
Abstract
Bee stings are the most common among insect emergencies. Bee venom contains dopamine, histamine, neurotoxin enzymes, melittin, hyaluronidase, and phospholipase-A. Hypersensitivity varies from mild urticaria to severe anaphylaxis leading to even death. We report a case of a 72-year-old man attacked by a swarm of bee and sustained multiple bee stings all over his face, head, neck, chest, and both arms causing massive envenomation following which he managed to walk home following which he developed systemic symptoms such as vomiting, weakness, fatigue, dizziness, gasping, and chest pain. He was brought dead to the casualty and hence was taken up for medicolegal autopsy. Postmortem examination revealed congestion of all internal organs including classical signs of anaphylaxis leading to respiratory distress and death. Multiple bee stings envenomation can end up in anaphylactic shock and death. Therefore, patients who have sustained multiple bee stings have to be rushed to the hospitals at the earliest and receive prompt treatment to avoid fatal complications. Purpose of this article is to highlight the symptomatology and gross changes noted in the autopsy are signs of anaphylaxis as a result of allergy to honeybee venom.
List of Abbreviations
ACTH—adrenocorticotropic hormone, IgE—immunoglobulin E, PLA2—phospholipase-A2, RAST—Radio allergo sorbent test.
Background
Insects that sting to defend their colonies are included in the order Hymenoptera in the taxonomy of animals. Notable Hymenoptera groups in medicine are the Apoidea (bees), Vespoidea (wasps, hornets, and yellow jackets), and Formicidae (ants). A bee sting is a wound and discomfort brought on by a bee stinger puncturing skin. In contrast to insect bites, bee stings are caused by venom that varies greatly in composition. Bee sting casualties are the commonest among insect sting/ bite emergencies.
From 2000 to 2017, hornet, wasp, and bee stings resulted in 1,109 deaths among US citizens, or an average of 62 deaths each year. The number of deaths varied, peaking at 89 in 2017 and falling to 43 in 2001. 1 Bees are typically 10–15 mm long, with a barbed sting, and brilliant yellow bodies with black markings on the abdomen. While wasps and hornets can sting repeatedly, bees can sting only once since their sting becomes embedded in the flesh. 2 The bee sting apparatus consists of three functionally independent parts: the motor part, the piercing part, and the venom-related area. 3 Honeybee venom contains dopamine, histamine, neurotoxin enzymes, melittin, hyaluronidase, and phospholipase-A. 4 The severity of reactions to bee sting hypersensitivity can vary from mild skin rashes/hives to fatal anaphylaxis leading to death. Anaphylactic reactions can happen instantly or within 20 minutes. There is breathing difficulty, dizziness, and unconsciousness. The number of stings has a direct bearing on the severity and outcome of the envenomation. Consequently, 50–500 stings can result in an adult man dying. 5 In 2–15 minutes, death could happen.
Case Presentation
A 71-year-old man, who was returning from his friend’s funeral, was attacked by a swarm of bees on 25 September 2022 at 8
External Examination
On the autopsy table, the length of the victim measured 160 cm; he was moderately built and nourished. Rigor mortis had developed over the upper part of the body. Postmortem staining was present over the back of the body and was not fixed. Multiple bee stings were present over the scalp, face, both arms, and forearms, front of the chest, outer aspect of both sides of chest, and below axilla, in total accounting for 106 bee sting injuries with a surrounding zone of inflammation around each sting (Figures 1–3). Thirty-six dead honeybees were collected from the body of the victim, from the scalp hair, within pockets, folding of full sleeve cuffs, within his tank and shirt, from nostril and mustache.
Dead Honeybee Recovered from the Dead Body.
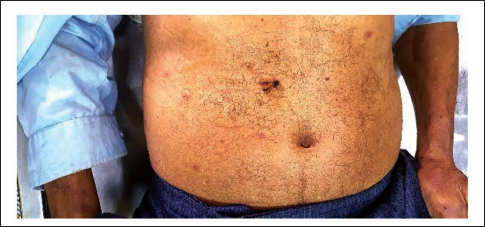
Bee Stings Struck in Skin of Face.

Removed Stingers.

Internal Examination
Autopsy examination revealed certain findings suggestive of anaphylactic reactions. Few honeybees were removed from the laryngeal lumen. Grossly larynx and trachea were intact, edematous, and congested, with obstruction of the laryngeal lumen (Figure 4), which was in concordance with a case report by Sethi and Jena.
6
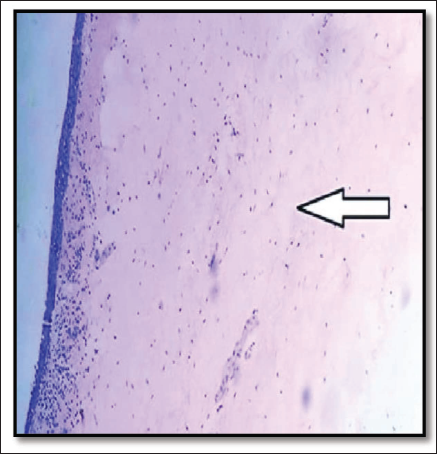
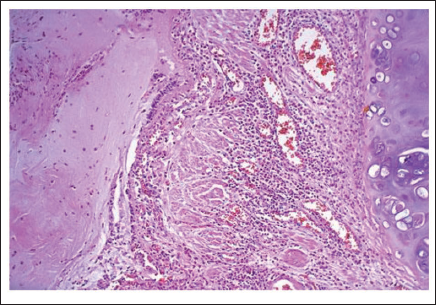
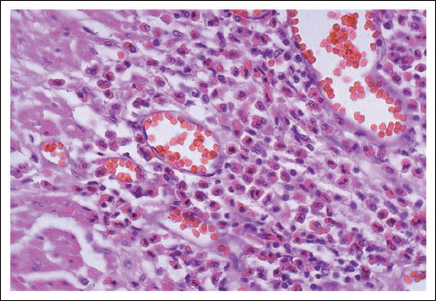
Histopathology of the larynx confirmed the same (Figure 5). Both lungs—Hyper expansion of the lungs and mucus clogging was present, which went in favor of asthmatic crisis. Anaphylactic asthma fatality—Lungs were heavy and diffusely congested on cut section. Blood with copious froth exuded on compression (right—511g, left—436 g) (Figure 6). The bronchial lumen was filled with mucus (Figure 7) and at high magnification, the numerous eosinophils were prominent (Figure 8). Chronic congestive splenomegaly was incidentally found even with neither any past medical history/condition nor with history of any addictions.
Gross Laryngeal Edema and Congestion.

Histology of Laryngeal Edema.
Heavy and Diffusely Congested Lungs with Mucous Plugs.

Microscopy of Bronchial Lumen.
Microscopy of Bronchial Lumen at High Magnification.
Anaphylactic shock from numerous bee stings was determined to be the cause of death based on the results of the postmortem examination and the histology report.
Discussion
Honeybee venom, enzymes (hyaluronidase, phospholipases), and biological amines (norepinephrine, serotonin, dopamine, histamine, and acetylcholine) are just a couple of the chemicals that make up stings and lead to the clinical picture. 7
A honeybee sting can present in either or all of the four modes of presentations as follows. Dermal reaction symptoms (urticaria, erythema, and angioedema), cardiovascular (acute coronary syndrome, hypotension, and shock), respiratory system effects (laryngeal edema and bronchospasm), and events involving the digestive system (vomiting and incontinence). 5
The melittin protein, which hydrolyzes cell membranes, modifies cell permeability, and releases histamine, is the primary cause of localized discomfort. Additionally, it releases catecholamines and in concert with phospholipase-A2 (PLA2), it facilitates intravascular hemolysis. Histamine and other vasoactive peptides are released from mast cells by the mast cell degranulating peptide (peptide 401). PLA2, which together with melittin causes intravascular hemolysis, is bee venom’s primary allergenic element. Another is hyaluronidase, which is thought to be the main “spreading factor” since it alters cell membranes. Additionally allergic is hyaluronidase and vasoactive amines, such as dopamine, noradrenaline, and histamine. 8
Management Considerations
In case of attack by a swarm of bees, the treatment should be immediately started without any delay, which includes ligature above the site of the sting, removal of the stinger and venom sac with a blade, or with a forceps, following the administration of the lifesaving drug, that is, an intramuscular shot of adrenaline also known as epinephrine. 9 Delivery of adrenaline must not be delayed by even a few minutes to prevent hypoxia or death. This can be followed by all the other first aid measures such as iodine or local antihistamine and local ice application, and adrenocorticotropic hormone (ACTH) 25 mg in a liter of normal saline can be given by intravenous infusion. 10
If there are pertinent clinical or postmortem signs, serum tryptase values of more than 100 µg/L in a postmortem sample would be compatible with anaphylaxis being the cause of death or contributing to it. 11
In addition to routine toxicological screening, serum should be submitted for radio allergo sorbent test (RAST) testing for serum tryptase level and immunoglobulin E (IgE) specific to bee venom. 12 These simple, low-cost tests might be able to rule out anaphylaxis as the cause of death.
In case of suspicion, a scene investigation has to be done to know whether the victim has used any strong scents, and wearing brightly colored clothing may make it easier for insects to find them. The presence of any biological or inorganic stains or trails must be noted and sampled. Interviews with parents, relatives, and other witnesses are required at all times. The location, month, and time of year at the moment of death must be taken into consideration, and they must be contrasted with the local geographic latitude’s pollen calendar. 11
Mass envenomation-related deaths are thought to be caused by three main processes: direct venom toxic consequences, intravascular hemolysis mediated by melittin and PLA2, and significant hypotension resulting from excessive histamine release. 13
Particularly in cases when there are no visible stings, a serum tryptase and specific IgE to bee venom on serum taken at autopsy might help identify anaphylactic reaction to bee venom as the cause of death. 10 Such testing and investigation were not done in our case, since multiple bee sting injuries, autopsy findings, and the cause of death were evident.
Parenteral antihistamines, fluid resuscitation, bronchodilators, supplemental oxygen, intubation, vasopressors, tetanus booster, and pain relievers may be required. Patients should be observed for 24 hours for recurrent anaphylaxis. Rarely, symptoms of bee stings include vasculitis, rhabdomyolysis, widespread alveolar hemorrhage, and thrombocytopenic purpura. The case in point showed the signs of itching, urticaria, hypotension and shock, nausea, vomiting, laryngeal edema; that is, the symptoms included involvement of all the above-mentioned systems. Deaths due to bee sting are quite avoidable deaths with prompt action. Immediate resuscitation and care would have saved the patient if he would have been ushered to the casualty.
Conclusions
Therefore, this article highlights the clinical manifestations and fatal outcomes of mass honeybee envenomation including the autopsy findings of anaphylaxis to bee venom and the need for initiating immediate resuscitation by anticipating the unwanted fatal outcomes including death.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval has been obtained for the conductance of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained for the conductance of the study.