
Abstract
Using Scandinavian literature reporting patient experiences of intensive care as a case, the aim of this qualitative systematic review was to explore if humanising was addressed in the descriptions of patient experiences and, if so, what words and theoretical perspectives were used to underpin the results. A comprehensive search of qualitative studies published between 1 January 2016 and 12 December 2024 was conducted in Embase, CINAHL, MEDLINE, Scopus, and Web of Science. Twenty-nine studies reporting patient ICU experiences were included and analysed using thematic synthesis following Thomas and Harden. The review adhered to the Enhancing Transparency in Reporting the Synthesis of Qualitative Research checklist. The terms humanisation and de-humanisation were not explicitly used, but the studies engaged with these concepts by corroborating the three themes that defined humanising ICU in this study: (1) feeling recognised as a human being when experiencing connectedness with healthcare professionals, (2) feeling connected with themselves and the situation when experiencing safety and well-being, and (3) feeling connected with significant persons and life outside the ICU. In addition, our analysis identified a further theme: (4) experiencing capacity to influence the situation when able to express themselves. Humanising intensive care involves ethical and caring engagement with the patient, helping them feel connected, experience well-being, and influence their situation. Although Scandinavian literature has not directly studied humanisation, it has focused on understanding patients’ experiences and addressing the ontology of critical illness. As such, humanising ICU aligns well with Scandinavian nursing traditions.
Implications for clinical practice
ICU staff should actively listen to patients and encourage them to express needs and preferences, create a safe and calm environment that supports well-being, and maintain communication with patients and families to promote a humanising approach to intensive care.
Introduction
Advances in lifesaving technology and medical treatment have improved survival rates for critically ill patients admitted to intensive care units (ICUs) over the past decades.1,2 However, the human dimensions of care can be obscured by lifesaving technological and medical advances. 3 A significant number of former ICU patients struggle to recover physically and psychologically and experience posttraumatic stress disorder, anxiety, and depression after hospital discharge.4–6 In response to patients’ suffering, there is an increasing interest in promoting a more humanised approach to intensive care,7,8 including a shift towards patient- and family-centred care that meets the individual beliefs and needs. 9 Since 2014, the Spanish Proyecto HUCI (https://proyectohuci.com) has promoted a humanised approach to intensive care, focussing on areas such as open-door policies, communication, patient well-being, family involvement, end-of-life care, and humanised infrastructure. 8 A scoping review 10 revealed that humanising care was described as holistic care of the patient, the attitude of healthcare professionals toward patients, and humanisation as an organisational approach encompassing all subjects within the healthcare system. A systematic review by Nielsen, Kvande, and Angel 11 synthesising findings from qualitative studies of patients’ ICU experiences found that intensive care was humanised when patients felt connected with healthcare professionals, with themselves and the situation when experiencing safety and well-being, and with significant persons and life outside the ICU.
In Scandinavia, healthcare is publicly funded, and ICUs are generally well staffed with nurse-patient ratios of 1:1 or 1:2, with no use of restraints. In this setting, the non-sedation paradigm that originated in early 200012,13 has spurred an interest in patients’ experiences of intensive care. 14 However, despite a long tradition for research in patients’ ICU experiences, 14 the review by Nielsen et al. 11 found only one Scandinavian study exploring patients’ experiences of humanising intensive care. This finding piqued our interest in whether the phenomenon of humanised ICUs might have been described using other terms in Scandinavian literature. If uncovered, such perspectives could provide valuable insights into how intensive care can be humanised to the benefit of ICU patients.
Therefore, using Scandinavian literature reporting patient experiences of intensive care as a case, the aim of this qualitative systematic review was to explore if humanising was addressed in the descriptions of patient experiences and, if so, what words and theoretical perspectives were used to underpin the results.
Methods
Design
This study employed a qualitative systematic review and thematic synthesis of qualitative studies following the method outlined by Thomas and Harden. 15
Inclusion criteria
Inclusion criteria include qualitative Scandinavian research papers exploring adult ICU patients’ experiences of intensive care. A previous scoping review 10 mapped literature on humanising intensive care and identified the year 2016 as the inception point. We therefore limited our search from 1 January 2016 to 12 December 2024.
Exclusion criteria
Exclusion criteria include the following: non-ICU setting, patients under 18 years, and end-of-life care; settings outside Denmark, Norway, and Sweden; reviews, conference abstracts, comments, editorials, and letters or not available in English, Danish, Swedish, or Norwegian.
Selection of studies for review
In April 2023, we searched Embase, CINAHL, MEDLINE, Scopus, and Web of Science for qualitative research papers reporting patients’ experiences of intensive care. In collaboration with the authors, a librarian experienced in research built a comprehensive and systematic search strategy in MEDLINE using medical subject headings and text words. The final search strategy in MEDLINE, shown in Appendix 1, was adapted for the other databases. The search was updated on 12 December 2024. The PRISMA flowchart (Figure 1) shows that a total of 1779 potentially relevant papers were identified. All identified studies were transferred to the reference management software Covidence, where 553 duplicates were removed. Two and two authors (MEK, SA, AHN) screened 1,226 papers based on title and abstract. In case of disagreement, the third author made the decision. Screening was done using the Covidence application, an internet-based application for handling, screening, and including papers in systematic reviews. A total of 29 papers were independently assessed for quality (Appendix 2) using the Critical Appraisal Skills Programme Qualitative Checklist (CASP-QC)
16
by two authors and discussed until consensus was reached. 29 papers were included in the study. PRISMA diagram.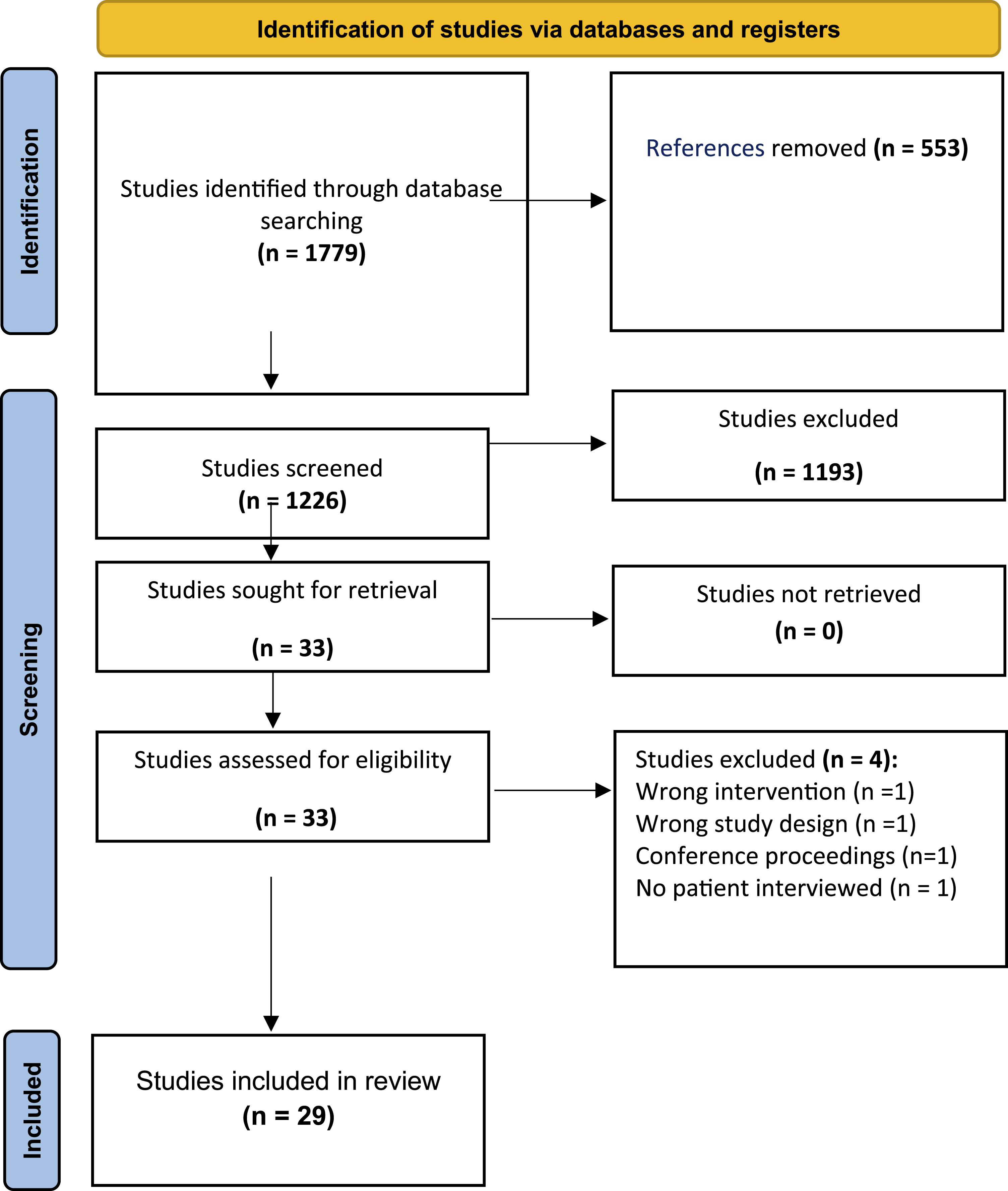
Data extraction
As we were exploring if humanising were addressed in descriptions of patients’ experiences of intensive care in a sample of Scandinavian literature that did not explicitly use the terms humanising or de-humanising, we organised the extraction and synthesis of data around two analytic questions: (1) How did patients’ experiences of intensive care reflect intensive care as humanising or de-humanising? and (2) What theoretical perspectives underpinned the results? The three themes from our previous study 11 were used to guide our understanding of when intensive care could be experienced as humanising or de-humanising: (1) Patients felt recognised as human beings when they experienced connectedness with healthcare professionals; (2) experiencing safety and well-being helps patients feel connected with themselves and the situation; (3) feeling connected with significant persons and life outside the ICU.
The following data were extracted from the included papers: authors, publication year, journal, title, country of origin, objective, and research design/methodology. We extracted themes, quotes, and results pertaining to patients’ experiences of intensive care as humanising or de-humanising. Finally, the theoretical frameworks or studies used to discuss or underpin results pertaining to patient experiences of intensive care as humanising or dehumanising were extracted. Data extraction was handled in Microsoft Excel. All authors read all included papers, and extractions were discussed until agreement was reached.
Synthesis of findings
Extracted excerpts from the included papers were read line by line and coded deductively using the three themes from our previous study as template 11 and inductively, using open descriptive codes. The descriptive codes were subsequently used for organising the data into related areas and developing more comprehensive descriptions of each area into themes.
This was an iterative process of hermeneutic reading and writing, going back and forth between excerpts and the generated descriptive themes and a movement towards more interpretive themes that reached beyond the original papers 15 and beyond the themes from our previous study. 11 Interpretations were continually discussed by all authors until agreement was reached.
Descriptions of theoretical frameworks or studies were categorised and summarised, but no further interpretation was attempted. The study was reported using the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) 17 (Appendix 3).
Findings
Descriptive characteristics of the articles (n = 29).

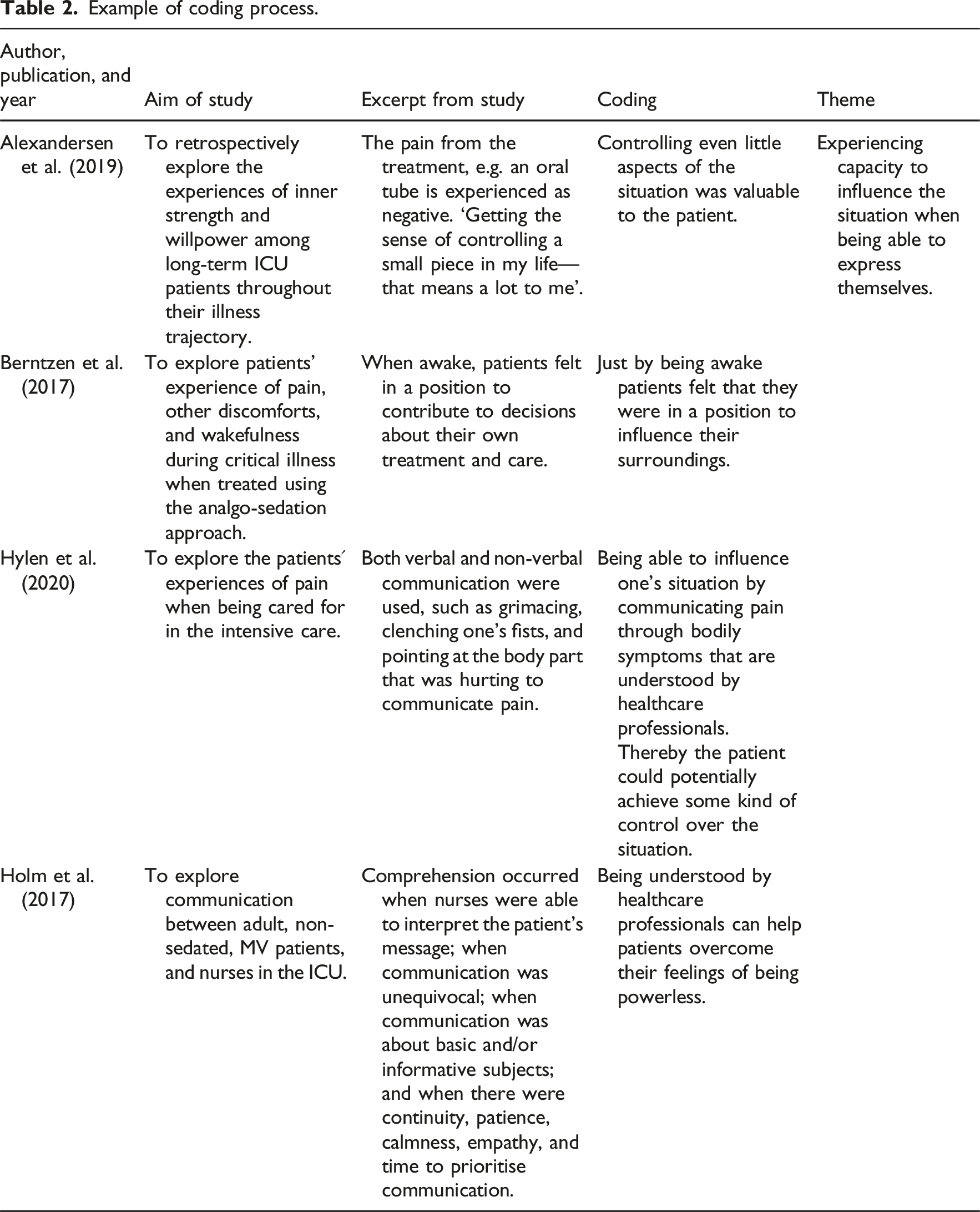
Example of coding process.
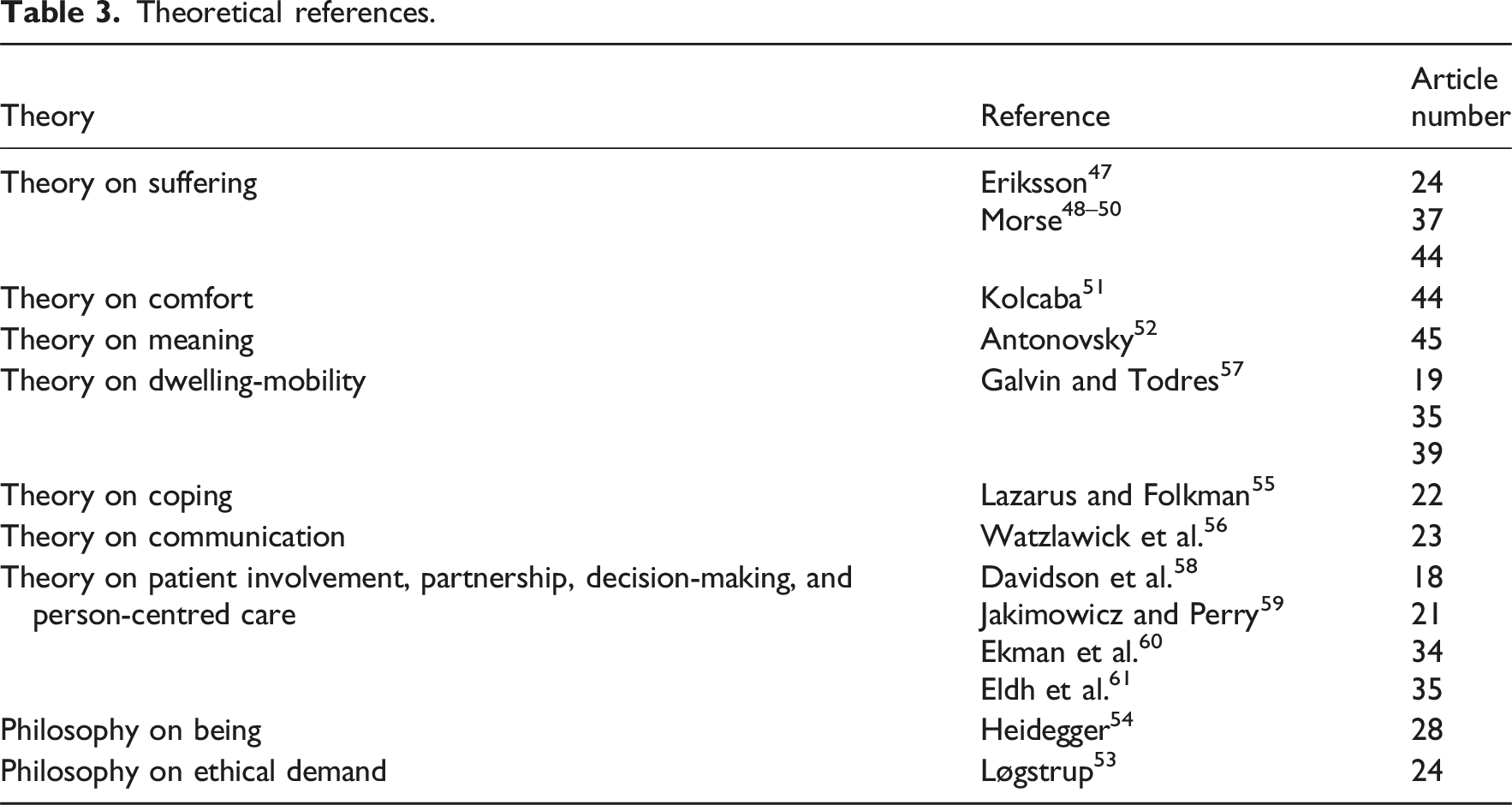
Theoretical references.
All papers discussed their findings in the light of other studies or reviews. Four of twenty-nine papers discussed their reported aspects of humanising or dehumanising with reference to the literature on patient involvement, partnership, decision-making, and person-centred care. Seven papers referenced a metasynthesis by Egerod et al. 14 about patient experiences of critical illness, thirteen papers referenced nursing theory and other philosophy, and only two referenced papers about humanising to discuss their findings.
Feeling recognised as a human being when experiencing connectedness with healthcare professionals
Patients in the ICU expressed how important it was for healthcare professionals to respect them and treat them as valued human beings rather than seeing them as a critical illness or just a diagnosis.18–22 Healthcare professionals who showed interest in patients as individuals with unique personalities and everyday lives were important to patients’ experience of humanisation of care.18–21,23,24
Several studies described being looked in the eyes, smiled at, and touched with kindness as creating a connection between healthcare professionals and patients that humanised intensive care.22,25–27 ‘The one most important thing was to have eye contact with the nurse’.
25
Nurses who were attentive and patient during fearful moments of deterioration in the ICU managed to help patients feel more secure in their presence and provide human intensive care despite an uncontrollable medical state and environment.19,21,24,28–32 Diverting the patient’s thoughts from the difficult situation with laughter and jokes helped patients endure, 33 which shows that establishing contact with patients is key to humanising care.
Patients’ interactions with nurses were not remembered as exclusively reassuring; some patients had memories of nurses being careful and cautious, and constantly focused on them during different caring actions, while other nurses acted more like machines,22,25,29,30 which again underscores the importance of the attitude and preparedness of healthcare professionals for connecting with patients.
Feelings of loneliness, alienation, isolation, and the loss of a sense of self could be countered by healthcare personnel when they established a relationship with the patient, thereby promoting humanised care.20,30 However, Køster et al.
20
described the detrimental effects of not recognising patients as valued individuals. ‘Not only did patients experience being addressed as a “spreadsheet of numbers” and an “object of manipulation,” but this attitude towards the body was also internalized by the patients themselves’.
20
This shows that objectification of patients influenced their sense of self negatively, whereas healthcare personnel’s efforts to acknowledge patients as valued persons may contribute to humanising intensive care.
Experiencing capacity to influence the situation when being able to express themselves
Patients emphasised that it was essential to be understood and were thankful when healthcare professionals managed to interpret their messages.25,28,34–37 However, patients expressed difficulties understanding the nurses and frustration being unable to express their basic human needs, such as thirst and the need for water.25,38 Being voiceless meant that patients could feel undignified or even humiliated when communication failed.21,35,36,38 Therefore, healthcare professionals’ willingness to communicate affected the degree to which patients felt in control,28,29,33–36,39–41 but involving patients in their care helped them to maintain self-esteem, made it possible to endure discomfort, and was perceived as a relief. ‘I was told not to touch, but they [nurses] discovered that I wouldn’t pull it [the endotracheal tube] out. Then they let me hold it and turn it a bit so that it didn’t irritate me in the throat’.
33
Being allowed to be part of a decision regarding whether to start mobilisation or to wait and just do simple things like wiping their mouth or changing their body position was essential21,35,39 and a sign of being able to manage themselves. 33 This shows that being conscious is key for patients to maintain a sense of influence, even if their participation is minimal.
Experiencing safety and well-being helps patients feel connected with themselves and the situation
Patients remembered both fantastic nurses and inexperienced, insecure nurses and emphasised that continuous care from experienced nurses was perceived as essential for feeling safe and secure in an unknown world.25,27,35 Feeling nurses’ presence and experiencing positive contact promoted a sense of safety and well-being.19,32,42 ‘It was nice of them to try to make it a little humane; someone held my hand when they washed me’.
22
Being cared for in a safe and calm environment also promoted well-being, 20 whereas disturbing elements such as light or noise made rest impossible and promoted discomfort. 25 Patients experienced feeling disconnected from their own body, changes in body functions, and feeling as though they were in a dream, floating between reality and delusions.20,21,25,26,38 Losing control over their body, feeling helpless, and becoming totally dependent on others affected the patients’ integrity and connection with themselves.26,34,38 Healthcare professionals’ initiatives to promote aesthetically founded well-being or the use of familiar aspects such as personal items in care contributed to the patients’ experience of feeling safe and secure in an unfamiliar world.35,43 This illustrates that healthcare professionals’ efforts to mitigate the strange and technological aspects of the ICU environment may help patients experience a sense of well-being and safety.
Feeling connected with significant persons and life outside the ICU
Patients remembered feeling safe and calm when family members were present. Even unconscious patients registered family members’ presence,18,21,25,44 which made them feel loved and cared for.
19
Family members gave patients strength to carry on24,45 and motivated them to struggle.
21
In addition, family members were experienced as a lifeline of hope for the patient and focused on the patient as a person and the patient’s familiar life, individual preferences, and situation.19,21,23 ‘The adjacency of their close ones connected them to their familiar life, thereby creating a safe space in an unsafe existence’.
19
Family members were described as the sole representatives of normality in the otherwise unfamiliar world of the ICU,18,19 which underscores the importance of supporting the bond with significant persons and life out of the hospital. 46
Theoretical perspectives underpinning the results
In our search for the theoretical underpinnings of the articles’ findings on humanising aspects of intensive care, we looked at the discussion sections of the included studies. Mostly, the studies referred to other studies or reviews to support or refute their findings. Most prominent was a Nordic meta-synthesis of patients’ ICU experiences by Egerod et al., 14 in which being an ICU patient was aligned with a liminal state, where patients faced a choice between life and death before transitioning back to life.20,21,28,35,41,44,45
However, 13 studies also referred to theories or philosophy. Granberg-Axèll and Bergbom 37 discussed their findings in the light of the Nordic nursing philosopher Professor Katie Eriksson’s work. 47 In addition, we found discussions using Morse’s48–50 theory on suffering24,44 and Kolcaba’s 51 theory on comfort. 44
Some studies discussed their findings using philosophy or other theory. Alexanderson et al. 45 referred to Antonovsky’s 52 discussion of how patients make meaning in relation to inner strength and will to live, and Vester et al. 24 used Løgstrup 53 to support the importance of belonging to a couple and having mutual trust and obligation to care for one another with reference to ethical demand. Wallander Karlsen 28 referred to Heidegger’s 54 philosophy of being. The theory of coping 55 was a reference in Vogel’s 22 discussion, whereas Nyhagen 23 referred to Watzlawick et al.’s 56 theory on communication. The dwelling-mobility framework by Galvin and Todres 57 was used to explore the tension between patients’ inability to act in their current situation and an orientation toward future possibilities.19,35,39
Finally, four studies18,21,34,35 discussed their findings in the light of patient involvement, partnership, decision-making, and person-centred care58–61 and only two recent studies referenced the literature on humanising intensive care (Table 3).18,43
Discussion
The synthesis of data included for this qualitative systematic review confirmed the presence of humanising care defined as feeling recognised as a human being when experiencing connectedness with healthcare professionals, feeling connected with themselves and the situation when experiencing safety and well-being, and feeling connected with significant persons and life outside the ICU, and complemented this understanding by an additional theme: Experiencing capacity to influence the situation when being able to express themselves.
We searched for examples of humanisation of intensive care in a sample of Scandinavian literature where humanising and dehumanising care was not the focus of the studies and therefore not explored as such. Instead, the studies focused on different topics such as patient experiences of delirium,37,41 pain, 35 inner strength and willpower, 45 and communicating and being non-sedated during mechanical ventilation. 30 Even if humanising has not been explicitly addressed in the Scandinavian literature, a great deal of attention has been paid to how nurses can mitigate patients’ experiences of being critically ill and cared for in the ICU,18,20,31,34,36 which is closely aligned with how humanising intensive care is described in other parts of the world such as holistic care of the patient, as an attitude of professionals toward patients, and as an organisational trait enabling humanised care for all subjects of the healthcare system. 8 In this qualitative systematic review, attention to experiences in relation to intensive care may be influenced by the long practice of caring for non-sedated and non-restrained mechanically ventilated patients in the ICU which originated in Scandinavia around the turn of the millennium.35,62 Moreover, our review shows that caring for awake critically ill patients often calls for an understanding that the patients need human attention, comfort, kind touch, information, and communication, hence the concept of humanising was very much present, although not explicitly labelled as such.
The concept of humanising care including attention to patients’ human need for comfort, contact, and communication aligns well with the Nordic nursing tradition, which is rooted in an ethics of care, a philosophical and theoretical tradition influenced by the Norwegian nurse and philosopher Professor Kari Martinsen and Swedish/Finnish nurse and philosopher Professor Katie Eriksson. Martinsen and Eriksson have argued that care is and should be a prerequisite for good nursing. 63 An ethics of care is reflected in our findings, which emphasise the contact between the healthcare provider and the patient as essential for feeling human and maintaining a sense of self. From this perspective, nursing that is attentive to all the patients’ expressed and unexpressed needs may be a necessary condition for humanising intensive care.
Our qualitative systematic review, however, did not only reveal positive patient experiences of care. There were also patient descriptions of alienation, 20 isolation, 30 lack of control,33,34 and inability to communicate.29,36 These negative experiences may lead to feelings of dehumanisation. 10 Basile et al. 64 explored what contributed to humanising and dehumanising care in the ICU and found that dehumanising care was insensitive care, callous talk, and lack of involvement. Similar to our findings, humanising care included connecting with the patient, encouraging and empathic communication, touching with care, respecting the patient as an individual, and inclusion of family members. Basile et al. 64 underscored the importance of healthcare staff attitude and preparedness to engage with the patient in order to humanise intensive care. Rodriguez-Ruiz et al. 9 argued that harmonising relationships between patients, healthcare professionals, and family members is key to establishing humanising care. This involves open communication, information sharing, and active listening which may be facilitated by patient and family-centred rounds. Notably, the authors also list a number of additional, but resource-demanding strategies to humanise the ICU including healing gardens and music therapy. 9 While we do not disagree that such interventions may contribute positively to patient well-being, we consider ethical and caring engagement with the patient as the crux of humanising intensive care.
Our qualitative systematic review showed that most studies were discussed in light of other studies, and seven studies20,21,28,35,41,44,45 referenced the meta-synthesis of Nordic literature by Egerod et al., 14 which described the experience of intensive care as a liminal state between life and death, where the transition toward life is assisted by caring others. Egerod et al. 14 described patients’ fight for survival as requiring caring relationships, with compassionate and competent nurses offering protection and providing strength and a connection to the real world. Their study aligns with the synthesis of international literature by Nielsen et al., 11 in which humanising was described as feeling connected to healthcare professionals, oneself, the situation, and family members. Therefore, the findings of this review and Egerod et al. 14 indicate that parallel to the international humanising movement, Scandinavian literature has been preoccupied with the same problems, exploring patient lifeworld experiences from a mainly phenomenological and/or hermeneutical point of view. 14 This focus suggests a strong interest in understanding the ontology of being critically ill and describing this experience in terms of caring, passionate, and protecting relationships with patients despite not using the term humanising.
Four papers18,21,34,35 discussed their findings in relation to patient involvement, partnership, decision-making, and person-centred care. Patient involvement
65
and person-centred care
60
are concepts that overlap with the concept of humanising intensive care.
8
However, humanising intensive care transcends person-centred care as it is defined as both holistic care and a general attitude of professionals and healthcare systems toward patients, family members, and healthcare workers.3,8 Patient participation suggests involvement on professionals’ terms, while person-centred care is more holistic
60
; although both are inherently positive
Limitations
This qualitative systematic review was built upon a search strategy ensuring that all literature studies were found and included. Furthermore, data extraction and analysis were undertaken by all three authors in collaboration, strengthening the internal validity of the study. The included sample allowed us to broaden our understanding of what humanising intensive care is. Literature was included from the year 2016, which marks the inception of the humanising ICU literature. 8 The Scandinavian research tradition, however, is longer, and not including literature from before 2016 limits our ability to explore the fundaments of Scandinavian ICU patient experience research prior to year 2016. Thomas and Harden 15 favour a representative sample over an exhaustive sample, and by including 29 very different studies, we have achieved that. We did not include studies from Finland, which is a limitation given that Finland and Scandinavia have comparable healthcare systems and a shared tradition of nursing theory.67,68
An advantage of thematic synthesis 15 is that findings remain close to the data reported in primary studies, but the method has also been criticised for its lack of transparency. 69 We have therefore provided examples of the coding process and supported all findings with examples from the studies included to provide transparency of the analytic process.
Conclusion
This qualitative systematic review expands the understanding of humanising intensive care as an ethical and caring engagement with the patient which helps the patients feel connected, experiencing well-being and being able to influence their situation. Although the Scandinavian literature has not studied humanising per se, it has engaged with the idea by focussing on improving patients’ situations, influenced by a strong desire to understand the ontology of critical illness. In Scandinavia, humanising intensive care is rarely used as a concept; however, the ideas behind it are strongly present in Scandinavian literature and align well with the Scandinavian nursing tradition.
Supplemental material
Supplemental material -
Humanising care in Scandinavian intensive care units – A systematic review
Supplemental material for Humanising care in Scandinavian intensive care units – A systematic review by Monica Evelyn Kvande, Sanne Angel, and Anne Højager Nielsen in Nursing Ethics.
Footnotes
Ethical considerations
All included studies had undergone relevant ethical approval and were publicly available.
Author contributions
MEK
Funding
All support for the study was supplied by study investigators in-kind.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.