood or blood clots from a leaking blood vessel; addressing arteriovenous fistulas; draining brain abscesses; repairing skull fractures or tears in the dura mater; relieving intracranial pressure (ICP) by removing damaged or swollen areas of the brain due to traumatic injury or stroke; treating epilepsy; and implanting stimulator devices to manage movement disorders such as Parkinson’s disease.16, 18, 19
There are several types of craniotomies, categorized based on factors such as the location of the pathology, ease of access, maximum safety, and minimal damage to surrounding organs and tissues. In neurosurgical and forensic practice, various craniotomy techniques—commonly referred to as surgical “corridors”—are selected based on clinical indications, lesion location, and required exposure. The following sections briefly outline several key approaches commonly employed in both therapeutic and postmortem settings.
Frontotemporoparietal (FTP) craniotomy: The FTP approach is frequently utilized in cases of traumatic brain injury, particularly when prompt decompression is essential. This technique involves the removal of a bone flap that spans the frontal, temporal, and parietal regions, allowing wide exposure of the cerebral cortex. In resource-limited environments, a modified version with liberal duroplasty and bone replacement during the same procedure can offer an effective, single-stage intervention without compromising outcomes. 20
Decompressive craniectomy: Decompressive craniectomy is typically employed in patients with elevated ICP that is unresponsive to medical therapy. By removing a substantial portion of the skull, this approach allows the swollen brain to herniate outward, thereby reducing ICP and minimizing further neurological damage. It remains a cornerstone procedure in the management of malignant cerebral edema. 21
Pterional craniotomy: One of the most established neurosurgical corridors, the pterional craniotomy grants access to the anterior and middle cranial fossae. It is especially useful in managing aneurysms, skull base tumors, and arteriovenous malformations. The technique offers excellent exposure of the Sylvian fissure and related neurovascular structures, with minimal cortical disruption. 22
Frontotemporal craniotomy: The frontotemporal craniotomy provides targeted access to the frontal and temporal lobes. It is frequently employed for lesion resections, hematoma evacuation, and vascular interventions, offering surgeons a direct route to the lateral fissure and deeper basal structures. 23
Bifrontal craniotomy: This bilateral approach enables comprehensive visualization of the anterior cranial fossa and is ideal for managing midline pathologies or diffuse frontal contusions. It is often used in decompressive surgeries where symmetrical cerebral decompression is required. 24
Minimally invasive supra-orbital keyhole craniotomy: This technique, accessed through an eyebrow incision, allows for less invasive entry to the anterior cranial base. It is well-suited for the resection of small tumors and aneurysms, particularly in cosmetically sensitive areas. The reduced operative footprint often translates into faster recovery and reduced complications. 25
Retro-sigmoid craniotomy: Primarily utilized for posterior fossa surgeries, the retro-sigmoid approach is favored in the management of cerebellopontine angle lesions such as vestibular schwannomas. It provides sufficient exposure while preserving important neurovascular structures. 26
Orbitozygomatic craniotomy: This extended approach involves removing portions of the orbital rim and zygomatic arch to improve access to deep-seated tumors and vascular lesions. It minimizes brain retraction while optimizing visibility of the skull base and surrounding anatomy. 27
Translabyrinthine craniotomy: This skull base technique provides access to the cerebellopontine angle while intentionally sacrificing residual hearing. It is most commonly indicated in patients with non-serviceable hearing undergoing resection of vestibular schwannomas. 28
Suboccipital craniotomy: The suboccipital approach is traditionally employed to access the posterior cranial fossa, particularly for resection of cerebellar tumors or decompression in Chiari malformations. It allows for safe entry to the brainstem and fourth ventricle while preserving critical posterior circulation structures. Among these, FTP craniotomy is the most commonly performed in traumatic cases, which are frequently encountered in medicolegal autopsies.16, 18, 19, 29
Surgical FTP Craniotomy Procedure
The surgical FTP (frontotemporal parietal) craniotomy procedure typically begins with a C-shaped or question mark-shaped incision made on either side of the scalp. The upper anterior portion of the incision is usually positioned above the corresponding eyebrow, while the lower posterior end is placed near the upper attachment of the corresponding ear. Once the scalp has been incised, the next step involves removing the bone over the skull vault at the site of interest. This is achieved by creating burr holes at the margins of the area, followed by sawing to connect these burr holes, thereby freeing the bone flap. The excised bone flap is often temporarily stored in the patient’s anterior abdominal wall, thigh, or in a bone bank, and it is typically replaced once the surgery is complete and the patient has sufficiently recovered.20, 30
The Procedure of Skull Opening and Delivery of Brain in Conventional Autopsy
During a conventional autopsy, the procedure of skull opening and brain removal follows a systematic approach. Initially, a bimastoid incision is made through the full thickness of the scalp. The scalp flaps are then reflected anteriorly to the level of the supra-orbital ridges and posteriorly to the occipital protuberance using a combination of sharp and blunt dissection techniques. The temporalis muscles are carefully dissected away from their origins on both sides. The cranium is subsequently opened using either a mechanical or electrical saw, with the sawing line extending above the superciliary ridges in the front and through the occiput at the back. It is important to note that the use of an electrical saw in this step generates significant aerosols. The skullcap is then removed by gently inserting and twisting a chisel along the cut line, which facilitates the opening of the skull.
Once the skullcap is removed, the external surface of the dura mater is inspected. The dura is then cut along the sawing line and gently pulled back after the anterior attachment of the falx cerebri has been detached. The frontal lobes of the brain are carefully lifted from the anterior cranial fossa while basal attachments are severed. With continued lifting and slight traction applied to the undersurface of the cerebral lobes, the tentorium cerebelli is incised along the superior border of the petrous bone bilaterally. This allows the tentorium to be reflected posteriorly, exposing the cerebellum and brainstem.
At this point, the cervical cord and its attachments are severed as far inferiorly as possible through the foramen magnum. The cerebellar lobes are then digitally scooped from their respective fossae, enabling the delivery of the brain, including the brainstem, in its entirety. Final, the dura mater can be stripped from the inner surface of the skull, allowing the base of the skull to be examined for fractures or other abnormalities.31–35
Proposed Modified/Minimal Invasive Approach
The proposed modified, minimally invasive approach for brain removal during autopsy has been applied in three cases at the Department of Forensic Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh. All of these cases involved roadside accidents and had undergone FTP craniotomy as part of their surgical management. This approach aims to deliver the brain in clearly defined parts through the pre-existing FTP craniotomy defect, thereby minimizing procedural artifacts and avoiding the use of electric sawing, which is considered an AGP.
Autopsy Technique
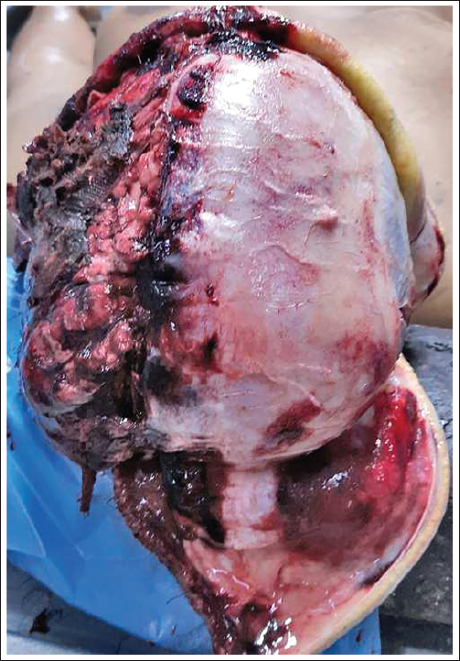
The initial steps, such as placing the body, positioning the head, and documenting external findings, remain consistent with conventional autopsy procedures.31–33 Upon examining the head in post-craniotomy cases, one may observe the craniotomy wound margins either fully healed or in various stages of healing. In cases with minimal healing, the wound margins can be manually separated without the use of instruments, and the scalp is reflected away from the wound margins (Figure 1). To facilitate the process, an incision is made from the contralateral mastoid process, intersecting the craniotomy wound perpendicularly. The scalp flaps thus created are reflected anteriorly and posteriorly (Figure 2). If the craniotomy margins are completely or nearly healed, a regular bimastoid incision may be used.
Downward Reflection of the Dura Mater to Expose the Underlying Cerebral Hemisphere.

Scalp Flaps Reflected Anteriorly and Posteriorly at the Midsagittal Region.
After reflecting the scalp, the skull vault, craniotomy defect, and the undersurface of the scalp are exposed. Special care should be taken during this step, as craniotomy involves the removal of a section of cranial bone, and a deep incision may inadvertently injure the brain. Furthermore, when removing staples from the craniotomy wound, attention should be paid to prevent the sharp ends of the staples from injuring gloved fingers.
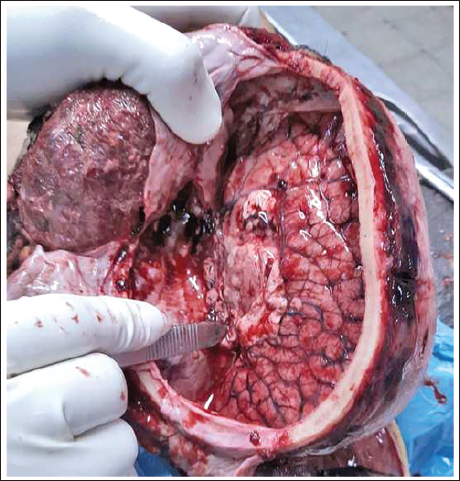
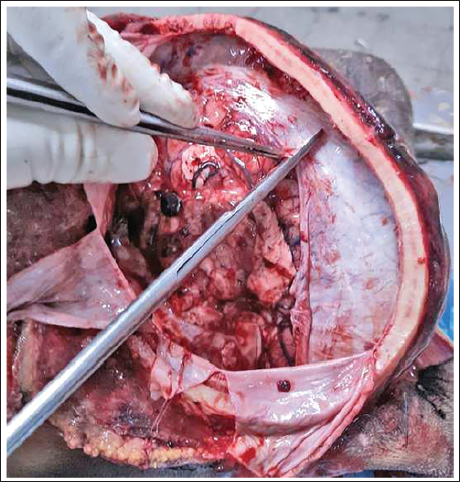
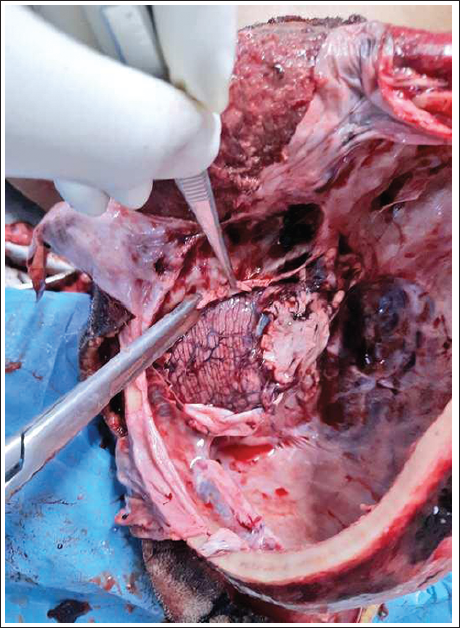
Through the craniotomy defect, the dura mater is examined. If the dura mater remains intact and covers the brain, it is carefully incised along the craniotomy wound margins, except at its inferior border, and gently reflected downward. The cerebral convexity is exposed, and the ipsilateral half of the brain is retracted outward at the sagittal fissure using a brain retractor. The falx cerebri and corpus callosum are then identified (Figure 3). The corpus callosum is incised along its length and depth in the midline, following the plane of the falx cerebri (Figure 4). A complete axial incision is made anterior to the concave notch of the tentorium cerebelli through the third ventricle, separating the cerebrum from the rest of the brain (Figure 5). This step can be facilitated by lifting the cerebral hemisphere with a spatula or retractor. The ipsilateral half of the brain is then carefully delivered by severing its attachments, such as cranial nerves.
Ipsilateral Half of the Brain Retracted Outward at the Sagittal Fissure to Visualize the Falx Cerebri and Corpus Callosum.

The Corpus Callosum Incised Along its Length and Depth in the Midline, Following the Plane of the Falx Cerebri.

An Axial Incision made Anterosuperior to the Concave Notch of the Tentorium Cerebelli Through the Third Ventricle to Separate the Second Half of the Cerebrum from the Brainstem and Cerebellum.
The next step involves incising the anterior and posterior attachments of the falx cerebri, reflecting it toward the now-vacant side, to allow for further examination of the contralateral brain. Additional incisions are made in the falx cerebri to release tension and facilitate the removal of the other half of the brain (Figure 6). With the previous axial incision having separated the cerebrum from the brainstem and cerebellum, the remaining half of the brain is easily delivered by severing any basal attachments (cranial nerves) with blunt-ended scissors. This is aided by tilting the head to the contralateral side and digitally manipulating the brain by inserting gloved fingers into the subdural space.
Reflection of the Falx Cerebri Away from the Remaining Half of the Cerebrum by Incising it at Multiple Points to Release Tension.
Once both cerebral hemispheres are removed, the tentorial attachment is incised along the petrous edges bilaterally to expose the cerebellum and brainstem (Figure 7). The spinal cord is transected as deeply as possible, and the brainstem–cerebellar complex is removed using conventional methods. The dura can then be stripped as usual, exposing the inner surface of the skull (Figure 8). Use of an external light source may assist in a more detailed examination.
Incision of the Tentorial Cerebelli Along the Petrous Edges Bilaterally to Expose the Cerebellum.
Exposure of the Inner Surface of the Skull by Stripping the Dura Mater.

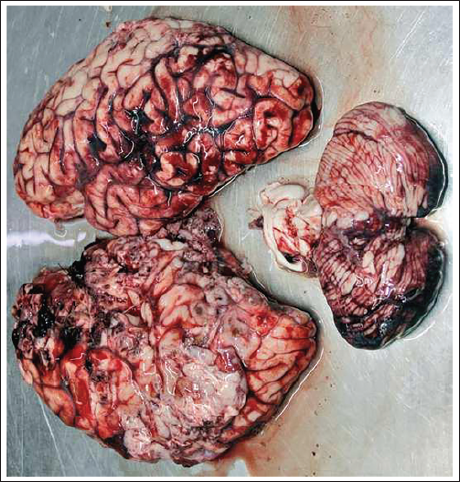
In this modified approach, the brain is removed in three distinct parts: (a) The right half of the cerebrum, (b) the left half of the cerebrum, and (c) the brainstem–cerebellar complex, all without the need for additional sawing. These parts can then be examined in a manner consistent with conventional autopsy methods (Figure 9).
The Whole Brain Removed in Three Distinctive Parts.
Limitations
Suitability for certain cases: This procedure is feasible only in cases where the brain’s firmness permits digital manipulation. In cases where the brain has already begun to putrefy, handling and removing the brain becomes significantly more challenging.
Risk of transecting the posterior aspect of the circle of Willis: During the separation of the cerebrum from other structures, there is a possibility of transecting the posterior aspect of the circle of Willis. However, in such cases, antemortem radiological investigations are usually available, which mitigates the impact of this limitation.36–41 Even if these structures are transected, they remain available for gross and histopathological examination.
Size of craniotomy defect: In some instances, the craniotomy defect may be too small to allow for the brain’s easy delivery. In such cases, greater digital manipulation or mechanical nibbling of the craniotomy wound margins may be required to complete the procedure.
Conclusion
The proposed method is particularly beneficial during situations involving highly infectious cases, where the spread of hazardous agents through aerosols poses a significant threat to the health of personnel working in mortuaries. In cases where a complete examination of the brain is essential, such as in highly sensitive autopsies, this technique offers a safer alternative. The novel procedure for brain removal through the craniotomy defect, without sawing the skull, minimizes the risk of aerosolization and potential exposure to infectious agents.
Given its utility, this method can be adopted not only in confirmed cases of highly infectious diseases but also in non-infectious autopsies. The rationale for broader application stems from the high number of asymptomatic cases of infectious diseases, which may go undetected during routine procedures. By incorporating this technique universally, forensic pathologists can ensure a higher level of safety, reducing the risk of inadvertent exposure to undiagnosed infections. Therefore, this method has the potential to become a standard practice in autopsy procedures, contributing to the overall safety of forensic pathology professionals while maintaining the integrity of the examination process.
Footnotes
Data Availability Statement
Not available publicly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.