
Abstract
Due to the unprecedented and repeated outbreak of the coronavirus pandemic and its highly contagious nature, social life of people of every strata of society across the globe considerably affected both economically as well as mentally. The pandemic affected the people most who earn their subsistence on a daily basis, working in the unorganised sector, patients suffering from co-morbidity, who need regular check-ups, as the government imposed lockdown and restricted the movement of people to check the spread of COVID-19. Despite the low fatality rate, the coronavirus created havoc among the people mainly due to inadequate medical infrastructure such as shortage of ICU beds, ventilators, lifesaving oxygen, medical staff and much more. The COVID-19 pandemic has raised challenges in the handling of the deceased of suspected or confirmed cases due to lack of knowledge and research. There is a lot of speculation among forensic medicine experts regarding post-mortem examination and management of the dead body after post-mortem examination of COVID-19 suspected or confirmed cases. The authors have conducted a research study based on a questionnaire to assess the knowledge & attitude of forensic medicine experts regarding post-mortem examination and management of COVID-19 dead body (suspected/confirmed).
Introduction
COVID-19 pandemic, also known as coronavirus pandemic, was a pandemic of coronavirus disease started in 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The virus was first identified from an outbreak in the Chinese city of Wuhan in December 2019, and attempts to contain it were failed, allowing it to spread globally. World Health Organisation (WHO) declared a Public Health Emergency of International Concern on 30 January 2020 and a pandemic on 11 March 2020. As of 21 January 2022, pandemic had caused more than 342 million cases and 5.57 million deaths, making it one of deadliest virus infections in history. 1
Post-mortem examinations are considered gold standard for establishing cause of death and role of pre-existing diseases & SARS-CoV-2 infection in cause of death. 2
On 22 April 2020, upon outbreak of COVID-19, more than 60 pathologists and technicians assembled as the COVID-19 Pathology Team in Wuhan & Chongqing (China) conducted PM examination in 37 cases and in addition, percutaneous multiple-organ biopsy was carried out in 54 cases. The PM discloses visible damage in lungs and immune organs of COVID-19 patients. Since few immune organs are SARS-CoV-2 positive with spleen atrophy, immune organs may be another target organ of virus infection in addition to lungs, which emphasises that clinical management should consider damage to the immune system also. We found that most of the deceased COVID-19 cases had mucous plugs in alveoli and deep small airways, which might severely affect ventilation. Mechanism of infection, course & prevention measures are subject of further investigation. In COVID-19 patients, pulmonary fibrosis occurred early & diffusely, suggesting a requirement for early measures on pulmonary fibrosis. In addition, hyperplasia of pulmonary epithelial cells & elevation of plasma carcinoembryonic antigen (CEA) in some patients also require studies on cause and follow-up. In some deceased cases, nasopharyngeal swab test showed negative viral nucleic acid, but positive in other organs, suggesting that current standard swab test for COVID-19 as an indicator for clinical cure & hospital discharge may not be adequate. Detection of nucleic acids of SARS-CoV-2 virus in multiple organs of patients implies that existence of SARS-CoV-2 and related organ damage might persist throughout disease course even in patients with a longer term of disease. Preliminary findings of post mortem examination revealed SARS-CoV-2 viral particles in multiple organs, suggesting a variety of viral-transmission routes such as digestive tract, skin & other body fluids (saliva, urine, semen, milk, etc.). These issues merit further investigation. 3
In Italy, a similar study was done on 22 patients who died with COVID-19 and were autopsied. 4
In India, we follow ICMR guidelines which state that Post Mortem Examination is an inquest-based medical examination vide S 174 CrPC & S 176 CrPC and contains panchnama report, statements from various witnesses & other allied circumstantial evidence. Dissection of bones & tissues will generate aerosol that can lead to the spread of infection. On the basis of the same, general examination, external examination, examination of clothing, photographs, verbal autopsy (as depicted by WHO), criteria of exclusion, autopsy should be conducted strictly avoiding any invasive surgical procedures & splashing of body fluids for staff, body handlers and doctors involved in the autopsy procedure. 5
In BPS Govt. Medical College, Khanpur, Haryana, detailed PM examination along with histopathological findings in organs of an asymptomatic patient of COVID-19 & its comparison with histopathological findings in aluminium phosphide poisoning has been done. 6
Uncertainty around the emergence of SARS-CoV-2, which causes COVID-19, has led to fast and widespread diffusion of misinformation about the virus, its origins, prevention and treatment strategies.7, 8
Misinformation is not a new problem, but it poses challenges for infectious disease management when public acceptance is required for its prevention, such as social distancing and wearing a mask. Coronavirus is a novel virus and due to lack of knowledge and continuous mutation in the virus, it makes it difficult to handle and manage the same.
Aim and Objectives
To access the knowledge among forensic medicine experts regarding post-mortem examination and management of dead body of COVID-19 suspected or confirmed cases with the help of a questionnaire.
Materials and Methods
Study was carried out with the help of 20 questionnaires, which were circulated as a Google form among 50 forensic medicine experts in North India. The research was approved by the Institutional Ethics Committee. Objectives of the study were explained to them in detail. Online written informed consent was taken before proceeding further. Questionnaire was designed to study the attitude & knowledge regarding the procedure of post mortem examination in COVID-19 cases among doctors doing autopsy.
Inclusion Criteria
Doctors performing post mortems & consenting for participation in the study.
Exclusion Criteria
Doctors not consenting. Incompletely filled Google form.
Results
The following questions had been asked along with the response given by the experts as an answer:
Should we consider all dead bodies as COVID-19 positive in pandemic phase?
56% told yes, 42% told no while 2% do not know.
Should we take all precaution while performing autopsy in COVID-19 pandemic phase irrespective of COVID-19 status?
84% told yes while 16% told no
Should there be mandatory COVID-19 status testing for dead bodies before they are transferred for medico legal autopsy?
94% told yes, 4% told no while 2% do not know.
Do you think that COVID-19 positive dead body is infectious or not?
94% told yes, 2% told no while 4% do not know.
Is it ethically correct to conduct a non-invasive autopsy on a COVID-19 body as per ICMR Guidelines?
50% told yes, 40% told no while 10% do not know
Do the ICMR Guidelines need to be amended in light of two years of experience of COVID-19 pandemic?
90% told yes, 4% told no while 6% do not know
Should there be a segregated fully equipped mortuary for conducting autopsy on COVID-19 dead bodies?
96% told yes, 2% told no while 2% do not know
Do you think there should be a separate laboratory for toxicological, histopathological and serological investigation in COVID-19 cases?
90% told yes while 10% told no
Which test result do you consider significant in relation to COVID-19 status in context to performing autopsy?
66% asked for RT-PCR, 32% asked for Rapid Antigen test while 2% said none
Do you think that the present condition of mortuary throughout India is up to the standard of conducting autopsy on a highly infectious body such as COVID-19?
4% told yes, 94% told no while 2% told do not know
Do you agree with ICMR Guidelines on autopsy of COVID-19 body that mere external examination and history of cases are sufficient to frame an opinion in medico legal autopsy of a COVID-19 body?
16% told yes, 78% told no while 6% told do not know
A large number of autopsies have been conducted on COVID-19 bodies in other countries to find out region-specific pathology of this disease. Do you agree that such a study should be conducted in our country?
94% told yes, 4% told no while 2% told do not know
Disposal of autopsied COVID-19 dead body is responsibility of Doctor, Relative or Administration?
Responsibility of disposal of body by doctors is 2%, relatives 0%, while the administration is 98%
Should there be immediate disposal of COVID-19 dead body after post-mortem examination?
90% told yes, 6% told no while 4% told do not know
Should the status of COVID-19 be verified at the level of emergency department before transportation of dead body to prevent the unnecessary spread?
96% told yes, 2% told no while 2% told do not know
Are the medicos think that dead body becomes non-infectious after 48–72 hours?
30% told yes, 50% told no while 20% told do not know
Do you think that virtopsy is adequate in COVID-19 death?
40% told yes, 50% told no while 10% told do not know
Should there be quarantine for mortuary staff and doctors after performing a one-week duty in COVID-19 dead body examination?
92% told yes, 6% told no while 2% told do not know
Do you think the number of members of conducting post-mortem examination should be minimal or same as routine?
84% told yes, 14% told no while 2% told do not know
Should there be a COVID-19 sample taking training, for paramedical and medical staff?
96% told yes, 2% told no while 2% told do not know
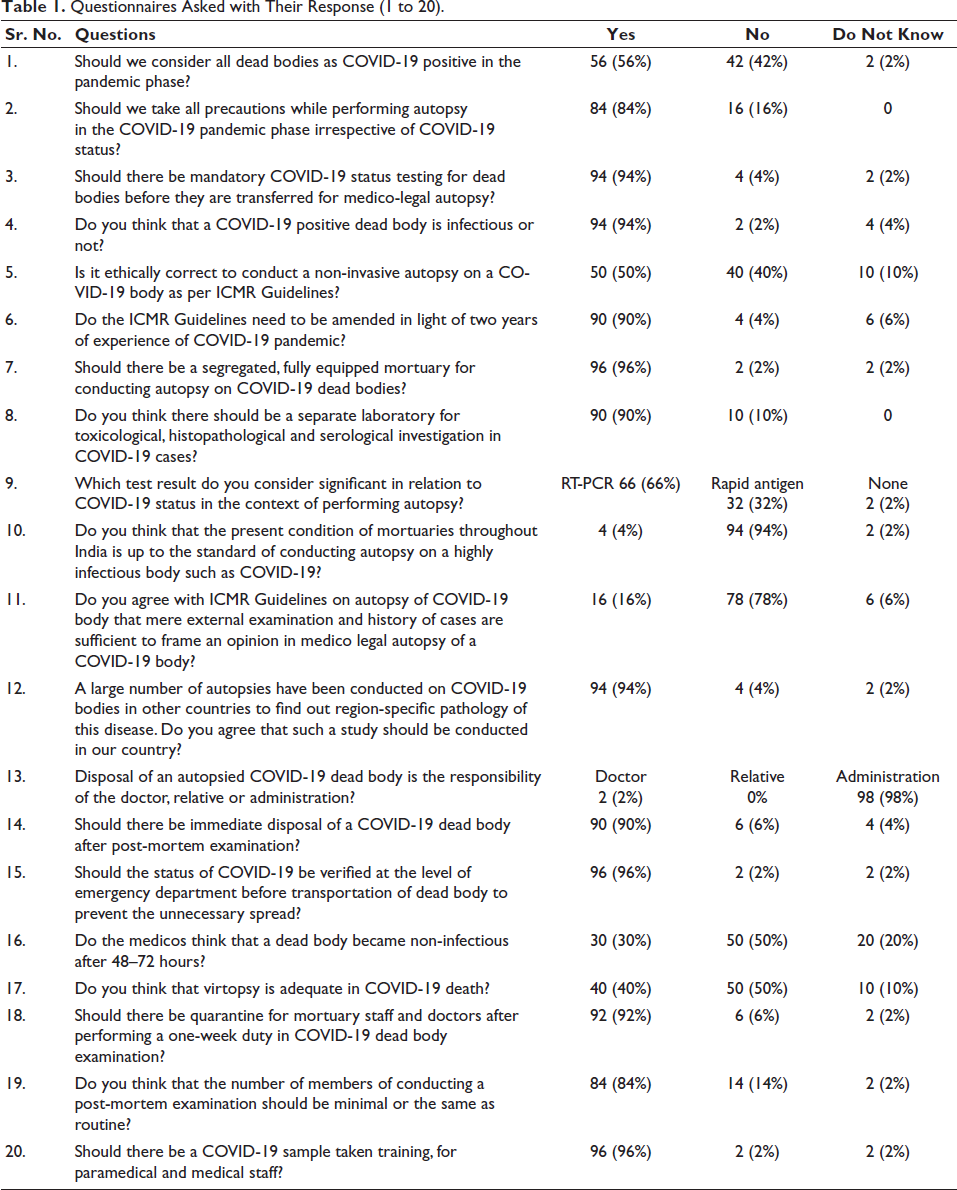
The result of the above-asked questions has been put in a table form as below (Table 1).
Questionnaires Asked with Their Response (1 to 20).
Discussion
Should we consider all dead bodies as COVID-19 positive in pandemic phase? In our current study, 56% of doctors agree with statement, whereas 42% of doctors disagree with statement, and 4% of doctors stated that they do not know.
Should we take all precautions while performing autopsy in COVID-19 pandemic phase irrespective of COVID-19 status? In our current study, 84% of doctors agree with the statement, whereas 16% of doctors disagree with the statement, and none of doctors stated that they do not know.
Should there be mandatory COVID-19 status testing for dead bodies before they are transferred for medico-legal autopsy? It is advisable to check COVID-19 status at an emergency department or casualty or ward or ICU in all suspected or latent cases before sending body to mortuary for preservation if it was not sent during hospital stay. 9 In our current study, 94% of doctors agree with statement, whereas 4% of doctors disagree with statement, and 2% of doctors stated that they do not know. To limit the unnecessary transmission, it is necessary that the COVID-19 status of the dead body should be known.
Do you think that a COVID-19 positive dead body is infectious or not? In our current study, 94% of doctors agree with statement, whereas 2% of doctors disagree with statement, and 4% of doctors stated that they do not know.
Is it ethically correct to conduct a non-invasive autopsy on a COVID-19 body as per ICMR Guidelines? In our current study, 50% of doctors agree with statement, whereas 40% of doctors disagree with statement, and 40% of doctors stated that they do not know.
Do the ICMR Guidelines need to be amended in light of two years of experience of COVID-19 pandemic? In our current study, 90% of doctors agree with statement, whereas 4% of doctors disagree with statement, and 6% of doctors stated that they do not know.
Should there be segregated, fully equipped mortuary for conducting autopsy on COVID-19 dead bodies? In our current study, 96% of doctors agree with the statement, whereas 2% of doctors disagree with the statement, and 2% of doctors stated that they do not know.
Do you think there should be a separate laboratory for toxicological, histopathological and serological investigation in COVID-19 cases? In our current study, 90% of doctors agree with statement, whereas 10% of doctors disagree with statement, and none of doctors stated that they do not know.
Which test result do you consider significant in relation to COVID-19 status in context of performing autopsy? In our current study, 66% of doctors agree with the RT-PCR, whereas 32% of doctors agree with the Rapid antigen test, and 2% of doctors do not agree with any of the tests.
Do you think that the present condition of mortuaries throughout India is up to standard of conducting a highly infectious body such as COVID-19? In our current study, 4% of doctors agree with statement, whereas 94% of doctors disagree with statement, and 2% of doctors stated that they do not know.
Autopsies on confirmed or suspected COVID-19 should be conducted ideally in airborne infection isolation rooms (AIIRs). If this is not available, another autopsy room with adequate air-handling systems may be used, which can:
Maintain negative pressure relative to surrounding area and with no air recirculation.
Provide a minimum of six ACH (air changes per hour) for existing structures & 12 ACH for renovated/new structures.
Exhaust air directly to unoccupied areas outside mortuary complex.
Having laminar flow systems that can direct air away from autopsy table downwards and away from personnel.
Have a Certified Class II Bio-safety Cabinet
Work surfaces should have an integral waste containment & drainage system that minimises spills of body fluids & wastewater. In addition, doors to a room should be kept closed except during entry and exit. Entry and exit should be limited to prevent interruptions in airflow.
A portable HEPA (high-efficiency particulate air) recirculation unit could also be placed in autopsy room to provide further air filtration.
If use of an AIIR or HEPA unit is not possible, autopsy should be performed in most protective environment possible.
Following combination of personal protective equipment (PPE) is recommended for PM examination:
Surgical scrub suit worn under impermeable gown/apron with full sleeve.
Double surgical gloves interposed with a layer of synthetic mesh gloves (cut proof).
A NIOSH-approved disposable N95 respirator should be worn; however, due to likelihood of generation of aerosols during various PM procedures, powered air-purifying respirators (PAPRs) equipped with N95/ HEPA filters are recommended:
PAPRs should be considered for people who cannot wear N95 respirators because of facial hair or other fit limitations.
PAPRs with high efficiency filters may provide increased comfort during extended PM procedures.
When respirators are mandatory to protect workers, employers must implement a comprehensive respiratory protection program in accordance with OSHA Respiratory Protection standard that includes medical examination, training & fit testing.
d. Eye protection such as goggles or face shield that covers front & sides of face:
Proper eye protection must be selected to ensure that N95 respirator does not interfere with correct positioning of eye protection & eye protection does not affect fit/seal of respirator.
Protective eyewear (e.g., safety glasses & face shield) without gaps between glasses & face to protect eyes from splashes.
e. Surgical cap.
f. Shoe covers having non-slip tread. 10
11. Do you agree with ICMR Guidelines on autopsy of COVID-19 body that mere external examination and history of cases are sufficient to frame an opinion in medico legal autopsy of a COVID-19 body? In our current study, 16% of doctors agree with statement, whereas 78% of doctors disagree with statement, and 6% of doctors stated that they do not know.
12. A large number of autopsies have been conducted on COVID-19 bodies in other countries to find out region-specific organ pathology of this disease. Do you agree that such a study should be conducted in our country? In our current study, 94% of doctors agree with statement, whereas 4% of doctors disagree with statement, and 2% of doctors stated that they do not know.
13. Disposal of autopsied COVID-19 dead body is responsibility of doctor, relative or administration? In our current study, 2% of doctors agree with the responsibility of doctors, whereas 98% of doctors agree with the responsibility of relatives. WHO & Royal College of Pathologists states that personnel who interact with body, like health care or mortuary staff or burial team, should apply standard precautions 11 and only trained personnel should handle such dead bodies. 12
Standard infection prevention control practices should be followed & these include:
Hand hygiene.
Use of PPE like water resistant apron, gloves, masks, eyewear.
Safely handling the sharps.
Disinfect bag having dead body; instruments & devices used on COVID-19 patient.
Disinfect linen and environmental surfaces. 13
14. Should there be immediate dispersal of COVID-19 dead body after post-mortem examination? In our current study, 90% of doctors agree with statement, whereas 6% of doctors disagree with statement, and 2% of doctors stated that they do not know. People who have died from COVID-19 can be buried/cremated. Confirm national & local requirements that may dictate handling & disposition of remains of body. Family & friends can view body after it has been prepared for burial, in accordance with customs. They should not touch or kiss dead body & should wash their hands thoroughly with soap and water after viewing. Those involved in placing body in grave or on funeral pyre, etc. should wear gloves and wash hands with soap and water after removal of gloves once burial or cremation is complete. 8
15. Should the status of COVID-19 be verified at the level of emergency department before transportation of dead body to prevent the unnecessary spread? In our current study, 96% of doctors agree with statement, whereas 2% of doctors disagree with statement, and 2% of doctors stated that they do not know.
16. Are the medicos think that dead body becomes non-infectious after 48–72 hours? In our current study, 30% of doctors agree with statement, whereas 2% of doctors disagree with statement, and 2% of doctors stated that they do not know.
17. Do you think that virtopsy is adequate in COVID-19 death? In our current study, 40% of doctors agree with statement, whereas 50% of doctors disagree with statement, and 10% of doctors stated that they do not know.
18. Should there be quarantine for mortuary staff and doctors after performing a one-week duty in COVID-19 dead body examination? In our current study, 96% of doctors agree with statement, whereas 6% of doctors disagree with statement, and 2% of doctors stated that they do not know.
19. Do you think that the number of members of conducting post-mortem examination should be minimal or same as routine? In our current study, 84% of doctors agree with statement, whereas 14% of doctors disagree with statement, and 2% of doctors stated that they do not know.
20. Should there be a COVID-19 sample taking training for paramedical and medical staff? In our current study, 96% of doctors agree with statement, whereas 2% of doctors disagree with statement, and 2% of doctors stated that they do not know.
Conclusion
We should consider all the dead bodies in pandemic area as COVID-19 positive. We take all the precautions while performing autopsy irrespective of COVID-19 status. There should be mandatory testing of COVID-19 bodies before transfer to mortuary to minimise the risk of transmission. COVID-19 dead body is infectious. There should be a new amendment in ICMR guidelines. There should be segregated, fully equipped mortuary, separate laboratory for toxicological, histopathological and serological investigation to minimise the risk of transmission.
Test for COVID-19 is RT-PCR, which is more accurate than Rapid Antigen. Mortuaries in India are not up to the standard of the guidelines. Non-invasive or minimal invasive autopsy is not sufficient to frame an opinion in a medico-legal case. Like other countries, in India also there should be a complete autopsy to know the pathology of disease, which can help in the treatment of patients.
Disposal of dead body as well as supply of PPE Kit is the responsibility of administration. There should be immediate dispersal of the COVID-19 dead body.
Footnotes
Acknowledgements
We are acknowledging the support and guidance provided by Dr Luv Sharma, Professor, Department of Forensic Medicine & Toxicology, Pt. B. D. Sharma PGIMS, Rohtak, Haryana.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was taken by Institutional Ethics Committee of World College of Medical Sciences and Research and Hospital, Jhajjar, Haryana. Online written informed consent was also taken from each participant doctor.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.