
Abstract
Burn constitutes a major public health problem, especially in low or middle-income countries where over 95% of all burn deaths occur. According to the World Health Organisation, an estimated 1,95,000 deaths every year are caused by burns, the vast majority occur in low and middle-income countries. The present medico-legal study aimed to assess the cause of death and rate of survival related to different types of burn injuries. This autopsy-based descriptive study was carried out at the mortuary of People’s College of Medical Sciences & Research Centre (PCMS & RC), Bhopal, and Medico-legal Institute, Bhopal. Statistical analysis was done using chi-squared, Student’s t-test, and Kaplan-Meier for survival where applicable. Primary causes of death were reviewed from 125 autopsy reports. Percentages of patients that died from sepsis, hypovolemic shock or multi-organ failure were calculated by comparing to the total number of deaths. The period of Survival and Extent of Burns in burn victims is compared. Eight (6.4%) victims survived more than 10 days after sustaining burns, among them four victims having TBSA 50%–70%. Septicaemia is the leading cause of death after burn injury. Period of Survival was higher in 50%–70% of burn victims.
Introduction
Burn constitutes a major public health problem, especially in low or middle-income countries where over 95% of all burn deaths occur. 1 Fire-related burns alone account for over 3 lakh deaths per year. 2 However, deaths are only part of the problem, for every person who dies as a result of their burns; many more are left with lifelong disabilities and disfigurements. 2
According to the World Health Organisation, an estimated 1,95,000 deaths every year are caused by burns, the vast majority occur in low and middle-income countries. Non-fatal burn injuries are a leading cause of morbidity. 3
The causes of death in a burn victim 4 include: (a) Primary or neurogenic shock due to pain, sepsis, toxaemias, etc., (b) More than half of deaths from burns occur within the first 48 hours usually from secondary shock, due to fluid loss from the burned surface (Circulatory collapse may occur with 15% of burns of total body surface area [TBSA]). (c) Asphyxia is a result of oedema of the glottis and pulmonary oedema due to inhalation of smoke containing carbon mono-oxide and carbon di-oxide, if the person dies in a burnt house. In smoke inhalation apart from CO, the other factors that contribute to death are oxygen deprivation, cyanide, free radicles (inactivate surfactants, thus preventing oxygen from crossing the alveoli into the blood), and non-specific toxic substances, (d) Toxaemia, due to absorption of various metabolites from the burnt tissue persists up to three to four days, (e) Sepsis is the most important factor in deaths occurring four to five days or longer after burning. (f) Biochemical disturbances are secondary to fluid loss and destruction of tissue, such as hypokalaemia. (g) Acute Renal Failure, due to lower nephron nephrosis occurs on the third or fourth day. (h) Gastrointestinal disturbances, such as acute peptic ulcerations, dilation of the stomach, haemorrhage into intestine. (i) Oedema of glottis and pulmonary oedema due to inhalation of smoke containing CO and CO2, if the person dies in a burnt house. (j) Accident occurring in an attempt to escape from a burning house or by injuries due to falling masonry, timber or other structures on the body. (k) Pyaemia, gangrene, tetanus, etc. (l) Fat embolism is rare. (m) Pulmonary embolism from thrombosis of veins of the leg due to tissue damage and immobility. (n) Multisystem failure. (o) Death may occur years after recovery from the malignant transformation of a burn scar (Marjolin’s ulcer). 5
The magnitude of burn-related fatalities in India is alarming. In 2019, more than 23,000 fire-related deaths were estimated in India, which is about 20% of the global mortality burden. However, this is an underestimate as not all such deaths are reported. 6
Burns have got their individual place in medico-legal practice. A forensic expert has to face a number of questions in the Court of Law on medico-legal examination reports on burn cases. 7 A thorough and accurate examination and assessment of these cases are of utmost importance.
The medico-legal points that demand consideration in burn cases are whether the lesions found are due to burns, the nature of the agent causing burns, the area of burns over the body, the cause of death, whether they are antemortem or post-mortem in nature and whether burns are suicidal, homicidal or accidental. 1
The present medico-legal study aimed to assess the cause of death and rate of survival related to different types of burn injuries.
Material and Methods
This is an autopsy-based descriptive study carried out at the mortuary of People’s College of Medical Sciences & Research Centre (PCMS & RC), Bhopal, and Medico-legal Institute, Bhopal. The study was approved by the Institutional Ethical Committee.
The material for this study thus comprised all types of burn death cases brought to the mortuary of both places. A total of 125 autopsies were conducted to burn victims’ bodies, including deaths due to flame burns, contact burns, scalds, and electric burns. The inclusion criteria adopted were autopsies of burn victims’ dead bodies. The deaths due to causes other than burns and autopsies of decomposed bodies were excluded. The variables taken into account were age, sex, education, occupation, marital status, TBSA, causes of burn, pattern of burn, circumstances of burn injury, period of survival, etc.
Each case was allotted a serial number. The data for the study were collected from individual autopsies of all burn victims in a pre-designed proforma. The data thus collected from individual autopsies were further analysed using SPSS software version 20 and appropriate statistical tests.
Observation and Results
The present study includes a total of 125 autopsies of burn victims, brought to the mortuary of PCMS & RC, Bhopal, and Medico-legal Institute, Bhopal. All the observations were carefully documented from hospital case records, police inquest reports, history obtained from the relatives of the deceased, meticulous post-mortem examination, and Histo-pathology and Forensic Science Laboratory reports. The observations thus encountered of all this data are presented here in various tables and statistical diagrams for easy understanding and interpretation.
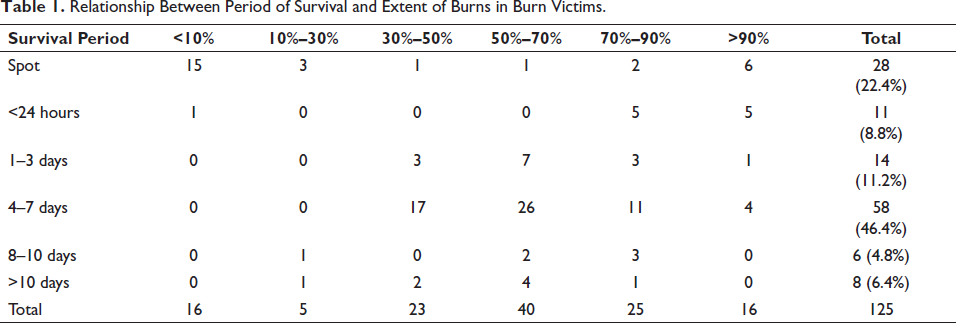
Relationship Between Period of Survival and Extent of Burns in Burn Victims
In the present study, it is found that the maximum number of burn victims (58%–46.4%) have survived from four to seven days, among these 58 burn victims, four had TBSA >90%. No victims had TBSA less than 30%, survived four to seven days.
Eleven (8.8%) victims died within 24 hours of sustaining burns, among them five victims had TBSA 70%–90%, five victims had TBSA more than 90% and only one victim had TBSA less than 10%. Eight (6.4%) victims survived more than 10 days after sustaining burns, among them four victims having TBSA 50%–70% (Table 1).
Relationship Between Period of Survival and Extent of Burns in Burn Victims.
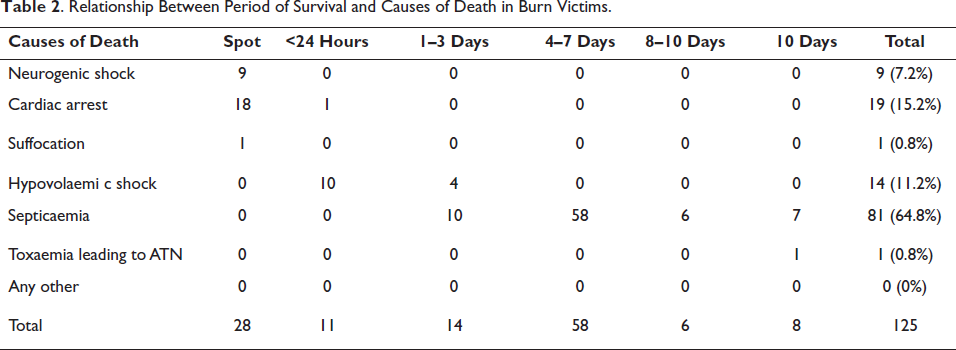
Relationship Between Period of Survival and Causes of Death in Burn Victims
The cause of death was septicaemia in maximum-81 (64.8%) victims, followed by cardiac arrest in 19 (15.2%), hypovolaemic shock in 14 (11.2%), neurogenic shock in 9 (7.2%), suffocation due to inhalation of fumes in 1 (0.8%), and acute tubular necrosis (ATN) in 1 (0.8%) victim (Table 2). Further in the study, it was found that the maximum (58) victims, who died due to septicaemia, survived four to seven days. Among 19 burn victims who died due to cardiac arrest, 18 died on the spot and one died within 24 hours of sustaining burns. Among 14 burn victims who died due to hypovolaemic shock, 10 victims died within 24 hours and four victims survived one to three days of sustaining burns. All nine burn victims of death due to neurogenic shock and only one victim, who died of suffocation due to inhalation of fumes, died on the spot. One victim of burns died due to ATN was survived for more than 10 days after sustaining burns (Table 2).
Relationship Between Period of Survival and Causes of Death in Burn Victims.
Discussion
Survival Period in Relation to Extent of Burns
Out of total 125 victims of death due to burns autopsied, maximum 58 (46.4%) victims had survived four to seven days, followed by 28 (22.4%) victims died on spot, 14 (11.2%) victims survived one to three days, 11 (8.8%) victims had survived less than 24 hours, 8 (6.4%) victims had survived more than 10 days, and 6 (4.8%) victims had survived 8–10 days after sustaining burns. Out of a total maximum of 58 (46.4%) victims, who survived four to seven days, the maximum was TBSA 50%–70% (26 victims), followed by TBSA 30%–50% (17 victims), TBSA 70%–90% (11 victims), and TBSA more than 90% (four victims). Out of total 28 (22.4%) victims, who died on spot, 15 (53.57%) were having TBSA less than 10% (electric burn cases), 6 (21.42%) having TBSA more than 90%, 3 (10.71%) having TBSA 10%–30%, 2 (7.14%) having TBSA 70%–90%, 1 (3.5%) having TBSA 30%–50%, and 1 (3.5%) having TBSA 50%–70%. Out of a total 14 (11.2%) victims, who survived one to three days, 7 (50%) were having TBSA 50%–70%, 3 (21.42%) were having TBSA 30%–50%, 3 (21.42%) were having TBSA 70%–90%, and 1 (7.14%) was having TBSA more than 90%. Out of a total of 11 (8.8%) victims, who survived less than 24 hours, 5 (45.45%) had TBSA 70%–90%, 5 (45.45%) had TBSA more than 90% and only one (9.09%) was having TBSA less than 10%. Out of total 8 (6.4%) victims survived more than 10 days, 4 (50%) were having TBSA 50%–70%, 2 (25%) were having TBSA 30%–50%, 1 (12.5%) was having TBSA 10%–30%, and 1 (12.5%) was having TBSA 70%–90%.
Out of total 6 (4.8%) victims, who survived 8–10 days, 3 (50%) had TBSA 70%–90%, 2 (33.33%) having TBSA 50%–70%, and only one (16.66%) victims was having TBSA 10%–30% as shown in Table 1. That means maximum number of victims-84 (67.2%), who were having extensive (more than 30%) burns had survived more than 1 day probably due to early availability of treatment, and they had died due to different causes, maximum-81 (64.8%) due to septicaemia. This is followed by 10 (8%) victims having extensive burns, who died before 24 hours of sustaining burns due to hypovolaemic shock, and 10 (8%) victims having extensive burns have died on the spot. Out of a total of 28 (22.4%) victims, who died on the spot, 18 (64.28%) had less than 30% burns, and 10 (35.71%) had more than 30% burns. The findings in relation to the survival period were consistent with the findings of Prakash I. Babladi et al. (1998–2002), 8 Sunil P. Tapse et al. (2008), 9 Anju Rani et al. (1998–2010) 10 and B.L. Chaudhary et al. (2006–2010). 11
Causes of Death in Relation to Survival Period
Out of a total of 125 deaths of burn victims autopsies, the cause of death in most of the cases (64.8%) was septicaemia, followed by 19 (15.2%) deaths due to cardiac arrest, 14 (11.2%) deaths due to hypovolaemic shock, 9 (7.2%) deaths were due to neurogenic shock, only one (0.8%) was due to suffocation as a result of inhalation of fumes, and one (0.8%) death was due to toxaemia leading to ATN. Out of a total of 28 on-spot deaths, the cause of death was cardiac arrest in 18 (64.28%), neurogenic shock in 9 (32.14%), and suffocation in only one (3.5%) victim. Out of a total 11 deaths of within an hour period, the cause of death was hypovolaemic shock in 10 (90.90%) and cardiac arrest in only one (9.09%) victims. Out of a total of 14 victims, who died in one to three days, the cause of death was septicaemia in 10 (71.42%), and hypovolaemic shock in 4 (28.57%) victims. Out of a total of 58 victims, who survived four to seven days, the cause of death was septicaemia in all (100%) cases. Out of a total of six victims, who survived eight to 10 days, the cause of death was septicaemia in all (100%) cases. Out of a total of eight victims, who survived for more than 10 days, the cause of death was septicaemia in 7 (87.5%), and toxaemia leading to ATN in only one (12.5%) victims, as shown in Table 2. Studies by other authors have observed similar results, the cause of death was septicaemia in the majority of cases in the study of Prakash I. Babladi et al. (1998–2002),8 Dr Mrs S. Dhillon et al. (1999–2003), 12 Anju Rani et al. (1998–2010),10 B.L. Chaudhary et al. (2006–2010),11 and Harish D et al. (2011–2013). 13
Conclusions
Septicaemia is the leading cause of death after burn injury. Period of survival was higher in 50%–70% of burn victims.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethical Committee, People’s College of Medical Sciences and Research Centre, Bhopal (Reference number: PCMS/OD/2013/3808).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.