
Abstract
An aneurysm is a localized dilation of a blood vessel or heart, with true aneurysms involving all three layers of the arterial wall. DeBakey Type III thoracic aortic dissection (DBTTCAD) is a fatal condition, commonly associated with chronic hypertension, which weakens the aortic wall. In this case, a heated quarrel triggered the sudden rupture of a pre-existing aneurysm, causing immediate death. Factors such as stress, physical exertion, or collapse can precipitate such fatal events. Five individuals involved in the altercation were charged with murder. Autopsy and microscopic examination were crucial in determining the cause of death, highlighting the forensic importance of sudden deaths during violent encounters.
Introduction
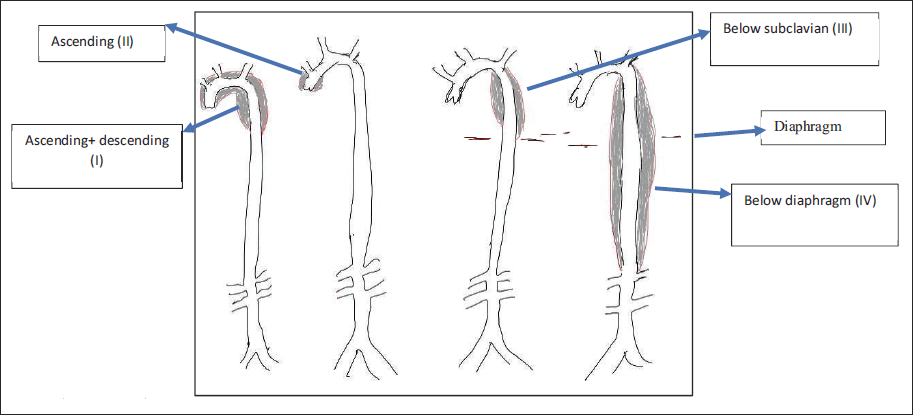
DeBakey Type III aortic dissection originates distal to the subclavian artery in the descending aorta and is further subdivided into IIIa that extends distally to the diaphragm and IIIb that extends beyond the diaphragm into the abdominal aorta 1 (Figure 1). An aneurysm is a localized dilatation of the lumen of the blood vessel or heart, which may be congenital or acquired, single or multiple. A true aneurysm involves all three layers of the arterial wall. We reviewed the literature and found not a single case reports of DeBakey Type III thoracic complete aortic dissection (DBTTCAD). Hypertension is a major risk factor for aortic dissection. 2 Aortic dissection occurs when blood separates the laminar planes of the media to form a blood-filled channel within the aortic wall. 3 Thoracic aortic dissection (TAD) is an emergency procedure. Approximately 22% of the patients with TAD do not reach the hospital. 4
DeBakey Classification of Aortic Dissection (Mentioned as I–IV).
Case History
A 58-year-old male presented with a history of fighting and intense arguments with others. The deceased fell down on the ground and immediately rushed to the hospital, and the clinician declared them dead. There was an alleged allegation of murder by the beatings. The deceased was sent to the mortuary for an autopsy examination by an investigating agency. The deceased had been taking hypertensive medicine for the last five years. The history of cardiac disease and coronary artery bypass grafting (CABG) was done two years ago.
Observations
Multiple whitish areas were observed over the pericardium. The circumference of the aortic valve was 06 cm, and numerous yellow plaques were observed in the ascending aortic wall. The coronary arteries exhibited narrowing of their lumens, which appeared gritty upon cutting. Stainless steel stents were found in the LCA (left coronary artery) and LAD (left anterior descending artery) walls.
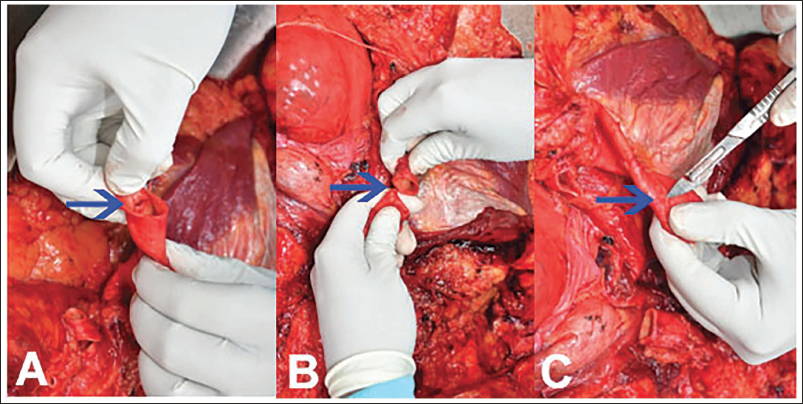
The descending aorta was ruptured and was completely separated 10 cm below the origin of the left subclavian artery (Figure 2A). Near the edges of the transection, the tunica intima of the aorta is stripped and attached in situ (Figure 2B). No other internal or external injuries were observed over the body. The descending aorta had multiple small aneurysms, with the largest measuring 0.5 cm in diameter (Figure 2C).
(A) Tearing of Aortic Wall. (B) Complete Dissection of the Thoracic Aortic Wall with Stripped Wall. (C) Multiple Aneurismal Aortic Walls.
Histopathological Observations
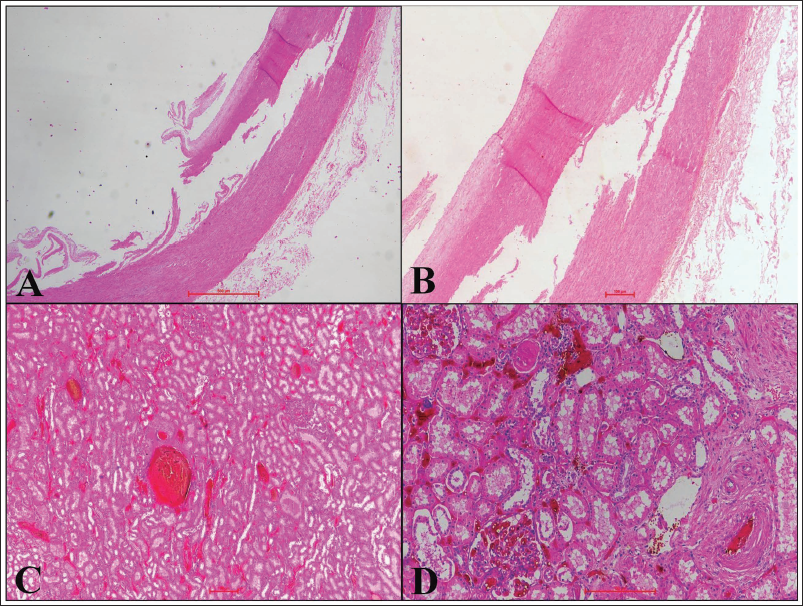
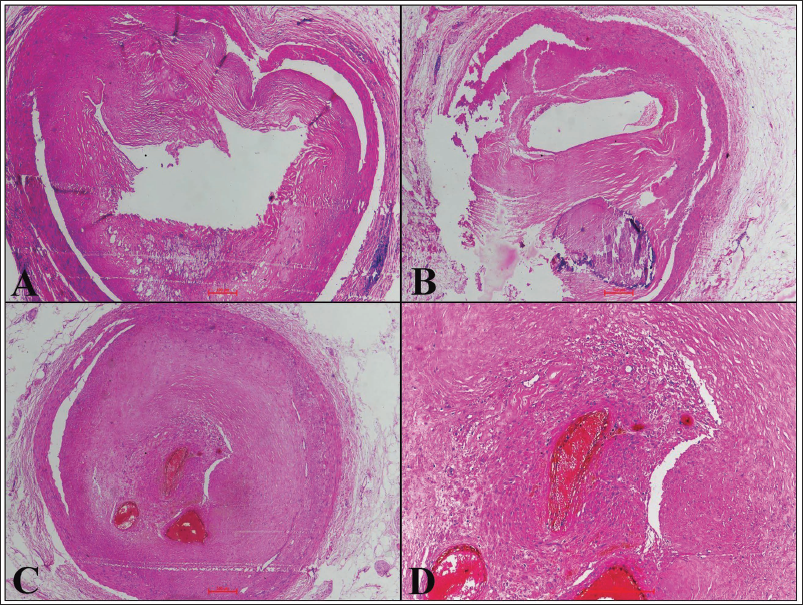
The thoracic aorta showed aortic dissection as a tear site in the tunica intima, and the tunica media was completely torn (Figure 3A and B). Each kidney showed focal glomerular sclerosis, thyroidization of tubules, hyalinized and thickened blood vessels, chronic inflammatory cell infiltration, and interstitial fibrosis (Figure 3C and D) Several atheromatous plaques were found in the LCA (Figure 4A), LAD (Figure 4B), and right coronary artery (RCA) (Figure 4C and D) along with thrombosis with the feature of recanalization. The anterior, posterior, and lateral walls of the left ventricle and the posterior wall of the right ventricle showed fibrosis.
(A) Large-size Blood Vessels Showing Tears in Tunica Intima and Media (Hematoxylin and Eosin (H&E); 4×), (B) Complete Dissection of Tunica Media (H&E; 10×), (C and D) Renal Parenchyma Shows Markedly Congested Blood Vessels, with Renal Vasculature Exhibiting Concentric Thickening of the Vessel Wall with Minimal Cellularity (H&E; 4× &10× Respectively).
(A) LCA Showing Atheroma (H&E; 4×). (B) RCA Showing the Presence of Fibro Atheromatous Plaque with the Presence of Calcification (H&E; 10×). (C) RCA Showing Near Complete Occlusion of the Lumen (H&E; 4×). (D) RCA Showing Recanalization (H&E; 10×).
Discussion
Aneurysm formation owing to atherosclerotic changes induces pressure or ischemic atrophy of the underlying media, resulting in elastic tissue loss, wall weakness, or rupture. Weakening of the tunica media predisposes the patient to an intimal tear, resulting in an intramural hematoma that cleaves the media layers, leading to aortic dissection.3, 4 Herein, we report a case of complete TAD. Hypertensive changes in the kidneys were seen as (Figure 4). The evidence of atherosclerotic changes with coronary artery intervention in the form of percutaneous coronary interventions in both the LCA and left anterior descending arteries was present. No other external or internal injury observed during autopsy.
Intimal tears occur in the ascending aorta 65% of the time, the descending aorta 25%, and the arch or abdominal aorta 10%. 3 One study found that chronic hypertension accounted for 49% of ischemic heart disease cases. 5 Formation of aortic aneurysms is nine times more frequent in the abdominal aorta than in the thoracic segment. 6 An autopsy revealed a massive left hemothorax and a tear in the descending aortic aneurysm. Microscopic examination confirmed complicated atherosclerosis in the descending thoracic aorta. Autopsies, clinical presentations, and treatment histories aid in the diagnosis. 5
Evidence of CABG was present, indicating a prior surgical intervention to restore blood flow in occluded coronary arteries. Hypertensive changes were observed in the vertebral and basilar arteries, characterized by the presence of atheromatous plaques. Chronic hypertension leads to structural alterations in cerebral arteries, which impair cerebral perfusion. These hypertensive changes result in a reduced arterial lumen and an increased wall-to-lumen ratio.7–10 The kidney shows evidence of focal segmental glomerular sclerosis, consistent with chronic hypertensive injury. Additional findings include thyroidization of the tubules, thickening and hyalinization of blood vessels, chronic inflammatory infiltrates, and interstitial fibrosis. 11 Hypertensive changes in the kidney were seen in microscopic examination. Upon autopsy, no signs of mechanical injury were found, either internally or externally. The cause of death was opined to be due to pathological complete thoracic aortic dissection. An autopsy examination ruled out the possibility of foul play in the murder case.
Conclusion
DBTTCAD is commonly associated with hypertension and aneurysmal dilation, both of which contribute to the development and progression of the dissection. Complete rupture of the thoracic aorta is fatal and may cause sudden death. Triggers include emotional stress, aneurysm rupture, sudden falls, or collapse. Such cases may raise medicolegal concerns, including the possibility of foul play. Autopsy and microscopic examination are hallmarks of opinion in cases of DBTTCAD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained for the study.