
Abstract
Corona virus disease pandemic of 2019 gained peak in India in early 2020 causing exhaustion of health care system which after mitigation again emerged in later march 2021 called second wave. Lot of literature published regarding difference strain, virulence, risk factors etc in between first and second wave. Therefore, a comparative study of demographic profile of COVID deaths in first and second wave conducted at AIIMS, Patna. The study included a total of 1470 deaths, of which 912 were from the first wave and 458 from the second. The age group over 60 years old saw the highest number of deaths. 51.3% in the first wave and 42.7% in the second. Of the female deaths in the first wave, 21.06% occurred in the first wave, and 28.39% in the second wave. Rural region infection dropped from 50.66% in the first wave to 37.33%.
Introduction
Since early 2020, the coronavirus disease pandemic of 2019, the chaos and destruction it has caused both scientific and social realms have been largely influenced by the ongoing pandemic. As we entered the latter part of 2021, the number of reported global infection cases surpassed 173 million, with over 37 lakh deaths attributable to the illness. 1
It is inconceivable the damage done to people’s economies, way of life, and mental health. India was successful in fighting COVID throughout 2020 with bravery. A rigorous lockdown combined with a proactive approach allowed our country to lessen the harm. India asserted that, despite having an exceptionally large number of patients, it possessed the lowest mortality rate and the highest rate of recovery compared to other major global powers. 2
The best news came at the beginning of 2021 when the greatest immunization campaign was initiated and two locally made vaccines were approved. 3 By January or February, the struggle against corona appeared to be almost over; the number of average daily cases dropped from a peak of 96,000 in September to just 12,000, and the number of daily fatalities dropped below 100.4, 5
Social, cultural, and economic activities were gradually reverting to their pre-pandemic conditions as the restrictions and lockdown measures were eased. Experts continued to issue warnings regarding the possibility of a second wave, the virus’s DNA mutation, the need to continue taking precautions, and how to behave in a COVID-aware manner. Expert and governmental communication appears to be ignored. In March 2021, there was a noticeable increase in daily case numbers, indicating the commencement of the second wave. 6
By the end of April, India had broken all previous records for the number of daily cases and fatalities reported in a single country, with over 4,00,000 cases reported daily. 7 The health system as a whole fell apart. Images of the country without oxygen, hospital beds, drugs, and even cremation areas would remain in people’s thoughts for many years to come. These scenarios demonstrate that the second wave was far bigger in scale than the first wave, but there was a dearth of information regarding demographic traits such as sex, age, and the disparity between rural and urban areas.
Aim of the Study
To compare the demographic profile of COVID-19 deaths, between the first and second waves of the disease, at AIIMS Patna.
Objective of the Study
To identify the prominent age groups of people who have died because of the COVID-19 disease, first wave, and those who are dying because of the COVID-19 disease, second wave.
To identify the prominent sex group, those who were and are more prone to mortality in COVID-19 disease, first wave and second wave, respectively.
To evaluate common co-morbidities, which were and are associated with the COVID-19 first wave and second wave mortality, respectively?
To compare the prominent age groups from Mortality rates during the initial and second waves of the COVID-19 pandemic.
To compare the prominent sex groups from Mortality rates during the initial and second waves of the COVID-19 pandemic.
To compare the common co-morbidities from Mortality rates during the initial and second waves of the COVID-19 pandemic.
Materials and Methods
This study, which was conducted at All India Institute of Medical Sciences, Patna, Bihar, India, was cross-sectional in nature. The hospital records at the mortuary, of the Department of Forensic Medicine and Toxicology, and the Medical Record Department at AIIMS, Patna, served as the study’s primary source of COVID-19-related data. The analysis of secondary data from records kept at the mortuary served as the foundation for the study. For the goal of retrieving the data and using it only for research, written consent was obtained. The first wave of COVID-19 was thought to have occurred between March 30, 2020, and March 3, 2021 (or until the data were obtained). The period believed to encompass the second surge of COVID-19 is considered to have taken place from March 9, 2021 to March 19, 2022.
In the first wave, there were a total of 912 reported fatalities and 458 deaths were reported during the second. For the categorical variables, a univariate Chi-square test was run in addition to the computation of mean, median, and percentages. The research utilized logistic regression analysis to investigate the standalone relationship between various factors and the mortality of individuals with COVID-19. Subsequently, these data were incorporated into a Microsoft Excel spreadsheet. Statistical analyses were conducted using the latest version, SPSS 20.0, and significance was determined at a 95% confidence level, considering a P value below .05 as statistically significant.
Results
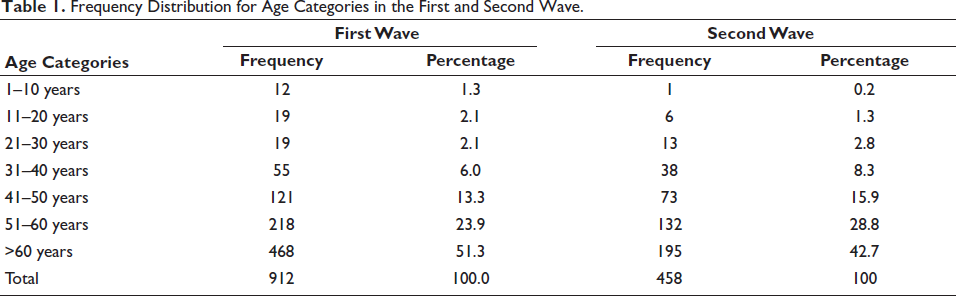
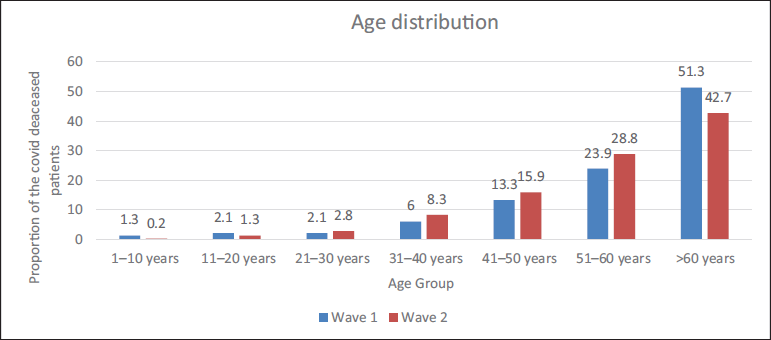
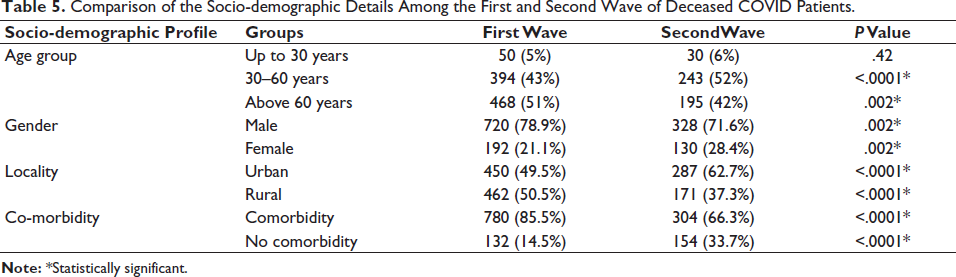
The analysis includes 1,470 COVID-19 deaths in total. During the first wave, the average age of those who passed away was 58.80 (±15.90) years, whereas in the second wave, it was 57.65 (±14.72) years. With 51.30% of all deaths, the age group over 60 was the most severely affected. The order of most affected age groups in both waves remained consistent, with those above 60 being the most severely affected, followed by the 51–60 age group, and then the 41–50 age group. Throughout both waves, fatalities in the 0–20 age range remained the least prevalent (Table 1, Figure 1).
Frequency Distribution for Age Categories in the First and Second Wave.
Age Distribution of the Deceased in the First and Second COVID Waves.
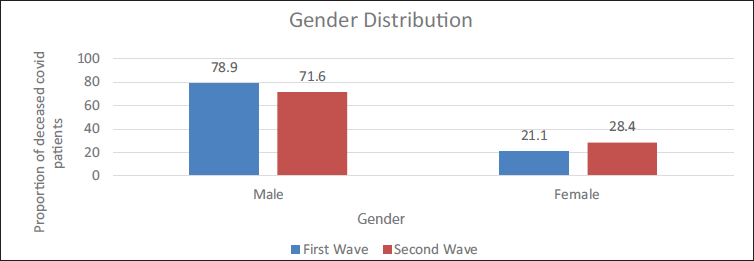
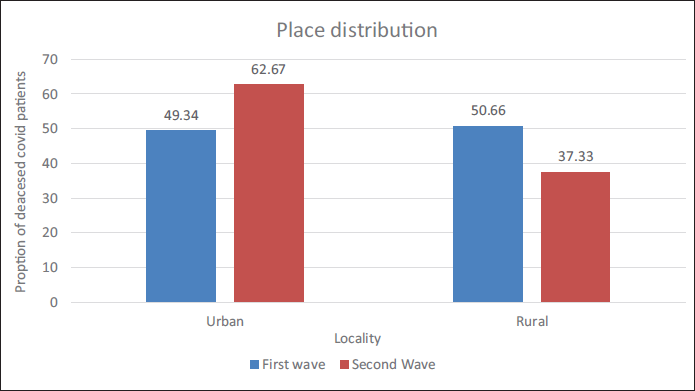
At AIIMS, Patna, the number of male deaths from the COVID-19 pandemic was reported to be more than 720 (78.94%) in the first wave and 328 (71.61%) in the second. In the second wave, the number of female deaths rose by 7% over the first (Figure 2). In the initial wave, rural regions constituted 50.66% of the fatalities. In the subsequent wave, urban fatalities witnessed a 1.27-fold rise compared to the first wave (Table 2, Figure 3).
Locality-wise Distribution of the Deceased COVID Patients.

Gender Distribution of the Deceased COVID Patients in the First and Second Wave.
Place Distribution of the Deceased in the First Wave and the Second COVID Wave.
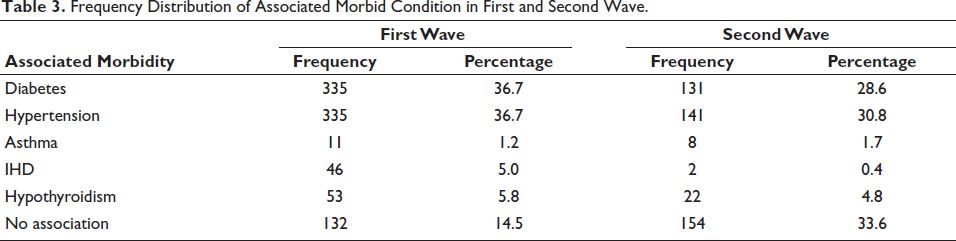
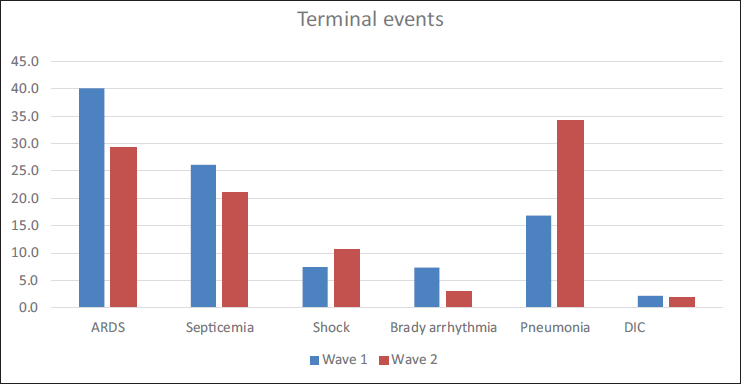
The most common connected morbid disorders in the second COVID wave were hypertension (30.8%) and diabetes (28.6%), with hypertension accounting for 36.7% of all related morbid conditions in the first wave (Table 3). Whereas, the most frequent fatal events in the first wave of COVID were ARDS and septicemia, while the most common fatal event in the second wave of COVID was pneumonia (Table 4, Figure 4).
Frequency Distribution of Associated Morbid Condition in First and Second Wave.
Terminal Events on the Deceased in the First Wave and the Second COVID Wave.
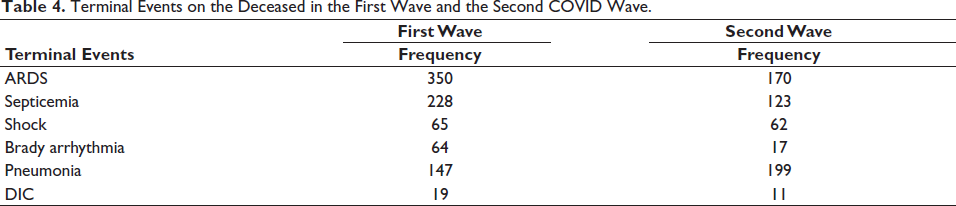
Terminal Events on the Deceased COVID Patients.
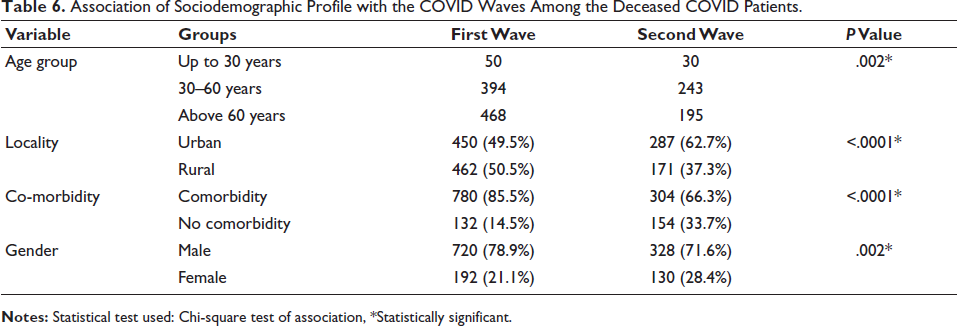
When examining the sociodemographic characteristics of patients who passed away during the initial and subsequent waves, a noteworthy variation was noted in the distribution of gender, locality, and the correlation of comorbidities between the two periods, indicated by a
Comparison of the Socio-demographic Details Among the First and Second Wave of Deceased COVID Patients.
Association of Sociodemographic Profile with the COVID Waves Among the Deceased COVID Patients.
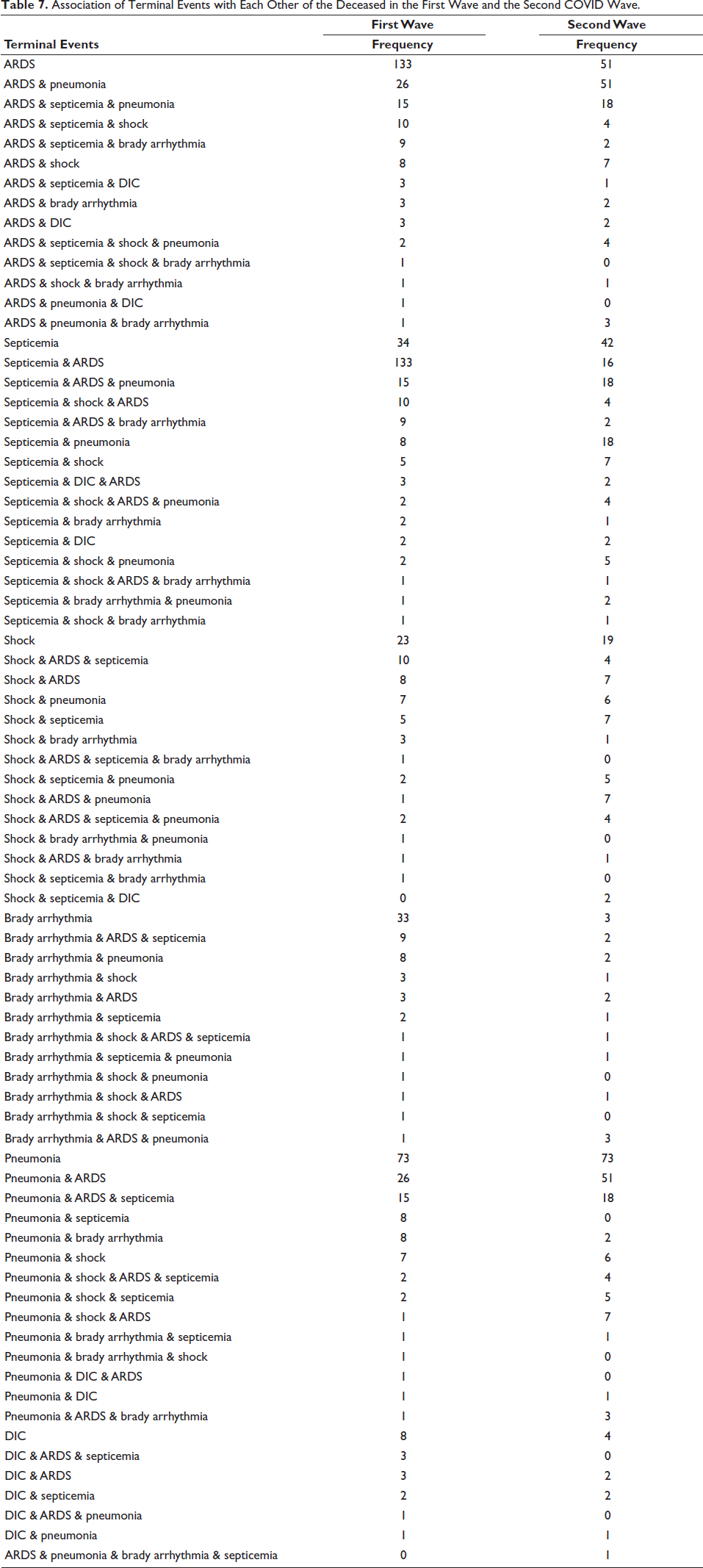
But there are also other co-morbidities that are noted; some of these were present alone, but most of them were in conjunction with other co-morbidities that are included in the table (Table 7).
Association of Terminal Events with Each Other of the Deceased in the First Wave and the Second COVID Wave.
Discussion
The initial confirmed fatality from COVID-19 at AIIMS Patna occurred on March 30, 2020, and by May 17, 2021, the cumulative death toll had reached 506. This study examines the demographic attributes of COVID-19 fatalities and the response to the two waves of the virus in Patna, Bihar from 2020 to 2021. The aim is to provide insights for future epidemic prevention and control measures and to assist general practitioners and family doctors in improving their adaptive strategies for various aspects of COVID-19. 8 The analysis includes a comparison of the total number of COVID-related deaths in the first and second waves. Looking at the total number of COVID-related deaths during the first and second waves, more deaths were reported in the first wave of COVID than the second, which is different from other states of India, where the second wave is far more aggressive and has around twice as many cases as the first wave. The percentage distribution of COVID-19-related deaths across different age groups was found to be relatively consistent during both waves. Mean age of the deceased was 58.80 (±15.90) years in first wave and 57.65 (±14.72) years in second wave. Contrary to popular belief, which holds that the second wave of infection affected younger people and the first wave slightly older people. The distribution of COVID-related deaths in Patna district aligns with national trends, with the highest percentage occurring in individuals over 60 years old. The percentage decreases progressively in each younger age group. Similarly, during the second wave, there was a parallel pattern in the distribution of cases based on gender, indicating that more males succumbed to the virus compared to females. This aligns with Peckham H. et al.’s research, which identified a male bias in COVID-19 mortality. They attributed this bias to a weaker immune response in males, citing higher levels of CD4+T cells, CD8+T cells, B-cells, and type 1 interferon (IFN) in females. The antiviral nature of interferon is linked to the number of X chromosomes, providing females with an additional defense against COVID-19. Additionally, the benefits of estradiol include enhancing immune cell production, proving valuable in combating SARS-CoV-2. Sociocultural factors are implicated in gender-based COVID-19 mortality differences, as men tend to engage in riskier behaviors like frequenting crowded places, inadequate hand hygiene, and habits, such as smoking and alcohol consumption. These behaviors contribute to an elevated risk of comorbidities, influencing the overall fatality rate in COVID-19. 9 There is a noticeable increase of 7.3% in the number of female fatalities between the initial and subsequent waves. Additionally, women tend to take on greater responsibilities in family and domestic tasks, becoming the primary caregivers for those affected by COVID-19 within their households. This shift is particularly pronounced due to the breakdown of the healthcare system, especially affecting children and the elderly, and has been further accentuated during periods of confinement.10, 11 The patterns of COVID-related deaths in Patna exhibit variations between urban and rural areas, contrasting with trends observed in other parts of India. In the initial wave, more deaths were reported in rural regions than urban areas. However, during the second wave, the situation reversed, with a higher concentration of fatalities occurring in urban areas. This shift may be attributed to factors like population density, crowded transportation infrastructures, and gatherings in educational, shopping, and healthcare facilities in urban settings, which contribute to increased virus transmission. 12 But most of the rural population of Bihar, working outside Bihar as a daily laborer, and they came back to the rural area from metropolitan cities, which were the epicenter of corona at that time, might lead to higher deaths in the first wave from a rural area. The increase in testing capacity and evolving testing criteria led to a surge in the number of cases, causing hospitals to become overcrowded and the medical system to enter a crisis. The anguish of a low doctor to patient ratio was made worse by the growing burden of patients. The doctors working in hospitals responsible for COVID-19 patients were required not only to promptly handle the challenges associated with COVID-19 medical issues but also to swiftly provide guidance on managing suspected COVID-19 cases and establish effective institutional protocols for addressing the pandemic. 13 During the second wave, a noteworthy discovery in this research is that the proportion of deaths increased among individuals aged 31–60, whereas in the initial wave, a greater percentage of fatalities occurred in the 61–90 age bracket. This demonstrates unequivocally that the younger age group experienced relatively higher mortality during the second wave. Likewise, in Spain, there was a significantly higher percentage of youthful fatalities in the second wave. 14
Surprisingly, despite the increasing number of verified cases, the second wave did not see as many deaths overall. In fact, fewer people died overall during the second wave than during the first, many recommendations for prompt diagnosis and treatment have been associated with the observed decrease in mortality levels during the second wave, as indicated by studies conducted globally.12, 15, 16 The extensive utilization of corticosteroids emerged as a transformative factor in reducing mortality rates. 16 Males outnumbered females in the distribution of mortality by gender in both waves, and in our study, also the mortality rate is around three times higher in males in both waves. According to the Global Health 50/50 study, men experience more severe COVID-19 cases and more fatalities due to a variety of causes. 17 First, there are biological distinctions: men typically have a weaker immune system than women, which may account for their greater vulnerability to infection. 18 Second, males are inclined to be more vulnerable to various long-term health issues associated with COVID-19, such as persistent respiratory conditions. Additionally, men have a higher likelihood of engaging in excessive smoking and alcohol consumption, both of which are connected to chronic illnesses. 17 In Barcelona, men saw higher excess death rates during the two waves. 19 In this study, it was found that the overall mortality had decreased in the second wave, but had a higher mortality ratio in an urban area in comparison to the first wave, in which the rural population had more mortality in comparison to the urban. Guihong Fan et al. proposed that the reduced-case fatality rate (CFR) in the second wave may be explained by factors including the harvest effect, improved testing capabilities, the age distribution among the infected population, heightened virus transmissibility in young, healthy adults and children, and favorable environmental conditions. 20 In the early phases of the pandemic, the predominant circulating virus strain was the original SARS-CoV-2 strain that originated in Wuhan, China. While some mutations occurred during the first wave, they were relatively limited in number and impact on the virus’s properties. The D614G mutation, for example, became prevalent and was associated with increased viral transmissibility. In the course of the second surge, numerous fresh strains of the SARS-CoV-2 virus surfaced. Among the noteworthy variants were the Alpha variant (B.1.1.7), initially detected in the United Kingdom, the Beta variant (B.1.351), first identified in South Africa, the Gamma variant (P.1), initially observed in Brazil, and the Delta variant (B.1.617.2), first recognized in India. 21 In our study, we observed a higher number of fatalities among individuals without pre-existing conditions during the second wave as opposed to the first wave. Specifically, during the first wave, only 14.6% (134) of the deceased had no co-morbidities, while in the second wave, 154 individuals (33.4%) who succumbed to the virus had no underlying health issues. This suggests a heightened virulence of the virus in the second wave, possibly attributable to mutations.
Conclusion
The world is currently experiencing an unprecedented situation that previous generations have not encountered. The virus responsible for this situation is continually changing, and as a result, our understanding of its characteristics and the measures to control it must evolve accordingly. Given that prolonged lockdowns are not sustainable, it is essential to adopt a data-driven approach to suppress transmission, prevent severe illness and fatalities from COVID-19, and minimize the social and economic impact of the pandemic.
This study suggests implementing more rigorous measures in response to a surge in cases, avoiding premature relaxation of interventions, and ensuring public awareness of the strict enforcement of COVID-appropriate behaviors (CAB). Additionally, it emphasizes the need to consider the impact of climatic variables on disease transmission in prevention and mitigation strategies. Furthermore, the study recommends involving primary care physicians in both planning and action for this emerging pandemic, tailoring policies to the specific needs of different regions.
Key Points
The average age of deaths related to COVID was comparable in the first and second waves. However, the second wave witnessed a higher number of fatalities in the younger age group compared to the first wave.
Although more males succumbed to COVID in both waves, there was a 7% increase in female COVID-related deaths during the second wave.
In the first wave, a greater proportion of COVID-related deaths occurred in rural areas, but the second wave experienced a reduction in such deaths among the rural population.
The second wave highlighted a lack of predictability and preparedness in dealing with the challenges posed by the pandemic.
Most of the deaths in the first wave were associated with comorbidities, whereas deaths in the second wave had less correlation to comorbidities due to increased virulence, which may be caused by mutations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study approved by Institutional Ethics Committee reference no AIIMS/Pat/IEC/ 2020/ 741 dated 10/ 07/ 2021.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
As this study is document bases retrospective study not revealing identity of the deceased therefore informed consent not required.