
Abstract
Falls are the second most common cause of injury-associated mortality after traffic accidents. The present study aims to find out the pattern of injuries among the victims of falls from height. This prospective observational study was conducted among victims of falls from height at SRTR Government Medical College morgue during the period of July 2020 to July 2022. All medico-legal cases involving head injuries brought for autopsy during the study period were included. Exclusion criteria include all medico-legal cases not involving head injury, advanced decomposed bodies, intracranial haemorrhage, infarctions, lesions as a result of natural disease. Various data were collected. A total of 996 autopsies were performed during the study period out of which 48 (4.82%) were cases of fall from height. Among them 30 (62.5%) were male and 18 (37.5%) victims were female. Most of the victims were day labourers or construction workers 16 (33.33%). Most deaths occurred during day time 35 (72.92%) with the highest mortality being due to accidental falls 31 (64.58%). The age of maximum victims was between 31 and 40 years (37.5%). All the victims had multiple abrasions and bruises on their bodies, followed by intracranial haemorrhage 42 (87.5%), laceration 34 (70.84%) among others. In the skull, linear fracture was the most common 26 (54.17%). Temporal bone was the commonest bone to fracture 25 (52.08%) and most of the victims 17 (35.42%) had a subdural haemorrhage. Most common cause of death is due to major injuries overhead 36 (75%). Strategies designed to prevent these falls should have a substantial effect.
Introduction
Falls are the second most common cause of injury-associated mortality after traffic accidents. 1 A fall is defined as an injury to a person that occurs after landing on the ground after falling from a higher place, such as a ladder, scaffold, building, roof or other elevated place or work area. 2 Factors determining serious and fatal injuries in a fall depend on the distance of the fall, the characteristics of the landing surface, the orientation of falling, and whether the fall was direct or broken. 3 The skull, brain, spinal cord and extremities are the most commonly injured systems. Falls from first/second stories are more frequently nonfatal, but falls from more than twenty feet have historically been triaged to trauma centres. But even low-level falls can cause serious head injuries and death.4, 5
Objectives
The objective of this study was to find out the pattern of injuries among the victims of falls from height.
Materials and Methods
This prospective observational study was conducted among the victims of falls from height at SRTR Government Medical College and Hospital morgue during the period of July 2020 to July 2022.
Various data of the victim were collected from inquest reports submitted by the investigating officers. Specific points regarding injuries were noted during autopsy examinations. Later on, the data were analysed.
Results
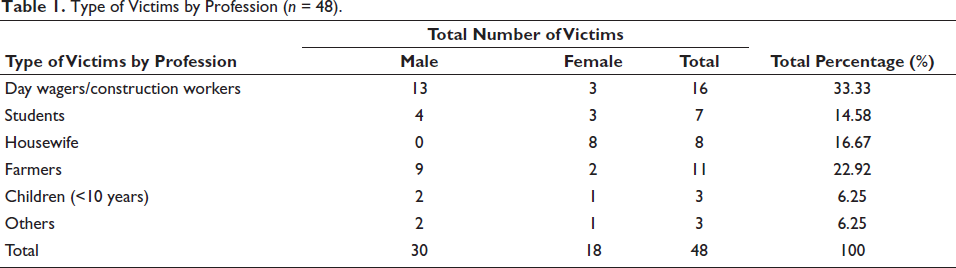
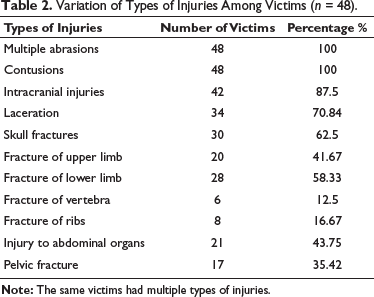
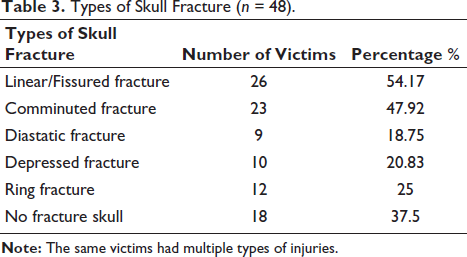
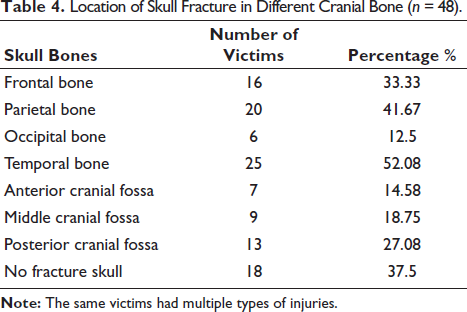
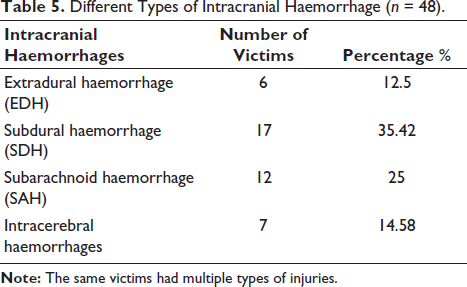
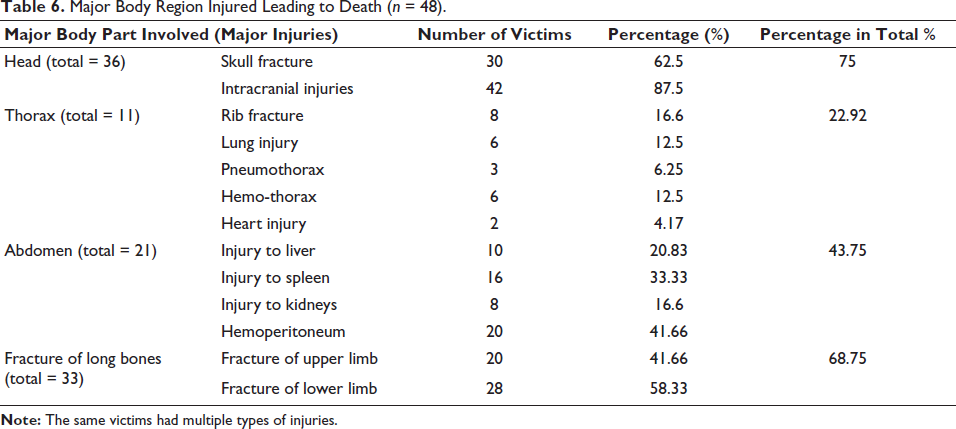
A total of 996 autopsies were performed during the study period out of which 48 (4.82%) were cases of fall from height. Among them 30 (62.5%) were male and 18 (37.5%) victims were female. Most of the victims were day labourers or construction workers 16 (33.33%) (Table 1). Considering timing, the highest incidents occurred during the daytime 35 (72.92%) and 13 (27.08%) at night. The highest mortality is due to accidental falls 31 (64.58%). The ages of maximum victims were between 31 and 40 years (37.5%). All the victims had multiple abrasions and bruises all over the body, followed by intracranial haemorrhage 42 (87.5%), laceration 34 (70.84%), fracture of skull bone 30 (62.5%), injury to long bones of upper limbs 20 (41.67%), injury to long bones of lower limbs 28 (58.33%), injury to abdominal organs like liver, spleen, kidney 21 (43.75%), fracture of pelvis 17 (35.42%) (Table 2). In skull bones linear fracture was the commonest one 26 (54.17%) (Table 3), Temporal bone was the commonest bone to fracture 25 (52.08%) (Table 4) and most of the victims 17 (35.42%) had subdural haemorrhage (Table 5). The most common injuries responsible for death were injuries over the head 36 (75%) followed by injuries over the thoracic region 21 (22.92%), abdominal region 21 (43.75%) and due to fracture of long bones 33 (68.75%) (Table 6).
Type of Victims by Profession (n = 48).
Variation of Types of Injuries Among Victims (n = 48).
Types of Skull Fracture (n = 48).
Location of Skull Fracture in Different Cranial Bone (n = 48).
Different Types of Intracranial Haemorrhage (n = 48).
Major Body Region Injured Leading to Death (n = 48).
Discussion
Injury due to falls from height remains a significant cause of morbidity and mortality in our day-to-day lives. Fatalities occur primarily when a person falls from greater than two stories or when the head of the victim hits a hard surface. This includes falls from rooftops, windows and balconies.3–5 In an Indian study, falls from height comprised the highest number of deaths among workplace accidents and the majority of these falls were from construction sites. 6 In this study, most of the victims were day labourers or construction workers 16 (33.33%) followed by housewives 8 (16.67%), farmers 11 (22.92%), students 7 (14.58%), children and others 3 (6.25%). Considering timing highest incidents occurred during daytime 35 (72.92%) and 13 (27.08%) at night.
Males are predominantly the earning members in our society context. Generally, men are exposed to trauma and falls more often than women because boys are more active than girls at early ages and more men are physical labourers than women.7, 8 In this study 30 (62.5%) were male and 18 (37.5%) victims were female. Nowadays a number of high-rise buildings are being constructed in Ambajogai City and nearby places and being a rural area building safety codes are not always properly followed. This indicates the significance of the highest number of victims as construction workers. Falling from rooftops and buildings is usually considered accidental in nature. But sometimes due to familial disharmony, financial issues, failure in examination, emotional blackout after refusal by lovers, drug addiction also leads to suicidal cases as these sites are commonly used to commit suicide. Homicidal cases are also not rare. Circumstantial evidence of some cases which occurred during the night points towards homicidal activities. In this study, most of the victims died due to accidental falls 31 (64.58%) followed by suicidal falls 10 (20.84%), homicide 5 (10.42%) and 2 (4.16%) were undetermined.
The Indian construction industry is the second largest contributor to the nation’s economy. While the industry is set to pick pace in the coming years, the government has also established regulations on how construction workers are supported. They include:
The Fatal Accidents Act, 1885 The Workmen’s Compensation Act, 1923 The Factories Act, 1948 The Employees State Insurance Act, 1948 The Central Labour (Regulation & Abolition) Act, 1970 Building & Other Construction Workers (Regulation of Employment and Conditions of Services) Act, 1996 Building & Other Construction Workers Welfare Cess Act, 1996 Building & Other Construction Workers (Regulation of Employment and Conditions of Services) Central Rules, 1998 The National Building Code of India, 2005
The falls from greater heights tend to cluster in the summer months, presumably because windows are more likely to be open and children are more likely to be playing on fire escapes, roofs and balconies.4, 9, 10 Falls in the elderly tend to occur with activities of daily living. In England falls account for 29% of injury deaths among adults aged 65 and older. Older adults are five times more likely to be hospitalised due to falls than to injuries from other causes. 11
Overall, in this study, 28 (58.34%) of the patients were between 20 and 40 years old, indicating that people of active ages are more frequently involved in trauma. Older individuals, especially those over 60 years old, lose their ability to balance, which causes more falls. 12 Host factors such as poor muscle tone, vision problems, medication use and sedentary lifestyle are the biggest contributors to ground-level and stair falls, but environmental components such as poor lighting and no handrails may increase the frequency. Factors contributing to falls from heights include faulty equipment, such as ladders and scaffold structures, and human factors, such as intoxication and inattention.
In this study, all the victims had multiple abrasions and bruises on their bodies which were minor in nature and not a definitive cause of death. Head trauma and severe loss of blood that leads to shock were the most common causes responsible for death due to blunt traumatic injury. In this study, the major cause responsible for death was head injury 36 (75%) in the form of skull bone fracture 30 (62.5%) and intracranial haemorrhages 42 (87.5%), followed by thoracic injury 11 (29.92%) in the form of fracture ribs 8 (16.67%), lung 6 (12.5%) and heart 2 (4.17%) injuries, pneumo-thorax 3 (6.25%) and haemothorax 6 (12.5%), abdominal injuries 21 (43.75%) in the form of injuries to liver 10 (20.83%), spleen 16 (33.33%), kidneys 8 (16.6%) and hemoperitoneum 20 (41.66%), long bone fractures 33 (68.75%) including upper 20 (41.66%) and lower 28 (58.33%) limbs.
Musemeche et al. and Meller et al. noted that fractures of the radius, ulna and femur were the most common injuries.13, 14 Velcek et al. and Lehman et al. in their study pointed out that, rib, spine, pelvis and calcaneus fractures were much less common among children than among adults because children tend to use their arms to protect their heads and they have relatively flexible bones.15, 16 Meller et al. and Lehman et al. noted that multiple fractures and cranio-cerebral trauma were common, especially in those cases that resulted from falls from greater heights. Abdominal and chest injuries were relatively uncommon in low-height falls but they are more frequent in fatal falls from greater heights.14, 16 In this study, the occurrence of major injuries was less in children as compared to the adult population.
The nature of the surface onto which the victim falls and the degree to which the fall is broken on the way down modify the pattern and severity of injuries. Children younger than three years are much less likely to have serious injuries than older children who fall the same distance because younger children have more fat and cartilage and less muscle mass than older children, they better dissipate the energy transferred by the fall. 17
The same victims had multiple types of skull fractures like linear, comminuted, depressed, diastatic and others. The force required to cause fracture depends on area of the skull struck, the thickness of the skull, scalp and hair and direction of impact. In this study, among skull bones linear fracture was the commonest one 26 (54.17%) and Temporal bone was the commonest bone to fracture 25 (52.08%). A skull fracture can occur if the moving head directly strikes an object in case of fall from height, it can be the hard ground. The linear fracture can also occur on the opposite side by contrecoup if the head moves and its movement is suddenly arrested by coming in contact with a hard surface. In most cases of fall from height head strikes by forcible contact with broad resisting surfaces like the concrete or tarred ground resulting in the liner fracture. The thinnest area in our skull is temporal bone (4 mm), followed by frontal bone (6 mm), parietal bone (10 mm) and occipital bone (15 mm). A force of 400–600 pounds per square inch is required to fracture a skull covered by a cushion of hair and scalp. However, a fall from three feet height will produce an impact energy of 35 feet pounds, causing two linear fractures or mosaic fractures. This indicates the predominance of different fractures, where the victims of fall from height are thrown with great impact.18, 19
This study has shown that most of the victims 17 (35.42%) had a subdural haemorrhage. Subdural haemorrhage is due to vascular injury, especially the bridging veins, where the head rapidly decelerates because of impact to a firm, underlying surface.
Subdural haemorrhages most commonly occur in old ages and children due to falls on ground by accidents, whereas subarachnoid haemorrhages were the most common pattern in intra cranial haemorrhage in RTA. Extradural haemorrhages were more common in 20–40 years of age and occurred mostly due to road traffic accidents (RTA) or hit by any other object. 20 Acute extradural haemorrhage is generally due to rupture of the middle meningeal artery as a result of fracture at ‘pterion’, an H-shaped formation of sutures on the side of the skull representing the junction of four skull bones, that is, Frontal, parietal, temporal and greater wing of the sphenoid.
The majority of traumatic deaths occurred in pre-hospital settings; on-scene or during transport and the leading cause of death is poly-trauma. The incidence of pre-hospital mortality is great among overall trauma-related deaths. So, pre-hospital medicine and trauma prevention programmes are significant factors in reducing traumatic deaths. 21
Conclusion
From the above study, we can arrive at a conclusion that most of the victims who died due to falls from height were construction site workers and death was accidental in nature and was preventable. Employers need to provide better access to job sites and invest in safety equipment that secures a worker. This includes both securing the worker to a safety line and providing a safety helmet. It is important that all scaffolding jobs should be carried out by trained professionals who are knowledgeable about the specialised safety equipment. This also includes the maximum amount of load they carry while working on scaffolds. Scaffolding should be designed so as to offer a solid footing for workers, be completely planked and away from any dangerous power lines. It is necessary that employers choose to work with the most suited ladder systems associated with the site of work. Workers should also be regularly trained about new ladder systems. Most construction workers in India come from rural areas looking for jobs. They are inexperienced and lack training in using safety gear. It is necessary that workers are chosen properly and that all are given the necessary training before being put on the job. Most of the time, workers are not informed or knowledgeable about the health and safety risks they are exposed to on construction sites. It is necessary that they are able to read and understand Material Safety Data Sheets and are prepared for the same. Implement safety programmes to ensure that workers understand the risk and are well prepared to face the challenges without risking their lives or health. Discouraging or prohibiting children from playing on fire escapes, roofs and balconies, especially those that are not adequately fenced with vertical bars and encouraging the use of ground-level safe play areas, such as public parks and playgrounds can reduce the number of incidents. At the same time, modernisation of physical environment and strict maintenance of safety procedures can protect vulnerable personnel and reduce economic burden. Triage must be done accurately at the accident location and critical patients should be referred to trauma centres quickly. This can reduce the mortality and morbidity due to falls from height.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Ethics Committee (IEC) of the college before commencing the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Not applicable.