
Abstract
Background
Nurses frequently encounter ethical dilemmas, moral distress, and situations in which they must balance professional duties, personal values, and organizational constraints. Deontological ethics, particularly Kant’s ethics of duty, offers a normative framework that emphasizes moral action grounded in duty rather than consequences. However, limited empirical research explores how nurses understand and enact Kantian principles in everyday clinical practice.
Research aim
To explore how nurses understand and enact principles of Kant’s ethics of duty in clinical decision-making and how this philosophical framework shapes their moral judgement, sense of duty, and professional integrity.
Research design
A qualitative descriptive research design.
Participants and research context
Between November and December 2025, 17 nurses were recruited from various clinical settings in Slovenia through purposive sampling. Data were collected through semi-structured in-person interviews focused on moral decision-making, professional duty, moral autonomy, and institutional constraints. Braun and Clarke’s thematic analysis approach was employed to analyze the data.
Ethical considerations
The study was approved by the university ethics committee. Participation was voluntary and anonymous, and written informed consent was obtained from all participants.
Findings
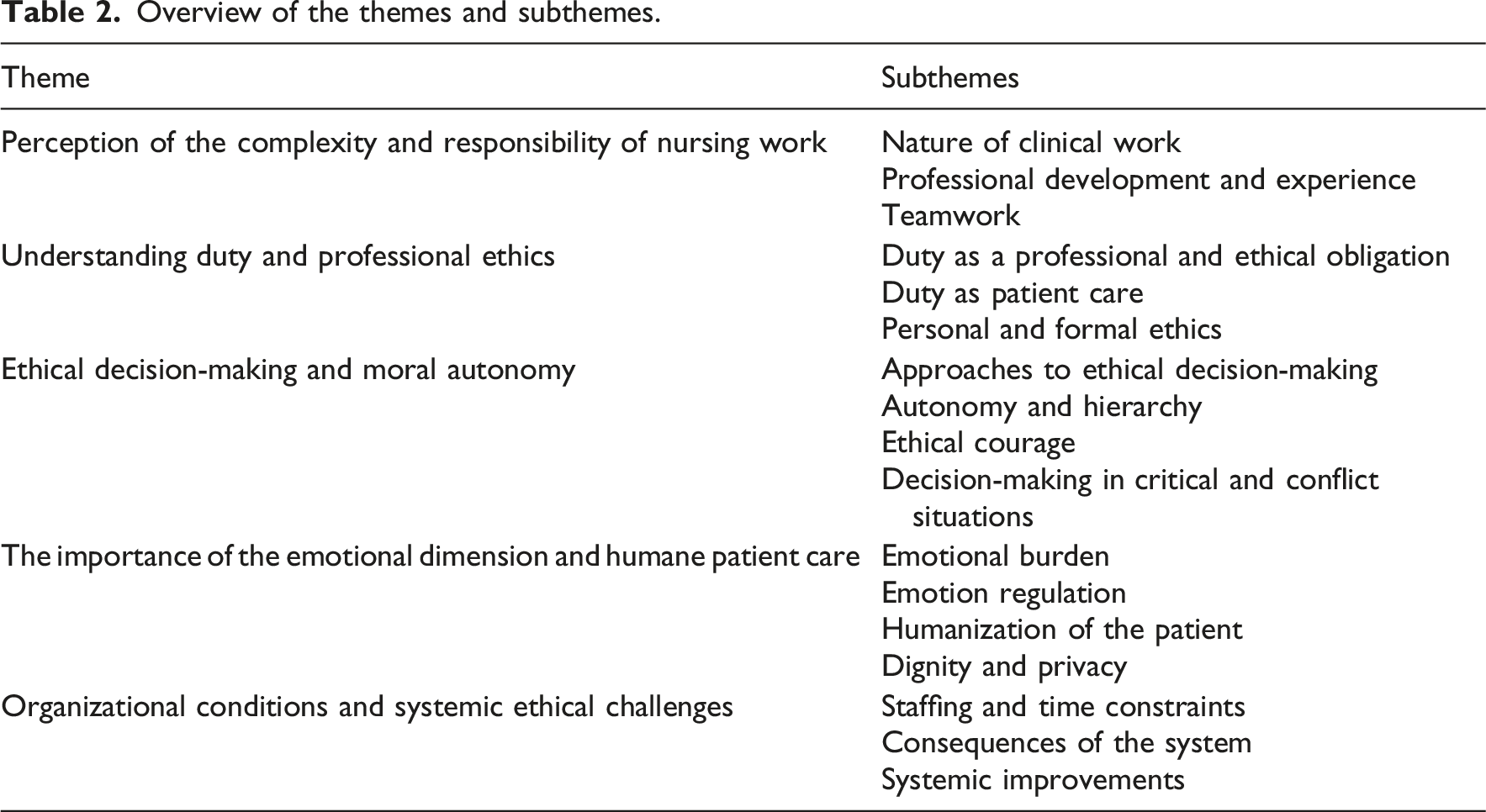
The data analysis developed five major thematic categories: perceptions of the demands and responsibilities of nursing work, understanding of duty and professional ethics, ethical decision-making and moral autonomy, the emotional dimension and humanized nurse–patient relationships, and organizational conditions and systemic ethical challenges.
Conclusions
The findings suggest that nurses largely enact Kantian ethics of duty through internalized professional values and commitment to patient dignity. However, organizational and systemic factors significantly limit their capacity for autonomous moral action. Strengthening ethical practice in nursing requires improved working conditions, enhanced professional autonomy, and structured support through ethics education, supervision, and team-based ethical reflection.
Introduction
Nurses regularly face ethical dilemmas in clinical practice, requiring them to balance professional duties, patient well-being, and personal moral judgment. While theoretical ethics provide guidance, how nurses interpret and apply duty-based principles in everyday practice remains less clear. This study aimed to explore how nurses understand and implement the principles of Kantian duty ethics in their moral decision-making and how this perspective shapes their sense of duty and professional integrity.
Background
Within clinical ethics, duty ethics occupies a distinctive position, emphasizing that the morality of an action does not derive from its consequences but from an individual’s awareness of duty. In practice, this means that nurses ground their decisions in moral principles and professional obligations rather than in personal benefit, emotions, or external pressures. Actions are considered moral when they are performed because they are right, not because of expected benefits, recognition, or reward. 1 Moral decision-making is based on ethical awareness and involves a process of observation, analysis, and weighing the possible consequences of chosen actions. In this process, nurses follow the ideal of care and the principle of “doing good,” which entails considering the patient’s well-being, the quality of care, and the patient’s dignity. 2 Moral action encompasses the ability to recognize, evaluate, and implement ethically appropriate decisions in situations where patients’ values, dignity, or rights are at risk. 3 In such situations, nurses frequently encounter internal conflicts between professional obligations, organizational expectations, and their own conscience. 4 These circumstances require a high level of ethical sensitivity, reflection, and willingness to take responsibility for one’s decisions. Ethics in nursing is therefore inseparably linked to the nurse’s personal and professional development and to their understanding of moral duty. 5
The German philosopher Immanuel Kant (1724–1804) developed one of the most influential ethical theories. His approach is grounded in the belief that human beings are primarily defined by their capacity for free and rational will, rather than by instincts, emotions, or external circumstances. Humans are moral beings because they are capable of thinking, formulating moral rules, and acting in accordance with them. 6 According to Kant, an action is moral only when it is performed out of a sense of duty, not out of self-interest, pleasure, avoidance of punishment, or the pursuit of praise. Kant therefore focuses on the question of how individuals come to know their moral duty. 7 He locates the answer in moral consciousness, or reason, which directs individuals toward what is right. This inner voice is expressed through moral commands known as imperatives. Imperatives do not originate from external authorities, institutional rules, or social pressures, but from the individual’s capacity for rational judgment. This implies that the individual is autonomous, capable of determining moral rules independently and acting in accordance with them. 8 On this basis, Kant distinguishes between autonomous and heteronomous ethics. Autonomous ethics is grounded in inner freedom, self-determination, and respect for the moral law accepted as a universal principle. Heteronomous ethics, by contrast, involves acting in response to external commands, rules, rewards, or sanctions, which limits moral freedom. 9 Kant’s doctrine is therefore referred to as duty ethics or deontology. It is based on the conviction that individuals must act out of duty, regardless of whether an action is pleasant, personally beneficial, or aligned with personal inclinations. 10
Deontological ethics, particularly Kant’s ethics of duty, plays a lasting and central role in understanding the moral responsibility of healthcare professionals. A nurse who acts in accordance with the moral law out of a sense of duty toward the patient realizes the essence of moral action in the Kantian sense, meaning that the action is performed out of duty rather than benefit. 11 Kantian duty ethics thus provides a firm and stable framework for understanding moral decision-making in clinical practice. It guides nurses toward conduct that is universally appropriate, carefully considered, and grounded in professional duty and respect for the patient as an autonomous and equal moral subject. 5
Nurses face ethical dilemmas daily, such as respecting patient autonomy when patients refuse treatment, deciding on participation in high-risk or life-sustaining procedures, maintaining the dignity of dying patients, and managing conflicts between patient wishes and institutional protocols. 2 Inadequate or inconsistent ethical decision-making in such situations may compromise patient care, violate patient autonomy and dignity, increase moral distress among nurses, and reduce trust in healthcare relationships. In such circumstances, Kant’s concept of duty offers a stable moral orientation by emphasizing that respect for the moral law is fundamental to preserving the dignity of both the patient and the healthcare professional.7,8 Nurses are therefore not merely executors of technical procedures but moral decision-makers whose actions realize core values of human dignity, truthfulness, and duty toward the patient. 9 Acting from a sense of duty represents a central element of clinical ethics, as it demonstrates how a philosophical theory such as Kant’s ethics of duty is directly enacted in practice and influences the quality of care in everyday clinical work. These considerations motivated the present study, which aimed to explore how nurses understand and implement the principles of Kantian duty ethics in everyday clinical practice and how this philosophical perspective influences their moral judgment, sense of duty, and professional integrity. By focusing on nurses’ lived ethical reasoning, this study seeks to illuminate the role of duty-based ethics in guiding moral action within complex and often ethically challenging clinical environments. Accordingly, the study was guided by the following research question: How do nurses understand and enact the principles of Kantian duty ethics in their moral decision-making in clinical practice?
Methods
Research design
A qualitative descriptive study design was employed to provide an in-depth understanding of nurses’ experiences of moral decision-making guided by the principles of Kantian duty ethics in clinical practice. We adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines to ensure consistent reporting of the qualitative research methodology. 12
Participants and settings
Purposive sampling was used to recruit nurses from various clinical settings and professional roles to capture diverse perspectives on ethical decision-making. Participants were intentionally selected to ensure variation in work environments (e.g., acute care, intensive care, and other hospital-based settings), years of professional experience, and levels of responsibility (e.g., staff nurses and those with additional responsibilities), thereby enhancing the richness and transferability of the data.
Seventeen nurses from Slovenia participated in the study. Data saturation was reached after the fourteenth interview; three additional interviews were conducted to confirm that no new themes or insights emerged, which determined the final sample size. Participants were recruited through the professional and personal networks of the research team within clinical settings. Potential participants were approached directly, informed about the purpose of the study, and invited to participate voluntarily. To protect participants’ anonymity, their characteristics are presented in aggregate form, and individual quotes are not linked to any personal identifiers. To ensure the appropriateness of the collected data, participants had to meet the following inclusion criteria: employment as a nurse in a clinical setting, age between 18 and 65 years, and willingness to be audio recorded during the interview. Exclusion criteria included having fewer than 5 years of professional experience or not currently working in a clinical setting.
Data collection
Data were collected through semi-structured individual interviews conducted between November and December 2025. An interview guide (Supplement 1) with predetermined questions was used, allowing participants flexibility to freely express their opinions and reflections. The research team developed the interview guide based on a review of relevant literature on nursing ethics and moral decision-making,7,9,13 as well as the theoretical framework of Kantian duty ethics. 14 The questions aimed to explore key concepts such as duty, moral dilemmas, and ethical reasoning in clinical practice. The development process included iterative discussions among the research team to ensure clarity, relevance, and alignment with the study aims.
The interview guide was pilot tested with two participants before formal data collection to assess clarity and relevance. No major ambiguities were identified, and the guide was considered appropriate for capturing the intended content. The first part of the interview gathered demographic information, including gender, age, years of professional experience, educational level, current position, work setting, and any additional ethics-related training. The second part consisted of open-ended questions structured around three main themes: understanding of duty, moral dilemmas in clinical practice, and duty ethics and universal principles.
Interviews were arranged individually at times convenient for each participant and conducted in a quiet and private environment. Before the interview, participants received an information sheet by email or in person, depending on the recruitment method. The information sheet described the study objectives, procedures, and participants’ rights. Participants could review the information in advance and ask questions before giving written informed consent. Written consent, demographic data, and verbal consent to audio-record the interviews were obtained if participants agreed to participate. They were informed that participation was voluntary, that they could decline to answer any question, and that they could withdraw from the interview at any time. Participants also received the interview questions in advance to ensure understanding and allow adequate preparation. No repeat interviews were conducted.
All interviews were conducted by members of the research team, both male and female, each holding a Bachelor’s degree in nursing. Before data collection, they completed structured training in qualitative research methodology, covering both theoretical and practical components (15 h), with an emphasis on conducting semi-structured interviews. Two senior researchers with extensive experience in qualitative research supervised all stages of the study, including data collection, to ensure methodological rigor and consistency. All interviews were audio-recorded. Each interview lasted an average of 30 min. Recordings were transcribed verbatim using the Transcript software and then manually checked with audio and corrected for accuracy. Transcripts were not returned to participants for comment. To ensure anonymity, participants were assigned unique codes (e.g., F.1), which included gender and the interview sequence number. This approach allowed for careful handling of sensitive data while capturing in-depth insights into nurses’ experiences and ethical reasoning.
Ethical considerations
The study adhered to the ethical guidelines outlined in the Declaration of Helsinki. 15 Ethical approval for the study was granted by the Commission of the University of Primorska for Ethics in Human Subjects Research (Approval No: 4264-16-3/2022). Participants were recruited voluntarily, explaining their rights to participate and withdraw at any time without negative consequences. Written informed consent was obtained before commencing the interview. Privacy and confidentiality were prioritized using unique codes and secure data storage methods.
Data analysis
Data were analyzed using Braun and Clarke’s six-step thematic analysis framework. 16 The analytical process was conducted inductively, without a predefined coding scheme, and included the following phases: (i) familiarization with the data—audio recordings were transcribed verbatim, and transcripts were read and reviewed multiple times to gain a thorough understanding of the content; (ii) generating initial codes—open, inductive coding was conducted, with content-relevant segments systematically identified and labeled; (iii) searching for themes—related codes were grouped into broader thematic categories; (iv) reviewing themes—categories and subcategories were compared with the codes and evaluated for coherence and consistency; (v) defining and naming themes—further analysis was conducted to refine each theme, ensuring clear boundaries and precise definitions; (vi) producing the report—data-rich examples were selected to illustrate and support interpretation of the findings.
ATLAS.ti software (Scientific Software Development GmbH, Germany) was used to analyze the data. To ensure reliability, triangulation was employed: three researchers independently coded the data and then compared their coding schemes, discussing discrepancies and reaching consensus on the final application of codes, subcategories, and categories. Unique codes were consistently used throughout the analysis to maintain participants’ anonymity. The iterative process of coding, theme identification, and refinement was conducted collaboratively by all authors to ensure an accurate representation of nurses’ experiences and ethical reasoning.
To enhance rigor, several strategies were used, including investigator triangulation, iterative data analysis, and regular discussions among the research team to ensure consistency and credibility of the findings. Field notes were taken during and immediately after interviews to capture contextual information and initial reflections, and these were shared and discussed within the team. Any discrepancies in coding or interpretation were resolved through discussion until consensus was reached.
Reflexivity was considered throughout the research process. All members of the research team had a background in nursing, which provided valuable contextual understanding but also required ongoing reflection on potential assumptions and biases. Regular team discussions were held to critically reflect on interpretations and to ensure that findings remained grounded in participants’ accounts rather than researchers’ preconceptions.
Findings
Participants’ demographics.
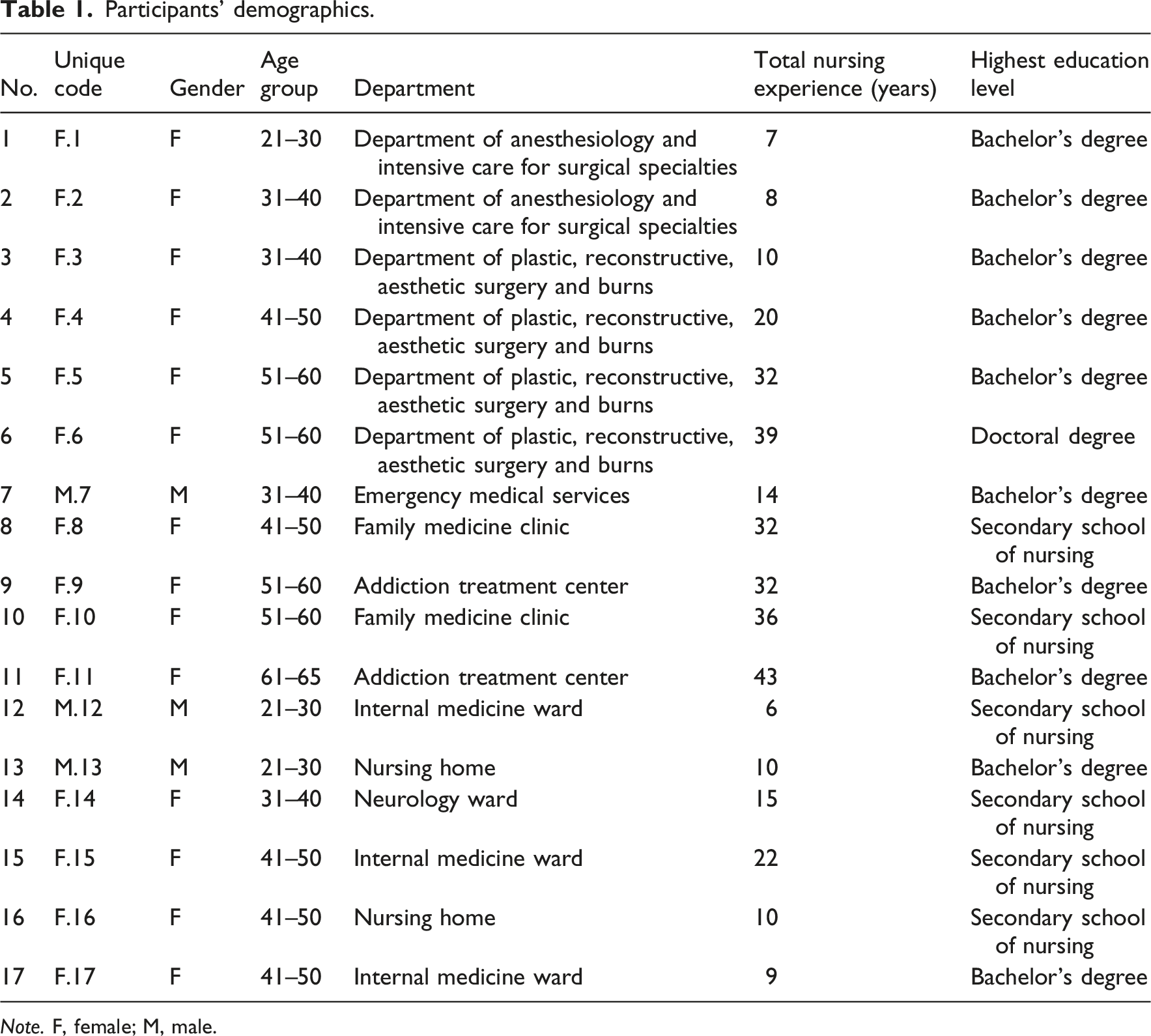
Note. F, female; M, male.
Overview of the themes and subthemes.
Theme 1. Perception of the complexity and responsibility of nursing work
Participants described clinical work as highly demanding and responsible, emphasizing its complexity, the high level of professional knowledge required, and the ability to make rapid decisions. Particular attention was given to work in intensive care units, where patients are often critically ill and fully dependent on healthcare staff. This further increases their sense of professional and ethical responsibility. Participants also highlighted the vulnerability of certain patient groups and nurses’ commitment to acting in the patients’ best interests and ensuring high-quality nursing care. “The experience I gained is primarily related to working with critically ill patients, which includes patient observation, monitoring vital signs, and working with various tools and devices such as pumps, ventilators, and hemodynamic and other monitors” (F.6). “Always acting in the patient’s best interest, making every effort to provide quality nursing care” (F.2).
Professional development was described as a continuous process that involves gaining experience in different clinical settings, developing organizational competencies, and the ability to handle demanding work situations. In addition to professional knowledge, participants emphasized the importance of learning to balance professional and personal life, linking this balance to greater personal stability. A key factor in establishing this balance was working according to protocols, which allows nurses to face ethical challenges in clinical practice more confidently and with less emotional burden. “I have especially improved in separating work and personal life” (F.5). “If I follow protocols, emotions or compassion do not present a particular obstacle, as I believe I am doing the best I can” (F.1).
Teamwork was recognized as an essential factor for quality and effective clinical practice. Participants emphasized constant collaboration, adaptation, and coordination with different members of the healthcare team. Special importance was attributed to team discussions and joint ethical decision-making, which enable participants to resolve ethical dilemmas and find professionally justified solutions. However, challenges of teamwork were also noted, particularly during time pressure, which can hinder timely decision-making and action in clinical practice. “I usually discuss this with colleagues, those who are working with me at the time, and I also consult a superior; together we usually find a solution” (F.2). “Sometimes a patient’s condition deteriorates rapidly, and you need a physician’s opinion and assistance, but they are occupied with other work” (F.1).
Theme 2: Understanding duty and professional ethics
Participants understood duty as a commitment to professional standards, guidelines, and protocols. This forms the foundation of safe, high-quality, and ethically grounded nursing care. Orientation toward the patient’s well-being was highlighted as a central element and a guiding principle in all professional and ethical decisions in clinical practice. “I understand duty as ethical conduct aimed at the patient’s well-being, ensuring safe and professional care through strict adherence to protocols and guidelines” (F.1). “I always first adhere to the professional and ethical principles of nursing” (F.10).
The patient was regarded as the primary value, taking precedence over all other work obligations or organizational constraints. Some participants perceived ethical conduct not only as a professional duty but also as a personal value, reflecting a high level of internalization of ethical principles. “It all depends on the situation; you must always keep in mind that everything you do is for the patient’s benefit” (F.1). “I do not feel this as a duty but as a mindset or part of who I am” (F.15).
A clear distinction was expressed between personal ethics, arising from internal values and personal beliefs, and formal ethical duty, dictated by institutional rules. Formal obligations were described as work with low emotional involvement, detached from direct patient care. “Out of duty, I perform mandatory delegated tasks from management, handle statistics, use the required programs—there are no emotions; this work must be done even if I do not see its real value, nor do I receive feedback” (F.5).
Theme 3: Ethical decision-making and moral autonomy
Despite diverse approaches to ethical decision-making, empathy was often recognized as a fundamental basis. Ethical decision-making was understood as a thoughtful process requiring time and consideration of different perspectives. Decisions were often context-dependent. Independent ethical decision-making was highlighted as an important expression of professional autonomy and responsibility. “I try to put myself in their shoes, make an effort to remember their names, not just diagnoses” (F.2). “I believe that one must always make decisions based on the situation at hand” (F.14). “I make ethical and professional decisions independently, for which I am also accountable” (F.3).
Professional autonomy was described as partially limited due to organizational and hierarchical structures within the healthcare system. Autonomy was understood as independence within clearly defined rules, guidelines, and institutional frameworks. Despite hierarchical subordination, participants emphasized personal moral boundaries, which they were unwilling to cross when they judged it to be in the patient’s best interest. Ethical dilemmas often arose in situations where the appropriateness or adequacy of planned patient care was questioned. “Sometimes a consulting physician requests a procedure, but I do not agree as a nurse; in such cases, I express and justify my decision, still in accordance with guidelines and for the patient’s benefit” (F.4). “I asked the physician to provide the patient with additional explanations and instructions” (F.8).
Ethical courage was highlighted as a professional competence of nurses in facing ethical dilemmas, particularly in disagreements with other professionals. Hierarchical structures were sometimes noted as inhibiting ethical action. Ethical courage was also demonstrated in rapid and decisive ethical judgments in urgent situations requiring immediate action for the patient’s benefit. An important aspect of ethical courage involves communication with family members, especially when managing sensitive information. “A patient with extensive burns on both arms and legs was scheduled for discharge as decided by the attending surgeon. Since I had cared for the patient for several days, I noticed she needed significant assistance with basic daily activities” (F.8). “I recognize situations where immediate action is needed for the patient’s benefit” (F.8). “Knowing what information to provide in such cases; luckily, I have a few phrases ready to avoid excessive interrogation” (F.8).
These accounts illustrate how nurses actively negotiate tensions between professional autonomy, hierarchical constraints, and patient advocacy, often requiring rapid judgement and a willingness to take personal responsibility. However, in certain situations, nurses choose to deviate from standard rules when they judged it to be in the patient’s best interest. These decisions were associated with individualized and humane patient care. Prioritization in ethical conflicts was emphasized, particularly during time and organizational pressures. “The patient wanted to smoke one last cigarette; after consulting my colleague, I took her outside where she smoked half a cigarette and was immensely grateful. The patient died next day” (F.4). “I prioritize work processes based on the urgency and necessity of procedures and interventions” (F.9).
Theme 4: The importance of the emotional dimension and humane patient care
Nurses described emotional burden as an inseparable part of clinical work, significantly affecting their well-being and long-term sustainability in the profession. The need for self-protection and setting emotional boundaries was emphasized as crucial for maintaining psychological balance and professional effectiveness. Nonetheless, they acknowledged that completely excluding emotions is impossible. Emotional burdens often arose in the context of moral dilemmas involving patients and family members. Regardless of emotions, patient well-being was always prioritized. “I believe it is important to establish boundaries at work, as responding purely based on emotions or compassion could have a negative long-term impact on my psychological well-being” (F.2). “Of course, certain cases evoke emotions and compassion, but I believe it is beneficial” (F.14). “Patients often refuse medications, or family members may want us not to disclose the severity of their condition” (F.4).
Conscious emotion regulation was identified as an important professional competence, enabling the maintenance of professional judgment and ethically grounded decision-making. Protocols and professional guidelines acted as protective mechanisms, helping nurses maintain professional distance and confidence in their decisions. Nevertheless, participants stressed the importance of a humane approach that recognizes the patient as a whole person. “When I have time, I talk with patients, listen to them, and try to fulfill small wishes” (M.12). “I frequently take the time to engage with them in conversations about everyday life” (F.2).
As an element of holistic and ethically grounded care, participants emphasized patient humanization and the importance of interaction with family members. Contact with family allowed a comprehensive view of the patient, contributing to a more empathetic and responsible approach. Safeguarding patient dignity and privacy was highlighted as a fundamental ethical duty, despite systemic limitations. “Interaction with family, who are often in distress, helps me remember that the patient is a person—a father, brother, partner to someone” (F.1). “Allowing family presence during nursing care” (F.14). “On our ward, we still have a six-bed room without privacy during rounds, where patients cannot freely ask what they wish” (F.2).
Theme 5: Organizational conditions and systemic ethical challenges
Staffing and time constraints were identified as the most significant systemic factors affecting ethical practice. Staff shortages were linked to patient safety concerns, increased workload, and constant pressure on ethical decision-making. In response, participants reported personal sacrifices. Ethical consequences of these constraints manifested in reduced quality of care and diminished human aspects of nursing. “Due to staff shortage, I have come to work while ill, so as not to burden the head nurse or colleagues” (F.9)
Despite systemic limitations, participants emphasized personal and professional commitment to prioritizing patient needs over efficiency. They also highlighted the connection between staffing stability and quality of care. Outdated equipment and extensive administrative requirements were cited as ethical challenges. Needs for clearer competencies, better material conditions, and adequate remuneration were stressed. Organized reflection on ethical dilemmas was identified as an important supportive mechanism. “If a patient has difficulty walking, I make the effort to accompany them to the bathroom instead of bringing a bedpan, which would be faster” (F.2). “If the unit is not understaffed, time and other pressures decrease as team dynamics improve, work flows smoothly with less mental and physical strain” (F.1). “We highlight major problems in daily morning meetings so that dilemmas can be discussed among all team members” (F.17).
Discussion
This study explored how nurses experience and enact ethical principles in their everyday clinical practice, particularly when faced with complex, emotionally challenging, and morally demanding situations. The findings indicate that participants perceive their role as highly responsible and ethically grounded, requiring a combination of professional knowledge, rapid decision-making, and constant attention to patient care. The analysis identified five major themes that illuminate nurses’ understanding of their duties, their approaches to ethical decision-making, and the influence of emotional and organizational factors on their practice. These findings are interpreted using a Kantian ethical framework, with particular focus on the concepts of duty, autonomy, and the role of rational moral principles in clinical decision-making.
The findings of this study indicate that nurses perceive their role as highly demanding, ethically responsible, and emotionally challenging, particularly in clinical settings where patients are critically ill and entirely dependent on healthcare staff. Participants highlighted the need for rapid and precise clinical decision-making, a high level of professional knowledge, and constant vigilance in monitoring vital signs and using complex medical equipment, reflecting a strong sense of professional and moral responsibility. This understanding of the nursing role is supported by the findings of Maluwa et al., 17 who define ethical competence as a cornerstone of safe and high-quality nursing care and a key skill for navigating complex clinical and ethical situations.
A significant aspect of nurses’ professional identity in this study was the internalized ethical commitment to act in the patient’s best interest, which goes beyond the formal fulfillment of institutional requirements. Participants described duty as part of their own value system and as a way of “being a nurse,” indicating a deeply internalized moral orientation, which can be understood in Kantian terms 14 as an expression of commitment to duty grounded in rational moral law rather than subjective inclination. These findings are directly supported by Walden et al., 18 who observed that nurses experience their professional duty as an internal moral obligation integral to their moral identity, rather than merely an externally imposed task. The authors Walden et al. 18 emphasize that nurses often act in the patient’s best interest, even when this involves personal burden or risk. This can be understood in the context of Kantian ethics, where the moral worth of an action lies in acting from duty rather than inclination, grounded in the concept of a good will. 14 Professional values such as integrity, altruism, and responsibility play a significant role in ensuring the quality of nursing care and in strengthening professional identity and ethical clinical practice.5,19,20
Furthermore, the findings indicate that nurses understand ethical decision-making as a deliberate and context-dependent process, in which empathy plays a central role. While empathy and compassion are considered important in practice, from a Kantian perspective, moral action must be grounded in rational duty rather than empirical inclinations.13,14 In this sense, empathy may support moral awareness but does not form the basis of moral action. This distinction highlights a potential tension between experiential aspects of nursing practice and the Kantian emphasis on rational moral justification. This is further corroborated by Fidan et al., 21 who found that higher levels of compassion and empathy are associated with greater moral courage among nurses and a willingness to advocate for patients even in ethically challenging situations. The findings also highlight the tension between professional autonomy and hierarchical constraints. Nurses emphasized personal moral boundaries and their readiness to advocate for patients, even when this entails the risk of conflict with superiors. Our findings align closely with Pajakoski et al., 22 who define moral courage as a key expression of professional autonomy and a central mechanism through which nurses fulfill their moral responsibility under institutional pressure. In Kantian terms, this reflects the distinction between autonomy, in which moral agents legislate moral law through reason, and heteronomy, in which action is shaped by external influences or constraints.13,14
The emotional dimension represents a significant component of nurses’ clinical work and strongly affects their well-being and professional effectiveness. Participants emphasized the need for conscious emotion regulation and setting emotional boundaries as protective strategies to maintain psychological balance. Wang et al. 23 describe empathetic work as an intensive form of emotional labor that requires constant regulation of emotional responses for the benefit of the patient. Prolonged exposure to emotionally demanding situations increases the risk of fatigue and burnout among nurses. 24 Importantly, participants do not seek to deny their emotions but aim to recognize and regulate them so they do not override professional and moral judgment. This aligns with emotion regulation strategies, including the use of clinical protocols, which help maintain professional distance and stable clinical judgment in challenging situations.25,26 From the perspective of Kantian duty ethics, this can be understood as striving for decision-making grounded in duty and professional principles while acknowledging emotions as an integral part of the human experience. Nonetheless, research indicates that providing humanized care represents an additional source of emotional burden.25,26 This is confirmed by Munkeby et al., 27 who describe the phenomenon of “moral distress” in nurses when organizational constraints prevent them from acting in accordance with their moral and professional values.
The findings clearly point out that organizational conditions significantly shape nurses’ ability to act ethically. Staff shortages, time constraints, and high workloads are associated with reduced quality of care, more frequent ethical dilemmas, and feelings of moral distress.25,28 Within a Kantian framework, this suggests that the space for autonomous duty-based action can be narrowed by heteronomous systemic pressures, increasing moral tension and the risk of distress. Therefore, organizational support (such as team support, reflection on ethical dilemmas, and systematic supervision) is particularly important for maintaining professional autonomy, well-being, and ethically grounded clinical judgment.29–31 At the same time, the findings suggest that real-world clinical practice may diverge from strict Kantian requirements for autonomous, duty-based action, especially in situations influenced by emotional demands and systemic constraints.
Study strengths and limitations
A key strength of this study is its inclusion of nurses from diverse clinical settings, which allowed for the exploration of a wide range of experiences and perspectives regarding ethical decision-making in nursing practice. This diversity enhances the depth and richness of the findings, providing a comprehensive understanding of how nurses perceive and enact ethical principles in real-world clinical contexts. Additionally, the use of in-depth qualitative interviews enabled participants to express their personal insights and experiences, capturing the emotional, moral, and organizational dimensions of ethical practice that may not be easily quantified in survey-based studies. The study also emphasizes the integration of theoretical perspectives, particularly Kantian duty ethics, with practical nursing experiences, offering valuable insights for both clinical practice and nursing education.
Several limitations should be acknowledged. The first limitation relates to the sample composition (14 women and 3 men). This is important due to the fact that the experience of ethical challenges may differ by gender. Next, seventeen nursing practitioners from various clinical environments were included, where ethical dilemmas, the level of autonomy, and organizational pressures may vary. This allows insights into diverse experiences but limits the generalizability of the findings to the wider population of nurses. Next limitation concerns the recruitment method as participants were selected based on the personal contacts of the research team. While purposive sampling is appropriate for qualitative inquiry, this approach may have introduced selection bias and influenced the perspectives represented in the study. Finally, the findings should be interpreted within the specific cultural context and healthcare system in which the study was conducted. Ethical decision-making in nursing is shaped by societal values, the level of healthcare system development, and the organizational structure of health services. Differences in cultural norms, healthcare policies, and institutional frameworks may therefore limit the transferability of the results to other countries or healthcare settings.
Implications
The findings highlight nurses’ awareness of ethical dilemmas in daily clinical practice and their ability to navigate complex moral situations in accordance with duty-based ethical principles. However, participants stressed that ethical action is not solely an individual responsibility but is strongly shaped by organizational and systemic conditions. Strengthening professional autonomy was identified as essential for enabling greater independence and accountability in clinical decision-making, particularly in hierarchical healthcare environments where organizational pressures may conflict with duty-based ethical principles.
The results indicate the need for concrete systemic measures, including improved staffing levels, adequate material resources, and organizational support that provides nurses with sufficient time and space for ethical deliberation. Participants also emphasized the importance of implementing regular, structured forms of ethical reflection, supervision, and ethics consultation within clinical settings to support moral reasoning and reduce emotional burden.
Importantly, the findings extend beyond a purely ethical perspective and highlight the practical relevance of ethical decision-making for daily clinical practice. Ethical reasoning emerges as an integral component of clinical judgement, particularly in acute care settings where nurses must respond rapidly to complex and uncertain situations. This suggests that ethical competence should be understood not only as a moral obligation but also as a core clinical skill directly linked to patient safety, quality of care, and professional accountability.
For clinical practice, the findings suggest that nurses should be supported in actively integrating ethical reflection into routine decision-making. This includes brief team-based discussions, reflective practice, and assertive communication when advocating for patients, especially in situations involving conflicting priorities or hierarchical constraints. Such approaches may strengthen both individual decision-making and team-based ethical coherence.
In addition, the findings suggest important implications for nursing education. Integrating applied clinical ethics, moral courage, communication skills, and emotion regulation into nursing curricula can strengthen nurses’ capacity to justify, reflect on, and act upon ethical decisions in complex clinical contexts. These competencies are particularly relevant for managing ethical dilemmas under time pressure and within organizational constraints.
Conclusion
This study contributes to understanding ethical decision-making in nursing by offering insights into how nurses interpret and apply Kantian duty ethics in everyday clinical practice. A key strength of the study is its grounding of ethical action in nurses’ lived experiences, including emotional demands and organizational constraints, rather than treating ethics solely as a theoretical construct.
The findings reveal limitations of normative approaches to clinical ethics by demonstrating that nurses’ moral autonomy is strongly shaped by systemic and organizational conditions. Strengthening professional autonomy, improving working conditions, and providing regular ethical reflection and supervision are therefore essential to support duty-based ethical practice. The results also underscore the importance of ethics education that integrates clinical ethics, moral courage, and emotion regulation, enabling nurses to reflect on ethical decisions, maintain psychological well-being, and uphold professional values in complex clinical settings.
Supplemental material
Supplemental material - Nurses’ moral decision-making in practice through Kantian duty ethics
Supplemental material for Nurses’ moral decision-making in practice through Kantian duty ethics by Mirko Prosen, Nađa Antonić, Ema Sovinec, Mitja Zdovc, and Sabina Ličen in Nursing Ethics
Footnotes
Acknowledgments
We extend our gratitude to all the participating nurses for their invaluable contributions to this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.