
Abstract
The most important and evident external finding of hanging is a ligature mark, which is a pressure abrasion. A ligature mark can tell so much about the material causing it and its antemortem origin if looked into with utmost care. This cross-sectional study makes a prompt and sincere attempt to study the pattern of ligature marks in hanging deaths and their relation to the materials producing it. The present cross-sectional study enrolled 210 cases of hanging deaths brought for autopsy to the mortuary wing of Government Medical College, Thiruvananthapuram, between March 2021 and October 2022. The classic non-continuous ligature mark which is situated over and above the level of thyroid cartilage was observed in the majority of the cases. Imprint pattern of the ligature material, grooving, the continuity of the ligature mark, and peri-ligature injuries showed a significant association with the consistency and type of ligature material used. The thyroid cartilage fractures and the cervical spine fractures showed a significant association with the position of the knot.
Keywords
Introduction
The principal external sign of hanging is a ligature mark which is a pressure abrasion caused by the loop of ligature around the neck. A classic ligature mark seen in hanging death appears as a groove encircling the neck and obliquely placed above the level of the thyroid cartilage, often showing discontinuity at the point of suspension which is the highest point of ligature mark on the neck. But atypical marks like horizontal ligature marks, absent ligature marks, and multiple ligature marks are also reported in hanging deaths though in small proportions especially in partial hanging, when soft ligatures are used or when multiple loops are used. Solving the puzzle in such a case needs expertise. Eccentricities of ligature marks and the reason behind them must be evaluated and validated carefully in the medicolegal investigation of hanging deaths. The signs of vitality of the ligature mark, the patterns imprinted by the ligature material on the mark, and the peri-ligature injuries, though subtle, are changes that should be looked upon with utmost care and precision. In the present study, a prompt and sincere attempt is being made to study the pattern of ligature marks in hanging deaths and their relation to the material producing it and the associated internal injuries.
Materials and Methods
The cross-sectional study enrolled 210 cases of hanging deaths brought for autopsy to the mortuary wing of Government Medical College, Thiruvananthapuram, between March 2021 and October 2022. The study commenced after obtaining the institutional ethics committee clearance. Data was recorded using semi-structured proforma and analysed using SPSS software version 25.0. The χ2 test and Fisher’s exact test were used to test the association between categorical variables and a P < .05 was considered significant.
Observations and Discussion
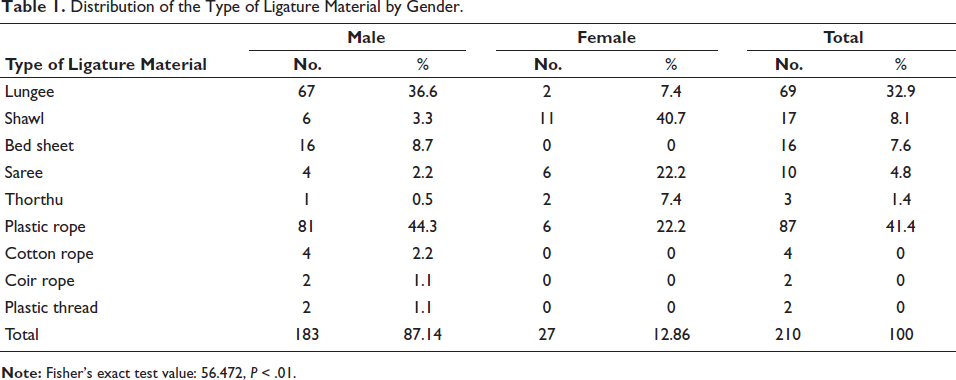
The majority of the victims were males (87.14% of cases). All cases were suicidal hanging. Most of the victims preferred their homes and their premises as a place of hanging (87.3% of cases). The body was seen suspended completely in 62.86% of cases. The victims preferred a soft ligature material over a hard ligature material in 54.76% of cases, agreeing with a previous study by Jayaprakash S and Sreekumari K. 1 However, when we measured the frequency of the type of ligature in the sample, plastic rope (41.4%) which is a hard ligature material outnumbered all others. This was in agreement with observations of Tumram et al., 2 Pradhan A et al. 3 and Ambade et al. 4 Lungee (32.9%) was the second most common ligature material preferred by the victims of hanging in the present study population. Soft materials like saree, shawl, and lungee are daily worn clothes and other soft materials like thorthu and bed sheets are easily available at home making them the favourite ligature material of choice. Plastic ropes are also used for various purposes in daily living and hence are easily available at home compared to other hard materials (Table 1).
Distribution of the Type of Ligature Material by Gender.
The width of the ligature varied from 2 cm to 260 cm. The thinnest hard material observed had a total circumference of 1 cm and the thinnest soft material observed had a width of 2 cm (Table 2). In the case of the thinnest soft material, which was the border piece of a lungee, the suspension was partial and the victim was standing with feet flat on the ground.
Distribution of the Number of Loops Around the Neck by Width/Total Circumference of the Ligature.
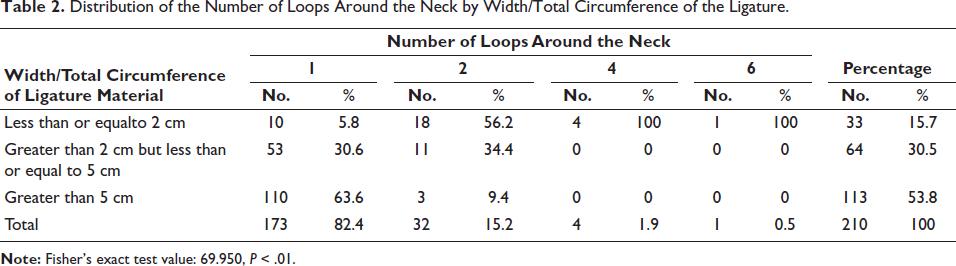
In 82.4% of the cases, a single loop of ligature was seen around the neck constituting the majority. Multiple loops were observed in 17.6% of cases of which 32 cases had double loops, four cases had four loops, and a single case had six loops. It has been observed that when the width/total circumference of the ligature material was 2 cm or less, cases with multiple loops outnumbered cases with a single loop, deviating from the norm that single loops are common in hanging. As the width of ligature material increases the frequency of multiple loops showed a decline in the study sample. Though uncommon, multiple loops are not a rare event in suicidal hanging. It could be a reinforcing method adopted by a desperate victim when he/she is unsure about the load-bearing strength of a thin ligature material. Thin ligature materials commonly used are hard materials. Ambade et al. noted a higher incidence of multiple loops when hard materials are used.
The most common knot observed in the present study was a slip knot (87.6%) similar to the results of other studies by Jayaprakash S and Sreekumari K, 1 and Ambade et al. 4 but differing from the observations of Sharma et al. 5 who observed fixed knot in the majority. Other knots noted in the study sample were half-knot (9%), cow-hitch knot (2.4%), Hangman’s knot (0.5%), and overhand running loop knot (0.5%). All these knots except the half-knot are slipping knots producing a running noose when placed around the neck. Half-knot is a highly unstable knot and tends to untie easily. The Hangman’s knot is an example of an occupational knot. But in the single case where Hangman’s knot was observed; the occupation of the victim was not related to the knot.
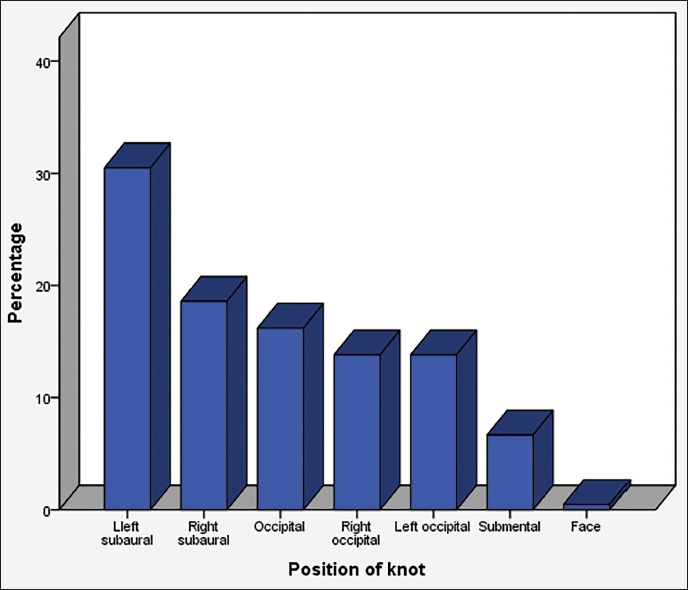
As depicted in Figure 1, the most common position of the knot observed in the present study was left subaural (30.5%) followed by right subaural (18.6%). The least common position was the face (0.5%) followed by the submental (6.7%). Typical hanging with a knot over the occiput was seen in 16.2% of cases. The knot was observed in the left and right occipital positions in 13.8% of cases each. The left subaural as the most common knot position was also noted in a previous study by Ambade et al. 4 The left subaural region being an easily accessible site for a right-handed individual might be the reason for its higher frequency observed in the sample population.
Bar Diagram Showing the Distribution of the Position of the Knot.
Apart from multiple loops the victim often uses restraint knots using the free ends or other materials either to reinforce the knot forming the loop to prevent the slippage of the knot or to tie the multiple free ends together when multiple ligature materials are used. In the present study, such knots were absent in the majority of the cases (71.4%). In the cases where restraint knots were present, they were simple knots either single or multiple, and in most of the cases, they were observed to be placed on either of the free ends just distal to the knot forming the loop on the neck.
Measures taken to prevent escape or to reduce pain in cases of suicidal hanging were observed to be adopted by four male victims in the present study. Two of them used mouth gags: a piece of a lungee and a handkerchief respectively. The purpose of such measures could be to prevent calling out for help. However, such findings are very rare in suicides. So, all other possibilities of a foul-play must be excluded before declaring it as a desperate attempt of the victim to prevent escape from the act of hanging.
Padding the neck with soft cloth was adopted by the other two male victims. One of them used a kitchen towel to place as a cushion between a loop made of plastic rope and the neck ensuring complete encirclement of padding material around the neck. The resulting pressure abrasion was a broad mark having a weaving pattern of the cloth. In the other case, the male victim used thorthu (a type of bath towel) as a cushion between the neck and the loop made of plastic rope, but the padding did not encircle the neck completely and did not have the desired cushioning effect due to slippage of the material. Padding the neck with a soft cloth is done to reduce the pain during hanging. This practice is also reported in cases of auto-erotic hanging.
Demirci et al. 6 observed the practice of using a scarf as a padding material commonly by female victims and male victims used the collar of their shirt as padding material. The present study observed male victims to have taken some measures to reduce pain or to prevent escape. A broad ligature mark or absent ligature mark when the alleged ligature used is a hard material, a remote possibility of padding of the neck must be ruled out before alleging a foul play. In none of these cases in the present study, ligature restraints in other parts of the body were noted whereas Demirci et al. 6 observed ligature restraints in some cases.
The ligature mark was single in 99.5% of the cases agreeing with the existing literature. In one case, it was three in number. In the only case exhibiting multiple ligature marks two plastic ropes were wound three times around the neck by crossing the ends of the rope in the midline on the front and back of the neck finally ending in a half-knot at the back aspect of the neck. So, there were three ligature marks merging at some point in their course at three different levels in the neck. Though 17.6% of cases used multiple loops multiple ligature marks were observed in only one case (0.5%). In all other cases, the marks made by individual loops around the neck were merging all around their course and an intervening strip of skin appeared as a slightly raised transverse reddish ridge between two grooves making it difficult to distinguish the two marks as separate. But the presence of such a ridge is difficult to miss and we can predict the multiplicity of loops around the neck and the consistency of the ligature material accurately when hard materials are used. But soft and broad materials often show a single ligature mark even when multiple loops are used and predicting the multiple nature of loops is difficult in such cases.
The colour of the ligature mark varied as pale, reddish, pale brown, and dark brown in the study sample. Dark brown pressure abrasions accounted for 59% of cases. The colour of the ligature mark showed a significant association with the consistency of the ligature material used. When a hard ligature material was used the majority showed a dark brown ligature mark (93.7%) followed by a pale brown mark (5.3%) and a reddish mark (1.1%%). Soft ligature materials were associated with a pale brown mark (46%) followed by a dark brown mark (30.4%) and a pale mark (23.5%). In none of the cases, a pale mark was observed whenever a hard ligature material was used. Hard ligatures due to the roughness of their surface abrades the skin more compared to a soft and smooth material. Abraded skin in the pressure abrasion loses moisture gets a parchment look and appears much darker and drier with time.
The mark was non-continuous in 53.81% of the cases and continuous in 46.19% of the cases. Tumram et al., 2 Ambade et al. 4 and Jayaprakashs S and Sreekumari K 1 also observed a classic non-continuous ligature mark in the majority of the cases. When the ligature material used was soft, the majority of the victims showed a non-continuous mark (70.4%) in the present study. However, when a hard ligature material was used, a continuous mark was seen in the majority of the victims (66.3%). This association between the consistency of ligature material and continuity of ligature mark was significant (P < .01 for Pearson χ 2 : 28.27).
The mark was situated over and above thyroid cartilage in the majority (63.3%) and was obliquely placed in 99.05% of cases. The mark was situated above the level of the thyroid cartilage in 31.9% of cases and over the thyroid cartilage in 4.3% of cases. The mark was situated below the thyroid cartilage in only one case. The mark may appear transverse or below the level of the thyroid cartilage, when the point of suspension is low or when the noose made of thin and hard material tightens around the neck immediately after suspension of the body, making the upward slipping of the noose impossible or when the thin and hard ligature materials are wound around the neck multiple times by crossing the ends of the ligature material.
Grooving was present in 30.5% of study subjects. When the ligature material was a hard one, more than half of the victims showed grooved ligature marks (61.1%). When a soft ligature material was used, grooving was present in 5.2% of cases. A significant association was present between the consistency of ligature and the grooving of the ligature mark. Tumram et al. 2 observed grooved ligature marks in 53.7% of cases and hard materials like rope were used as the ligature material in all such cases.
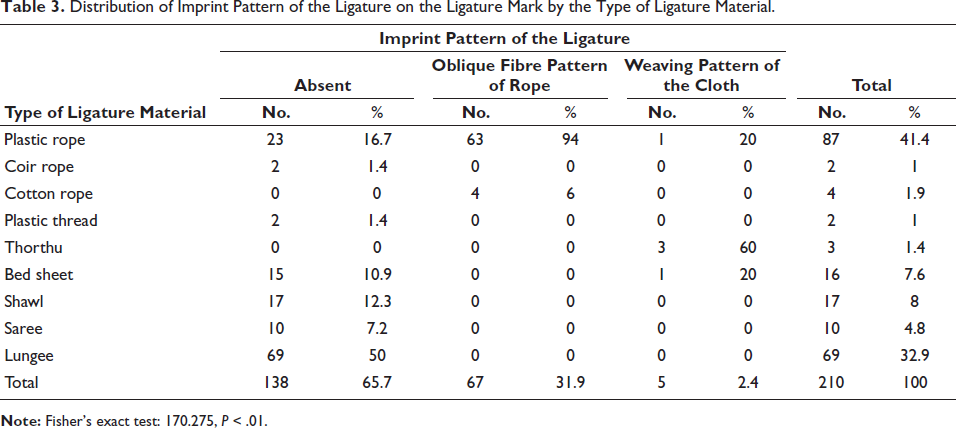
The most common imprint pattern noted was the oblique fibre pattern of rope, seen in 31.9% followed by the weaving pattern of cloth in 2.4% of cases in the present study (Table 3). Among the cases with an oblique fibre pattern of rope, 94% used a plastic rope and 6% used a cotton rope as a ligature material. Weaving pattern of cloth was seen only in five cases of which the majority was produced when thorthu (a type of bath towel) was used as a ligature (three cases or 60%). The bed sheet was the other soft material imprinting its pattern to the ligature mark, seen in one case (20%). Interestingly the weaving pattern of cloth was observed when the ligature material used was a plastic rope in one case (20%), where a kitchen towel was used for padding the neck. So, it is not always the ligature that imprints its pattern in the ligature mark. Any material that gets entrapped between the ligature and the neck can influence the imprint pattern of the ligature mark. Tumram et al. 2 observed imprint patterns of ligature in 32.5% of cases, similar to the findings of the present study. Jayaprakash S and Sreekumari K 1 observed an imprint pattern of rope in 4.2% of cases.
Distribution of Imprint Pattern of the Ligature on the Ligature Mark by the Type of Ligature Material.
Peri-ligature injuries like blisters, abrasions, ecchymosis and nail marks were observed in 21% of cases (Table 4). The commonest peri-ligature injury observed was blister (17.1%) followed by abrasion (2.9%). Ecchymosis and nail marks were rarely observed (0.5% of cases each). The majority of the cases (79%) did not show any peri-ligature injuries. When a hard ligature material was used 37% showed peri-ligature injuries compared to 7.8% where a soft ligature material was used. Blisters were more commonly associated with a hard ligature material (31.6% of cases that used hard ligature material) than a soft material (5.6% of cases that used a soft ligature material). Abrasions showed almost equal distribution among the two groups. Blisters were commonly seen either along the upper border (50%) or within the mark (47.2%). The majority of the abrasions were seen merging with the ligature mark (66.6%) and were situated either above or below the ligature mark (33.3% each). Abrasions not merging with the ligature marks were observed only in two cases. In one case the abrasion was situated below the ligature mark and in the other case, it was situated above the ligature mark.
Distribution of Peri-ligature Injuries by the Consistency of Ligature Material.
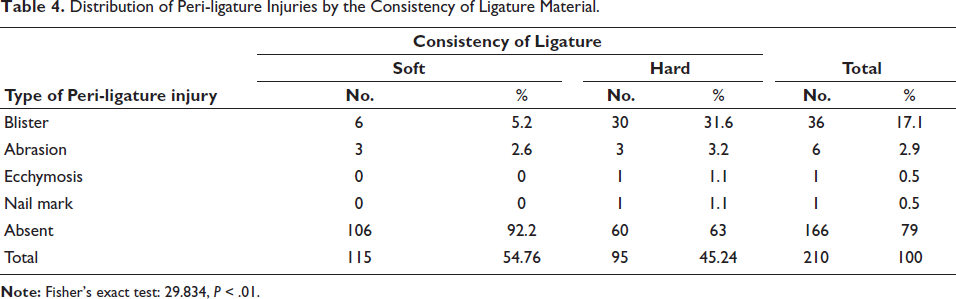
A significant association was present between the type of peri-ligature injuries with the consistency of the ligature material and between the type of peri-ligature injury and the location of the peri-ligature injury in the present study. Blisters are produced due to heat generated by friction between the loop of ligature and the skin of the neck. The maximum amount of friction is seen along the upper border in the case of single or multiple loops and the intervening skin trapped between the loops in case of multiple loops and hard ligature material tends to exert more friction than soft. This might be the reason why blisters are more commonly associated with hard ligature material than soft materials and their peculiar locations. Abrasions merging with the ligature mark might be due to the slippage of ligature upwards during the act of hanging due to the gravitational drag by the weight of the body. Jayapraksh S and Sreekumari K 1 also noted blisters along the margins in 2.1% of cases when the synthetic rope was used as ligature material. Tumram et al. 2 also noticed peri-ligature injuries like blisters, abrasions, and ecchymosis when hard materials like ropes were used and abrasions and ecchymosis were noted with soft ligature material. Tumram et al. 2 noted peri-ligature blisters on the upper border and abrasions below the ligature mark in the majority of the cases. The presence of peri-ligature injuries strongly suggests an antemortem origin but abrasions can happen during the perimortem period or resuscitation. Ecchymosis situated below the level of ligature mark is more likely to be antemortem as it will not be influenced by stasis of blood in the engorged blood vessels due to constriction by the loop of ligature.
Salivary dribble mark, an antemortem sign of hanging was observed in 18.6% of cases in the present study. A salivary dribble mark was observed in none of the cases when the knot was submental in position or on the face. It was present on the right side when the knot was left subaural (75%), left occipital (15%) or occipital (5%) in position. Salivary dribble was seen on the left side when the knot was right subaural (57.1%), occipital (7.1%) or right occipital (35.7%) in position. Ambade et al. 4 noted salivary dribble in only 11.8% of cases. Evidence of excessive salivation is more of a crime scene finding than a postmortem room finding. A long postmortem interval and manipulation of the dead body by external agencies such as the removal of clothes worn by the victim and wiping the body of the victim often result in the loss of this finding. This might be the reason behind such variation in the frequency of distribution among different studies. So, educating the investigating officers regarding the significance of such findings and the importance of recording and preservation of such findings is necessary from the medicolegal point of view.
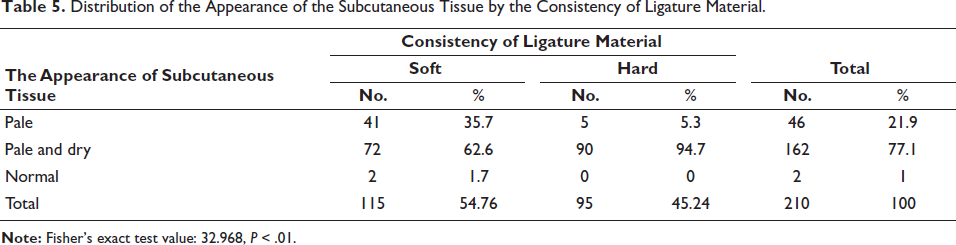
The subcutaneous tissue underneath the pressure abrasion was pale and dry in the majority of the cases (77.1%) (Table 5). When a soft ligature material was used the subcutaneous tissue appeared pale and dry in 62.6% of cases, pale in 35.7% of cases, and normal in 1.7% of cases. Among the victims who used hard ligature material, the subcutaneous tissue appeared pale and dry in 94.7% of the cases and pale in 5.3% of cases. Only two cases showed normal subcutaneous tissue and the ligature material used was a soft one in both cases. There was a significant association between the consistency of ligature material and the appearance of subcutaneous tissue. Ambade et al. noted pale and dry subcutaneous tissue in 78.7% of hanging deaths. Jayaprakash S and Sreekumari K 1 noted that in 95.8% of hanging deaths, the subcutaneous tissue was pale and dry. The observations of the present study are consistent with the findings of previous studies.
Distribution of the Appearance of the Subcutaneous Tissue by the Consistency of Ligature Material.
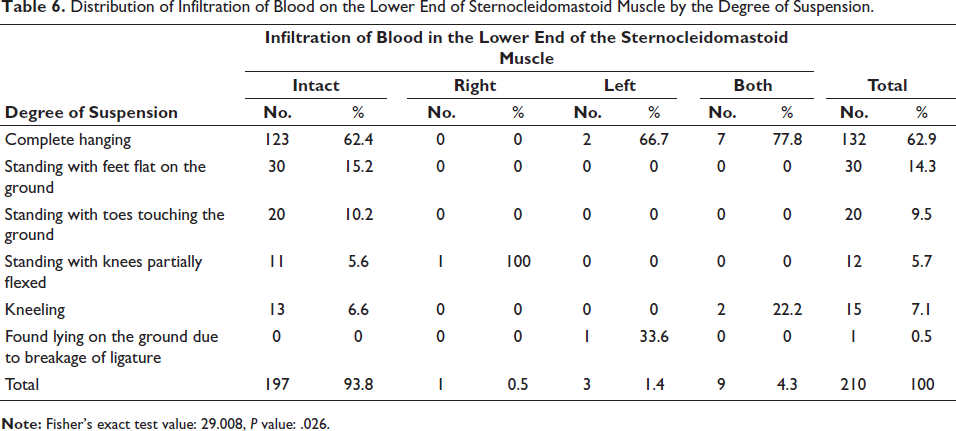
Sternocleidomastoid muscle showed infiltration of blood in the lower end in 6.2% (13 cases) of cases in the present study (Table 6). In 4.3% of cases, both sternocleidomastoid muscles showed infiltration of blood in their lower end. In 1.4% of cases, only the left sternocleidomastoid showed infiltration of blood in its lower end, and in 0.5% of cases, only the right sternocleidomastoid muscle showed infiltration of blood in its lower end. Most of the cases showing infiltration of blood in the lower end of the sternocleidomastoid muscle belonged to the group of complete hanging (9 out of 13 cases), agreeing with the results of Hejna and Zatopkova. 7 Hejna and Zatopkova 7 stated that there is a significant association between the position of the knot on the neck and the completeness of suspension with the occurrence of haemorrhage. A significant association was noted between the degree of suspension and infiltration of blood in the lower end of the sternocleidomastoid muscle in the present study. Among the 13 cases with infiltration of blood in the sternocleidomastoid muscle, a hard ligature material was used in nine cases and a soft ligature material was used in four cases. Sivasuthan S et al. 8 noted rupture of the lower end of the sternocleidomastoid in 62% of cases and attributed it as an antemortem sign of hanging. Jayaprakash S and Sreekumari K 1 noted sternocleidomastoid muscle injury in 19.2% of cases on the same side of the knot but the present study did not find any such association with the position of the knot.
Distribution of Infiltration of Blood on the Lower End of Sternocleidomastoid Muscle by the Degree of Suspension.
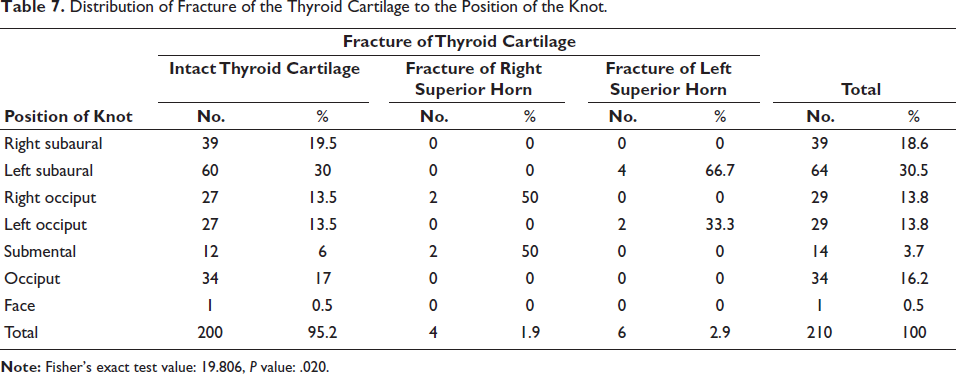
In the present study, the fracture of thyroid cartilage was noted in 4.76% of cases (Table 7). All were superior horn fractures. When the left superior horn was seen fractured, the position of the knot was either left subaural (66.7%) or left occipital (33.3%). The right superior horn fracture was associated with the knot position of the right occipital and submental (each 50%). There was a significant association between the position of the knot and fracture of the thyroid cartilage in hanging deaths in the present study. Similar to the results of the present study, isolated fracture of the superior horn of thyroid cartilage was the most common type of injury encountered in deaths due to hanging in studies conducted by Jayaprakash S and Sreekumari K, 1 Zatopkova et al., 12 Khokhlov, 9 Kurtulus et al. 10 and Nikolic et al. 11 Zatopkova et al. 12 noted the maximum incidence of fracture of the thyroid cartilage in lateral hanging (knot was on sides of the neck) which is in agreement with the present study. But, according to Nikolic et al. 13 occipital, right occipital and left occipital knot positions were commonly associated with superior horn fracture. The hyoid bone fracture was noted only in 1.5% of cases in the present study. The knot was on the back of the neck in all the cases (occipital in two cases and left occipital in one case), agreeing with Kurtulus et al. 10 that the commonest knot position was occipital in the case of hyoid fracture. A posterior knot position exerts maximum compression over the anterior aspect of the neck by the ligature material, resulting in maximum divergence stress in greater horns causing their fracture. Cervical spine fracture was observed in 2.4% of cases in the present study. All of them were associated with a submental position of knot. The fracture level was between C3 and C4 (1% of cases) and between C5 and C6 (1.4% of cases). A significant association was observed between cervical spine injury and the position of the knot. These findings tally with Nikolic and Zivkovic 14 that anterior knot position is associated with cervical spine injuries. Hyperextension and distraction of the cervical spine during hanging with a submental positioning of the knot are responsible for cervical fractures in hanging.
Distribution of Fracture of the Thyroid Cartilage to the Position of the Knot.
Conclusion
The classic non-continuous ligature mark which is situated over and above the level of thyroid cartilage was observed in the majority of the cases. Imprint pattern of the ligature material, grooving, the continuity of the ligature mark, and peri-ligature injuries showed a significant association with the consistency and type of ligature material used. The thyroid cartilage fractures and the cervical spine fractures showed a significant association with the position of the knot.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
The study was commenced after approval of Institution Ethics Committee, Government Medical College, Thiruvananthapuram. Prior to data collection, informed written consent was taken from next of kin of the decedent and anonymity was maintained throughout the study.