
Abstract
Background
Contemporary nursing practice involves increasing complexity, time pressure, and organisational demands that require rapid judgement. Nurses are also expected to address the vulnerability of patients and families while maintaining dignity. Ethical tensions often occur when institutional expectations, professional responsibilities, and personal conscience do not fully align. Although conscience is recognised as an important ethical resource in nursing, little is known about how it is experienced in everyday clinical practice.
Aim
This study aimed to examine conscientious pauses experienced by nurses in Japanese nursing practice and to analyse how harmony is experienced and reconfigured during these ethical moments.
Research design
A thematic narrative analysis explored nurses’ ethical experiences in everyday practice.
Participants and research context
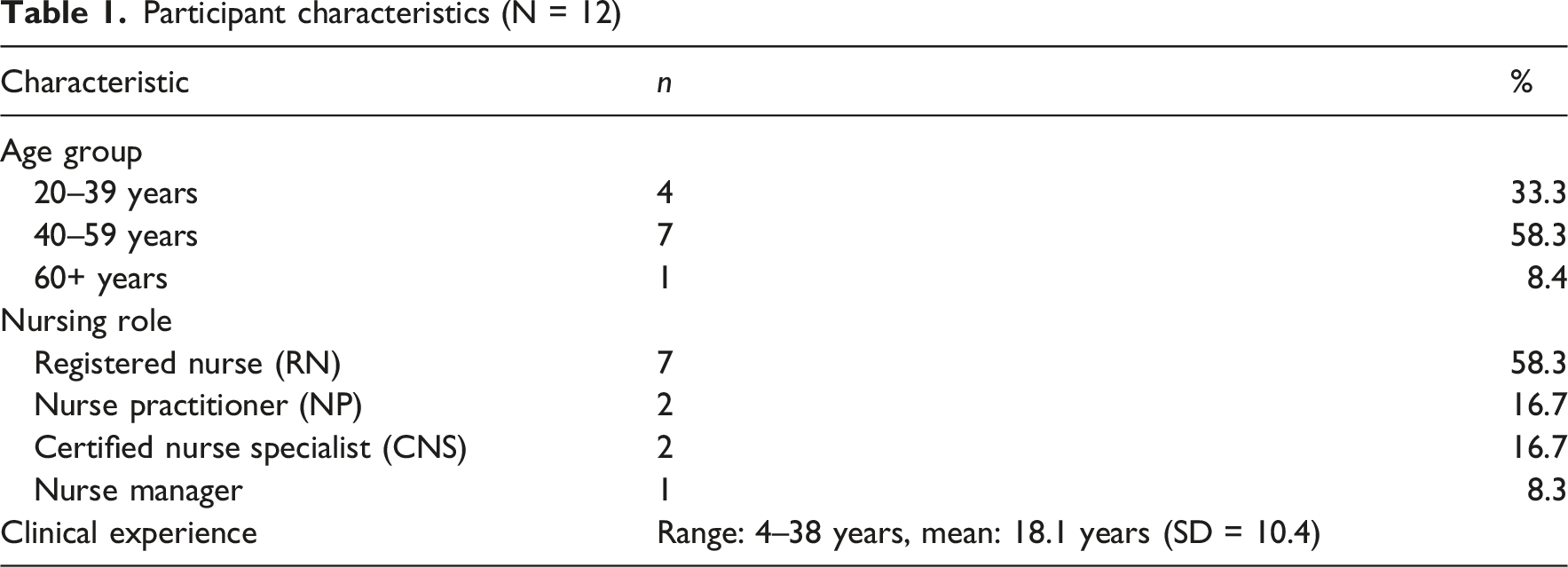
Twelve nurses working in healthcare institutions in Japan participated in the study.
Ethical considerations
Ethical approval was obtained from the relevant ethics committee, and all participants provided informed consent.
Findings
Conscientious pauses occurred in several ways: as deliberate hesitation to avoid premature judgement, as relationally sensitive actions to maintain harmony, as engagement with organisational and institutional tensions, and as ongoing processes of meaning-making over time. These pauses were not limited to specific clinical domains and often appeared as sensitivity to unspoken vulnerability rather than explicit ethical claims. Harmony was experienced not as a fixed value but as a relational condition negotiated and reconfigured through practice.
Conclusions
Conscientious pauses are relational and temporal ethical practices that enable nurses to address vulnerability in daily care. By viewing ethics as lived experience rather than solely as decision outcomes, this study emphasises the need to recognise and support conscientious pauses as shared ethical moments in nursing practice.
Introduction
This study explores how nurses experience ethical moments in everyday practice, focusing on the concepts of conscientious pauses and harmony. By adopting a narrative approach, it examines how ethical reflection emerges within ongoing care and how these experiences are interpreted in relational contexts. The study aims to contribute to a deeper understanding of ethics as lived experience in nursing practice.
The paper begins by establishing the theoretical background, followed by an analysis of nurses’ narratives, and concludes with a discussion of the organisational frameworks needed to support these ethical moments.
Background
Contemporary nursing practice occurs in increasingly complex healthcare environments with technological advancement, time constraints, and greater organisational demands.1–4 Nurses often make judgements in uncertain conditions while providing care that respects the vulnerability and dignity of patients and families.5–11
In these contexts, pressure for efficiency and institutional compliance can create ethical tensions when professional responsibilities,12–14 organisational expectations, 15 patients’ values, 16 and nurses’ own conscience do not fully align. 17 Nursing judgement is rarely the result of completely autonomous individual choice; instead, it develops within relationships involving patients, colleagues, and organisations.18–21 International nursing ethics research consistently shows that these conditions lead to ethical conflict and moral distress. 22
Philosophical and psychological discussions indicate that conscience is not a single, unified concept but has been interpreted in various ways across historical and theoretical traditions. 23 Conscience has been described as a capacity for moral self-reflection, a source of moral knowledge, a motivational force, or a means of self-evaluation. 24 Rather than serving as a mechanism that guarantees correct action, conscience is often viewed as a reflective capacity that initiates ethical questioning and deliberation. 23 This understanding resonates with nursing practice, in which ethical concerns frequently emerge not as clear decisions but as moments of uncertainty and reflection in the context of ongoing care.
Conscience has long been recognised in the nursing ethics literature as an important element supporting ethical practice.17,25–30 A recent systematic review by Lamb et al. 31 identifies conscience as a key internal resource for healthcare professionals in ethically challenging situations but also notes limited empirical knowledge about how conscience is understood and experienced in everyday clinical practice. From a care ethics perspective, conscience is not only an internal belief or psychological resource but also a form of sensitivity and responsiveness to the vulnerability of others that develops within practice. 9 However, empirical studies exploring conscience in this relational and experiential sense are limited.26,29,32,33 Consequently, discussions of conscience in nursing ethics often remain abstract or normatively framed, with little empirical research on how nurses experience conscience in daily clinical practice. 30 This lack of empirical research creates a gap in understanding how conscience is enacted and experienced in the realities of clinical nursing work, especially in relation to everyday ethical moments. This study addresses this gap by focusing on the lived experiences of nurses and examining how conscientious pauses and harmony are negotiated in practice.
Internationally, nursing codes of ethics and professional guidelines in several countries explicitly reference conscience and conscientious objection (CO), positioning it as part of professional ethics rather than only a matter of personal belief.34–37 However, other authors emphasise that conscientious objection is also grounded in the personal values and beliefs of the individual. 31 Research on CO has largely focused on ethically extreme situations, such as abortion or end-of-life care, in which moral conflict becomes explicit and unavoidable.38–43 In contrast, Japan lacks formal guidelines that clearly define or institutionally support conscience in nursing practice. 44 As a result, conscience is often addressed implicitly through individual judgement and negotiation with patients, colleagues, and organisations, indicating that it is less regulated by formal frameworks and more embedded in everyday relational practice. 45
Much of the existing nursing ethics literature addresses ethical decision-making models, outcomes of moral judgement, and the psychological impact of ethical conflict. 46 However, in contexts in which the right to conscientious objection is not formally recognised or protected within institutional frameworks, ethics may be experienced less as a formal decision-making process and more as moments of uncertainty, hesitation, and reflection within practice. These experiences cannot be fully captured by applying principles or rules alone.7,47
In everyday nursing practice, ethical decision-making may take the form of an internal deliberative process embedded within ongoing care, particularly in situations that generate unease or uncertainty.48–50 In this study, these ethical moments are conceptualised as conscientious pauses, defined as temporary adjustments in judgement that enable nurses to reorient their practice and address vulnerability without stopping action. 45 This concept differs from hesitation or reflection in that it is not merely a passive delay or internal cognitive process, but an active, relational, and embodied response that occurs within ongoing practice. In nursing research, harmony is identified as a valued relational concept that shapes practice, 51 while Japanese nursing ethics research highlights its ambivalent nature: harmony can support collaboration and mutual respect, but it may also create ethical tension by encouraging conformity or limiting professional judgement. 52 This conceptualisation of harmony aligns with relational and culturally situated ethical perspectives that emphasise interdependence, respect, and relational attunement in practice.
Although both conscience and harmony have been discussed in nursing ethics,31,51,52 little is known about how nurses experience and reinterpret harmony when they pause in response to conscience. These ethical experiences occur within relational and temporal contexts. In this study, ‘ethical tensions’ refers to situations of unease or uncertainty experienced in practice,53,54 whereas ‘ethical problems’ refers to more clearly defined ethical dilemmas discussed in the literature.55,56, Therefore, a narrative approach is suitable for exploring how nurses understand ethical tensions over time.57,58
The aim of this study was to explore conscientious pauses experienced by nurses in Japanese nursing practice and to examine how harmony is experienced, interpreted, and reconfigured during these moments through narrative analysis of nurses’ accounts. This study seeks to complement principle-based approaches to ethics and deepen understanding of ethics as experienced in everyday nursing practice.
Research question
This study considered the following research questions: 1. How do nurses experience conscientious pauses in their nursing practice? 2. How is harmony interpreted and reconfigured within these experiences?
Methods
Study design
This study used a qualitative research design to examine how nurses experience conscientious pauses in daily practice and how the meanings of harmony are negotiated and reconfigured during these moments.
Ethical experiences in nursing practice arise not only from decision-making but also from processes of meaning-making within temporal and relational contexts. 59 Therefore, this study used a narrative approach to examine how nurses interpret ethical moments through their stories. 58 This approach was operationalised through thematic narrative analysis. 58
Participant recruitment and characteristics
Participants were registered nurses employed in healthcare institutions in Japan and were recruited through purposive and snowball sampling. Inclusion criteria were as follows: (1) at least 3 years of clinical nursing experience; (2) self-identification of having experienced ethical uncertainty, hesitation, or conflict in everyday practice; and (3) willingness to participate and reflect on these experiences in narrative interviews.
To prevent overrepresentation of particular clinical domains or career stages, the sampling strategy ensured diversity in years of clinical experience, work settings, and employment arrangements. This approach aimed to capture a wide range of conscientious pauses across various clinical contexts rather than concentrating on a single speciality area.
Data collection procedures
Data were collected through semi-structured narrative interviews guided by an interview schedule developed specifically for this study. Each interview began by inviting participants to describe situations in their everyday practice in which they experienced uncertainty, hesitation, or discomfort. Participants were encouraged to recall specific scenes and interactions.
Participants were then asked to reflect on moments when they felt that they had paused while continuing to act, identifying instances in which they sensed a need to slow down, reconsider, or recalibrate their actions. They were encouraged to describe their thoughts, bodily sensations, and emotions as well as the nature of their hesitation. Participants were also asked how these pauses affected their subsequent actions, judgements, or interactions.
Further questions examined what participants aimed to protect or value in those moments, including considerations related to patients, families, professional responsibilities, colleagues, and organisational expectations. The study also considered how participants experienced relationships with patients, coworkers, and other professionals during these times.
Finally, participants were asked to consider how they understood these experiences over time, including whether and how the meanings changed in their later practice or self-understanding.
No predefined ethical concepts or terminology were introduced during the interviews. The researchers prioritised participants’ own words and narrative flow, adapting questions flexibly to follow each participant’s story. Each participant was interviewed once for approximately 60–90 min. With consent, interviews were audio-recorded, transcribed verbatim, and used as analytic material.
Data analysis
Analytic approach
Data were analysed using thematic narrative analysis as described by Riessman. 58 Narratives were considered as sites where participants actively constructed meaning, ethical positioning, and orientations toward practice rather than as objective representations of events.
The analysis focused on the content of the narratives rather than their structure. The study paid particular attention to expressions of hesitation, ambivalence, discomfort, delayed judgement, and relational adjustment, as these moments were considered indicative of conscientious pauses. Interpretation focused on how participants constructed meaning through their narratives, including how they positioned themselves ethically and made sense of their actions over time.
Analytic procedure
The analysis maintained theoretical sensitivity to moments of hesitation and relational attunement, avoiding the imposition of predefined categories. 58
Transcripts were read multiple times to gain an overall understanding of each participant’s narrative trajectory. Instances of ethical uncertainty, hesitation, or discomfort were identified, with attention to the triggers of conscientious pauses and the relational contexts in which they occurred.
Narratives were examined in temporal order, focusing on how participants evaluated and reinterpreted their experiences before, during, and after the pause. Narratives were then compared across participants to identify commonalities and variations, which led to the generation of themes and subthemes.
Throughout the analytic process, researchers continually checked emerging interpretations against the original transcripts to ensure coherence with the narrative context and to avoid decontextualised abstraction.
Sensitising concepts
Two sensitising concepts guided the analysis: Conscientious pause and harmony. A conscientious pause refers to a process in which nurses temporarily slow their actions while continuing to work, reassess the situation based on their conscience, and adjust their ethical stance and practical approach. This concept was not considered a fixed behavioural category or decision rule; instead, it was examined inductively as it emerged in participants’ narratives.
Harmony referred to nurses’ experiences of relational and environmental attunement in practice, encompassing moments of stability, tension, disruption, and reconfiguration. These concepts did not constrain the analysis but acted as interpretive lenses, which were refined through engagement with the data.
Ensuring rigour and trustworthiness
Several strategies were used to enhance the trustworthiness of the analysis.60,61 Interpretations were based on explicit excerpts from transcripts to avoid reliance on researchers’ assumptions. Generated themes were repeatedly examined in relation to the narrative context to ensure analytic coherence. In addition, member checking was undertaken by sharing selected narrative interpretations with participants, who were invited to comment on the resonance and factual accuracy of the accounts.
Ongoing discussions with qualitative researchers experienced in nursing ethics critically examined analytic decisions and identified potential biases or blind spots. Analytic memos documenting coding decisions, theme development, and reflexive considerations were maintained to ensure transparency and auditability of the analytic process. The sample size was considered appropriate for narrative research, as the study prioritised depth of individual accounts and the richness of narrative data.
Ethical considerations
The institutional ethics review board of the authors’ affiliated institution approved this study. Participants received oral and written information about the study purpose, procedures, voluntary participation, right to withdraw without penalty, and measures to ensure confidentiality and anonymisation. All participants provided written informed consent.
Given the ethically sensitive nature of discussing hesitation and moral conflict in practice, particular care was taken to minimise psychological burden. Participants were informed that they could pause, modify, or terminate the interview at any time. All identifying information was removed or pseudonymised during transcription, and data were securely stored in password-protected files.
Findings
Participant demographics
Participant characteristics (N = 12)
Overview of findings
Analysis of the narratives showed that conscientious pauses experienced by nurses in clinical practice did not follow a single, uniform pattern. Instead, they took several forms: deliberate hesitation to avoid premature judgement, actions intended to preserve relationships, engagement with institutional or organisational tension, and ongoing processes of meaning-making that continued after practice.
Themes, subthemes, and codes of conscientious pauses in nursing practice.
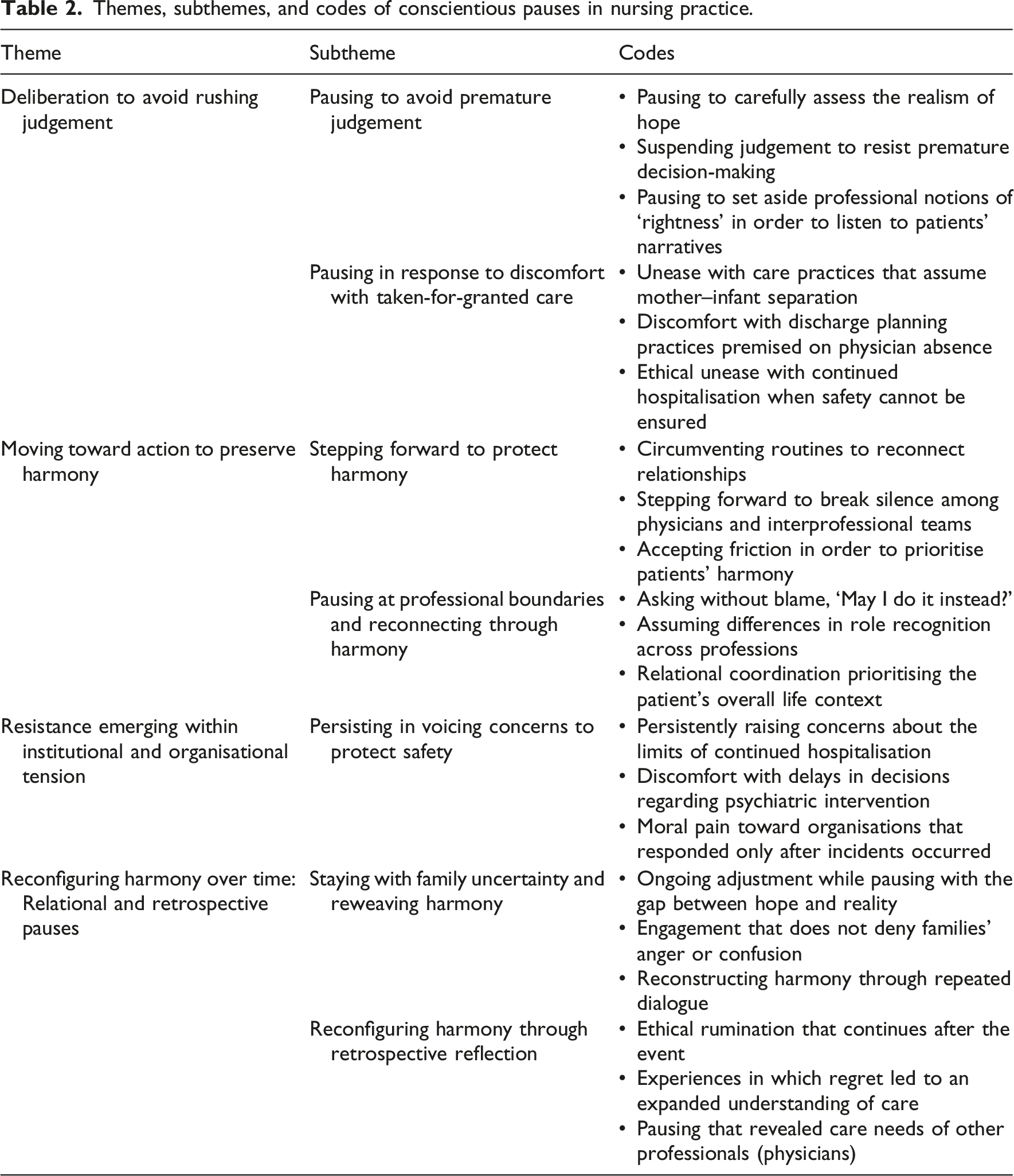
Theme 1: Deliberative pauses to avoid premature judgement
In this pattern, nurses reported intentionally refraining from making immediate decisions or taking action. Instead of responding automatically, they paused to consider multiple possibilities and potential consequences.
Subtheme 1: Pausing to avoid premature judgement
Nurses reported withholding judgement when patients’ wishes, family expectations, clinical realities, and prognostic uncertainty converged. Rather than immediately applying what was considered professionally appropriate based on clinical judgement, ethical standards, and experience, they paused to listen to patients and families and considered what might be possible.
One nurse explained as follows: If the patient or the family even slightly expressed a wish to go home, I felt we could take some time to examine whether that was realistically possible. After actually asking and understanding whether it was possible or not, then, if it truly wasn’t, that might be unavoidable. But if there was a chance, I felt we needed to consider it. (Nurse A, ward nurse)
Another nurse reflected on a highly acute situation: I was almost certain the patient would go into cardiac arrest during the flight. That’s why I begged the doctor to take the husband with us, saying I could stay behind. I kept thinking about what would be best for this person, even though I believed the outcome was almost inevitable. (Nurse B, flight nurse)
In these narratives, conscientious pauses were not passive delays but intentional ethical deliberations intended to re-examine the situation from multiple perspectives.
Subtheme 2: Pausing in response to discomfort with routine practice
This pattern also included instances in which nurses paused due to discomfort with care practices that had become routine in daily work. Even without an obvious alternative, nurses questioned whether these established routines were ethically acceptable. In a setting where separating mothers and infants was treated as the norm, I kept feeling uncomfortable, wondering whether that was really okay. (Nurse C, operating room nurse)
Another nurse described a similar sense of unease: I was told that it was normal for physicians not to attend conferences here, but it kept bothering me. I felt it was disrespectful to the patient. (Nurse D, discharge planning nurse)
These narratives show that conscientious pauses are moments of ethical questioning, during which nurses resisted uncritical acceptance of routine practices.
Theme 2: Relational action to preserve harmony
In the second pattern, nurses described situations in which pausing resulted in taking minimal and carefully calibrated action – rather than withdrawing – to preserve relationships.
Subtheme 1: Stepping forward to maintain harmony
Nurses reported carefully selecting their words and actions when they believed that ignoring a situation could harm relationships. Instead of directly confronting others, they aimed to maintain harmony while continuing to address patients’ needs. I felt uneasy about the doctor not coming, so when the home-care physician was scheduled to visit, I always made sure to bring the hospital doctor along. If I confronted them directly, it might have caused conflict, so I framed it as something necessary for the patient. (Nurse F, discharge planning nurse)
Here, the pause enabled nurses to navigate between ethical concern and relational preservation.
Subtheme 2: Navigating professional boundaries through harmony
Nurses reported adjusting their relationships with other professionals by recognising role boundaries and avoiding blame or confrontation. I wanted to ask why they hadn’t done it, but instead, I said, ‘Would it be okay if I did it?’ If I had argued about whose job it was, it would have caused conflict, so I decided to take it on myself. (Nurse G, outpatient nurse)
In these narratives, conscientious pauses served as relational adjustments that allowed continued collaboration without increasing tension.
Theme 3: Navigating institutional and organisational tensions
In the third pattern, nurses described conscientious pauses that were limited, dismissed, or reluctantly accepted within institutional and organisational structures.
Subtheme 1: Persisting in voicing concerns for safety
Nurses reported raising concerns multiple times in situations in which it was not possible to ensure the safety of the patient, other patients, and staff at the same time. However, organisational decisions did not always reflect these concerns. I kept saying that we couldn’t protect the safety of the patient, other patients, and the staff at the same time. I kept raising my voice over and over, but it didn’t immediately change the organisational decision. (Nurse H, ward nurse)
These accounts present conscientious pauses as moments when ethical tension between care values and institutional priorities became apparent.
Theme 4: Reconfiguring harmony over time
In the fourth pattern, conscientious pauses extended beyond the immediate clinical situation and continued over time through reflection, reinterpretation, and relational reconfiguration.
Subtheme 1: Sustaining engagement with family uncertainty
Nurses reported staying with families as they tried to balance hope and reality, avoiding the temptation to draw conclusions too soon. There was a huge gap between what the husband believed was possible and the reality we were seeing. I felt we shouldn’t deny his feelings. We kept discussing the situation over and over, trying to figure out together what would be best. (Nurse I, ward nurse)
Here, harmony was maintained through ongoing engagement rather than resolution.
Subtheme 2: Reflective reconfiguration of harmony
Nurses reported that they continued to reflect on their experiences after practice, often experiencing regret or ongoing discomfort. Over time, these reflections changed their understanding of care and professional relationships. I deeply regretted that the family couldn’t be there in the patient’s final moment. Later, when I entered a CNS programme, I realised for the first time how difficult the decision must have been for the doctor as well. (Nurse B, flight nurse)
These narratives show that conscientious pauses are ongoing ethical processes that reshape meanings and relationships over time.
Overall, conscientious pauses occurred in several forms: as purposeful ethical deliberation, as relationally sensitive action, as engagement with institutional tension, and as ongoing processes of meaning-making that developed over time. These findings show that conscientious pauses are not isolated moments of hesitation but dynamic ethical practices situated within relationships, organisational contexts, and the temporal progression of nursing practice.
Discussion
This section examines how the study’s findings address the research questions: first, how nurses experience conscientious pauses in their nursing practice, and second, how harmony is interpreted and reconfigured within these experiences. The findings show that the conscientious pause nurses experience is not simply a delay in decision-making or an act of caution. Instead, it represents ethical deliberation intended to protect the vulnerability of patients, families, and healthcare providers from irreversible harm. This interpretation is consistent with nursing ethics research, which suggests that ethical judgement begins with ‘awareness’ or the ‘direction of attention’ before actions are chosen. For example, Nielsby et al. report that when nurses encounter ethical challenges, ethical awareness and attentional orientation come before judgement and choice, forming the basis of clinical decision-making. 62 Similarly, Gastmans et al. highlight sensitivity and attentiveness to the vulnerability of others and situations as essential qualities of morally competent nurses, placing greater value on these qualities than on normative judgement abilities. 63 These perspectives together present ethics not as the result of decision-making but as a responsive posture that arises in the early stages of practice.
Crucially, these pauses did not occur because ‘there was ample time’. Instead, they arise when nurses recognise the vulnerability present in relational dynamics within practice and feel a responsibility to respond. In this context, the conscientious pause aligns with care ethics discourse, which views ethical action not as an individual rational calculation, but as a responsibility to respond that emerges within relationships.9,64
The narratives show that conscientious pauses occur across various clinical domains, not only in areas such as end-of-life care or acute medicine. This finding supports the perspective of everyday ethics, 65 which holds that ethics emerge within routine practice rather than only in exceptional situations. This perspective supports the view that conscientious pauses are a cross-cutting ethical practice embedded in everyday nursing work.
From this viewpoint, conscientious pausing reveals ethical dimensions of nursing practice that extend beyond professional boundaries. The ability to pause, attend, and respond to another’s vulnerability may indicate ethical sensitivity within human relationships66,67 rather than a competence restricted to specific professional skills. However, because this study is based on nurses’ narratives, further empirical research is needed to assess the extent of this universality.
Furthermore, in the nurses’ narratives, conscientious pauses appeared not as explicit statements or demands but as inarticulate feelings of unease or hesitation. This indicates that the ethical pause is a practice of confronting ‘unspoken vulnerability’, whether that of patients, families, or healthcare providers. 68 These responses are best understood as ethical experiences embedded in practice, which conventional decision-making models or rule-based ethical frameworks cannot fully capture.
Conscientious pauses were not limited to individual nurses’ internal experiences; they also served as moments that made organisational values and judgement criteria visible. When these pauses occurred, tensions emerged between organisational demands for efficiency and speed and care values focused on protecting vulnerability and dignity. The meaning of these pauses was not immediately determined; instead, they were experienced as processes that reorganised relationships and harmony over time.
Taken together, these findings indicate that conscientious pauses should not rely solely on individual virtue or personal conscience. They should be recognised, shared, and supported as essential ethical moments within nursing practice. In the Japanese nursing context, where the right to conscientious objection lacks explicit institutional recognition and nurses often carry ethical burdens within relational settings, it is crucial to establish organisational and relational frameworks. Such frameworks are essential to prevent conscientious pauses from being reduced to isolated, individual burdens.
Limitations
Several limitations of this study should be acknowledged. First, the findings are based on narratives from a relatively small number of nurses working in healthcare institutions in Japan. Therefore, the results reflect a specific cultural, organisational, and professional context. Although the findings may provide insights relevant to other settings, they are not intended to be statistically generalisable.
Second, this study relied on participants’ retrospective narratives of ethical experiences. Although narrative analysis is appropriate for examining how meaning develops over time, participants’ accounts may have been affected by memory, reflection, and later experiences. Therefore, the narratives reflect how nurses understood conscientious pauses rather than providing objective reconstructions of past events.
Third, the analysis used the sensitising concepts of conscientious pause and harmony. These concepts were applied flexibly and refined through engagement with the data, which may have influenced the interpretive focus of the analysis. Consequently, other ethical dimensions of nursing practice may exist that were not fully captured within this conceptual framework.
Conclusion
This study examined conscientious pauses as experienced by nurses in everyday clinical practice and explored how harmony is experienced and reconfigured through these ethical moments. Analysis of nurses’ narratives showed that conscientious pauses are not simply delays in decision-making or expressions of individual caution but relational and temporal ethical practices through which nurses address vulnerability and protect dignity within complex clinical and organisational contexts.
The findings show that conscientious pauses occur not due to available time for deliberation but because nurses recognise vulnerability within relationships. Observed in various clinical settings, these pauses represent a consistent ethical practice in nursing and often appear as sensitivity to unspoken vulnerability rather than explicit ethical claims. As a result, they remain mostly invisible within principle-based or decision-focused ethical frameworks.
Furthermore, conscientious pauses were not limited to isolated moments; their meanings developed over time through reflection and changes in relationships and harmony while also revealing organisational values and tensions. These findings together reconceptualise conscience as a shared ethical capacity expressed within practice rather than as an individual moral attribute. In contexts such as Japan, where conscience is not explicitly institutionalised, organisational and relational frameworks are necessary to recognise and support these ethical moments. This approach complements dominant ethical models by highlighting lived ethics in everyday nursing practice.
Footnotes
Acknowledgements
The author wishes to express sincere gratitude to the participating nurses who generously shared their experiences. The author is also grateful to Professor Chris Gastmans for his inspiring lectures and valuable insights, to Karen Klotz for her helpful comments on parts of the results, to Carlos Gomez-Virseda for his thoughtful reflections, and to the participants of the KU Leuven Nursing Ethics Seminar 2025 for their valuable discussions, which contributed to the development of this research.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI Grant-in-Aid for Scientific Research (C) [Grant Number: 24K13670], and by the Grant-in-Aid for Fostering Young Researchers from the Japan Academy of Nursing Science.
Declaration of conflicting interests
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to the sensitive and narrative nature of the interviews. Anonymised excerpts may be shared upon reasonable request to the corresponding author, subject to ethical approval.
Identifiable Information Statement
No identifying information regarding participants, institutions, funding bodies, or ethical review committees is disclosed in the manuscript. All details have been anonymised to protect confidentiality in line with ethical research practices.