
Abstract
Among the frequent congenital anomalies of teeth, the labio-cervical vertical groove (LCVG) is a rare congenital morphological anomaly of teeth. The science of forensic dentistry has valuable contributions to assist in personal identification, syndromic correlation of congenital diseases, victim search after a mass disaster by ensuring faster and scientific information from recorded secure past data to compare it with the present one. Infolding of an enamel organ and Hertwig’s epithelial root sheath can create a vertical groove on the labial surface of permanent maxillary incisors extending from crown to root. A 47-year-old male patient, came to a private clinic with a complaint of bleeding from gums. On clinical examination, generalized mild gingival inflammation and vertical groove along with mild gingival irregularity were found on the labial surface of 21. The present case shows mamelon remnants extension with LCVG in 21 in the patient and his mother.
Keywords
Introduction
The labio-cervical vertical groove (LCVG) is a unilateral or bilateral structural malformation in which infolding of the enamel organ and Hertwig’s epithelial root sheath create a groove on the permanent maxillary incisors.1–6 LCVG is a type of cementoenamel defect like palato-radicular groove and cervical enamel projection. 7 Different studies in past had described LCVG as a notch.1–4 It appears as a shallow vertical enamel depression to deep groove,1, 8, 9 which can be mild, moderate or severe type based on its extent and depth. 5 Etiology includes trauma to the developing tooth bud via primary teeth injury,1, 3, 8, 10 vertical extension of the mamelon groove,4, 5, 11 environmental, nutritional, infection or genetic.2, 5, 12 This article reports, a unilateral labio-gingival groove on tooth 21 in a 42-year-old male and his mother, to consider defect occurrence was due to vertical extension of the mamelon grooves.5, 12
Case Report
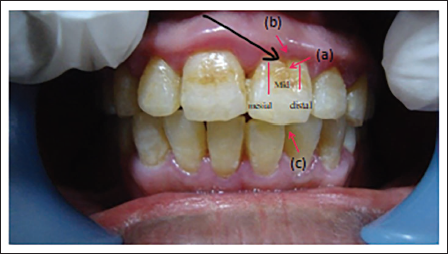
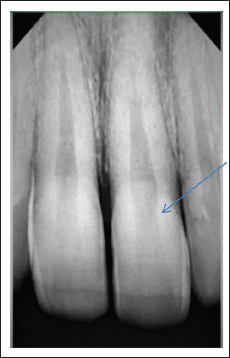
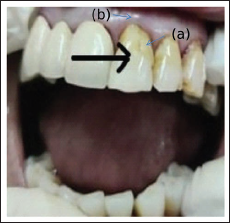
A 47-year-old male patient came with a complaint of gingival bleeding. On clinical examination, generalized mild gingival inflammation was present. Abnormal gingival contour and vertical groove were present in relation to the labial surface of 21 (Figure 1). Careful intraoral examination revealed a deep vertical groove on the labial surface of 21 of patients with mamelons remnant on incisal age and mild change in gingival contour. An intraoral periapical radiograph (IOPA) of patient revealed mild linear abrupt radiolucency up to cervical one-third of radicular part of 21 (Figure 2) Same defect of mild form was also observed in patient’s mother, aged 72 years (Figure 3). There was no past history of trauma to the primary teeth and non-contributory medical history. Scaling along with deep curettage of localized areas the treatment of choice, was done. An explanation of care to be taken for a particular deformity was discussed till patient’s satisfaction. Regular periodic follow-up and cleaning were suggested as a preventive measure.
Labio-cervical Vertical Groove: Male Patient with a Permanent Maxillary Left Central Incisor (Tooth #21 According to the FDI Tooth Numbering System). (a) A Deep Vertical Groove (Severe Form) in the Mid-cervical Region of the Tooth Crown, Abruptly Merging with the Tooth Convexity. (B) Abnormal Gingival Contour with Reddish Gingival Margins. (c) Mamelon Remnants.
Intraoral Periapical Radiograph (IOPA): Abrupt and Notched Pulp Canal, Correlates with the Clinical Defect as a Labio-Cervical Vertical Groove.
Labio-Cervical Vertical Groove: Female Patient, in Permanent Maxillary Left Central Incisor Tooth 21. (a) A Shallow Vertical Groove (Mild Form) in the Mid-part of the Cervical Region Of The Tooth Crown. (b) Mild Inflamed Gingival Margin and Calculus.
Discussion
LCVG is a congenital morphological anomaly of an enamel, 1 in which an infolding of the inner enamel epithelium and Hertwig’s epithelial root sheath create a groove, extending to varying depth in the root,1–6 found at the labio-cervical surface of the permanent maxillary central incisors.1–7 It is a 3rd type of cementoenamel defect similar to palato-radicular groove on permanent maxillary lateral incisors and cervical enamel projection as enamel pearls in the furcation areas of maxillary and mandibular molars.2, 7 Gingival contour is normal in shallow enamel depression, whereas it is irregular1, 8, 9 and shows a breach in gingival attachment as a deep groove. 2 Radicular extension of LCVG can be mild, moderate or deep based on its extent and depth.1, 5 Brin and Ben-Bassat (1989, 2001) 10 have observed that LCVG is associated with single or multiple incisor teeth involvement. According to past studies, deep grooves were observed predominantly in males and involving the left central incisors. Mass et al. 5 have categorized groove into three stages, that is, (a) a mild subgingival shallow groove below the marginal gingiva that can be felt only by probing. (b) A moderate groove that can be detected with the eyes extends subgingivally as in (a), and additionally supragingivally on the labial crown surface, not more than 2 mm from the marginal gingiva in the incisal direction and (c) a severe defect which extends supragingivally more than 2 mm from the marginal gingiva on the labial crown surface and further subgingivally. According to the severity ranked by Mass et al., in our case, it is a moderate type with mild gingival contour deformity in the patient and only gingival recession in his mother’s case. Different studies in the past have described it as a notch.2–4, 11 The etiology is thought to be trauma to developing tooth bud, 2 vertical extensions of mamelon groove,2, 6 genetics, environmental and nutritional factors. Damage to the ameloblasts, enamel organ and Hertwig’s epithelial root sheath with impaired function causing gingival, periodontal, aesthetic and prosthetic concern.12–15 Teams of specialists from different fields such as Law enforcement departments, Pathologists, Odontologists and Anthropologists, Knowledge and evidence from dental specialists are unique to guide for positive outcome of individual identification. 16 The present case noticed a vertical groove on 21, which are remnants of mamelon groove extension in the patient and his mother. Suggestive treatment includes the elimination of grooves by gingival curettage, saucerization and restorative fillings, whereas, in hopeless teeth, extraction is recommended. 2 In the present case, we performed deep curettage only to resolve a complaint and advised to keep follow-up at regular intervals of time.
Conclusion
Abnormal tooth morphology may be a systemic indicator of developmental problems. Accurate diagnosis, elimination of inflammation and periodic follow-up are key factors to achieving favourable results. Early detection and prompt treatment of defects minimize plaque accumulation, caries, gingival inflammation and periodontal problems. Further studies can include screening of more family members to understand the underlying genetic correlation.
Footnotes
Acknowledgement
I acknowledge my deep sense of gratitude to my guide Mr Rami Kamlesh B. for encouraging guidance and kind supervision. I am also thankful to Dr Kunal Thakkar for his support in providing data along with good photographs of both patients and my nephew Harshil Mehta for support in editing and writing. Their deep thoughts, knowledge and immense support have created an opportunity for me to present this case at its best.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed written consent were obtained from the patients.