
Abstract
Background
Disclosure of information that identifies deceased organ donors and/or organ transplant recipients is prohibited in many countries, including Australia. Anecdotal evidence suggests that some donor family members and transplant recipients desire and independently establish contact using strategies such as social media.
Objective
To describe and synthesise the views of Australian donor family members, transplant recipients, and healthcare professionals regarding the disclosure of identifying information between donor family members and transplant recipients.
Research design
An exploratory descriptive qualitative study design was used.
Participants and research context
Semi-structured interviews were conducted with 23 donor family members, 25 transplant recipients, and 16 healthcare professionals. Interviews were audio recorded and transcribed verbatim. Data were extracted and synthesised using thematic analysis.
Ethical considerations
This study was approved by the Human Research Ethics Committee of Griffith University, Queensland. Participation was voluntary, and informed consent was obtained from all participants.
Findings
Three themes were revealed: (i) a desire for choice, (ii) perceptions of benefits, and (iii) perceptions of risks and risk mitigation. Some donor family members and transplant recipients would like the choice to pursue identifiable contact, and for this to be facilitated by donation agencies and transplant units. Many healthcare professionals also support the notion of choice.
Conclusion
Current Australian laws prohibit the disclosure of information identifying deceased organ donors and transplant recipients to each other. Any desire to amend existing laws would necessitate a thorough consultation process and the establishment of suitable systems and processes to support identity disclosure. Further research is needed to ascertain options for identifiable contact and to identify strategies to maximise benefit and minimise harm for donor family members and recipients.
Introduction
Anonymity in organ donation is a legal requirement in many countries, which means disclosure of identifiable information about donors and transplant recipients is prohibited. The law in Australia requires health professionals (and, in some cases, other individuals) to maintain the anonymity of organ donors, their families, and transplant recipients. 1 Despite these prohibitions, some Australian donor family members and recipients have advocated for formal mechanisms to enable mutually agreed, identifiable contact. 2 However, there is little research that explores the view of those most impacted by the law. Our study seeks to identify, describe, and synthesise the views of Australian donor family members, transplant recipients, and donation and transplantation healthcare professionals regarding disclosing information to facilitate identifiable contact between donor family members and transplant recipients.
Background
In 1977, the Australian Law Reform Commission was tasked with recommending laws for the removal of human organs and tissues for medical and scientific purposes. 3 The Commission’s report recommended standardising legislation across states and territories. At the time, organ transplantation was emerging in Australia and received considerable media attention, resulting in the media publicly identifying an organ donor and transplant recipient in violation of an agreement with a hospital. 3 The Commission observed that such media exposure, coupled with breaches of confidentiality by healthcare professionals, led to a decline in kidney donations. 3 As a result, it recommended that the privacy and confidentiality of organ donors, transplant recipients, and their families be safeguarded. These recommendations were incorporated into Australian state and territory laws, such as the Human Tissue Acts or similar legislation.
The legal right to privacy and protection of personal information is regulated by the Privacy Act 1988 (Cth). 4 The ethical requirement to maintain confidentiality and safeguard personal information that is not publicly available is also protected by common law. Some Australian jurisdictions, such as Victoria, have additional confidentiality protections under the Health Services Act 1988 (Vic). 5
In Australia, organ donation is an opt-in system regulated by state and territory Human Tissue Acts or similar legislation. The Australian Organ and Tissue Donation and Transplantation Authority was created in 2008 by the Commonwealth Government to improve organ and tissue donation and transplantation outcomes. The Authority’s functions are outlined in the Australian Organ and Tissue Donation and Transplantation Authority Act (2008) (Cth), 6 including the implementation of a national deceased organ donor coordination ‘DonateLife’ Network. 7
A review of the international literature demonstrated differing opinions on identity disclosure between donor family members and transplant recipients. 8 Previous Australian studies have demonstrated that donor family members desire personal communication, 9 and feel comforted by receiving anonymous correspondence from recipients. 10 Some donation agencies in the United States, 11 Israel, 12 The United Kingdom, 13 and parts of the European Union 13 have implemented processes for donor family members and recipients to pursue identifiable contact following the consent of both parties.11–13 Other studies highlighted the varying perspectives of healthcare professionals regarding identity disclosure between donor family members and transplant recipients. For example, some physicians 14 and transplantation coordinators 15 prefer to maintain anonymity, emphasising that identifiable contact may lead to emotional conflict or financial involvement, whereas others have neutral perspectives about identifiable contact. 16
The advancement of social media over the last two decades offers people the potential to identify a donor, their family, or a transplant recipient independently of established support systems.17–20 Sharing identifiable information on social media without professional assistance, such as the presence of trained mediators, counselling, or a formal mutual consent register, may expose donor family members and transplant recipients to increased risks than when contact is facilitated by regulated agencies.17,21 However, the extent to which sharing identifiable information on social media occurs is unclear.
Anonymised written correspondence between donor family members and transplant recipients is facilitated by healthcare professionals. However, a recent Government review recommended a national process for donor family members and adult transplant recipients to be identified with each other based on the principle of mutual informed consent. 22 A detailed exploration of the views of key stakeholders in donation and transplantation is required to inform potential policy changes.
Identity disclosure in the context of this study is defined as an individual whose identity is apparent, or can reasonably be ascertained for example, name, age, gender, geographical location, or physical appearance. Identity disclosure may extend to being contactable via social media. However, some individuals are satisfied with the option of receiving additional information which may identify/humanise the other party, but there is no intention to initiate contact.
Objective
The objective of this study was to identify, describe, and synthesise the views of Australian donor family members, transplant recipients, and donation and transplantation healthcare professionals regarding disclosing information to facilitate identifiable contact between donor family members and transplant recipients.
Method
Design
An exploratory descriptive qualitative design was used to explore the phenomena of interest, which were the beliefs, attitudes, and perceptions relating to identity disclosure or anonymity from individual perspectives, including donor family members, transplant recipients, healthcare professionals, and policymakers.
Participants and setting
Inclusion criteria.
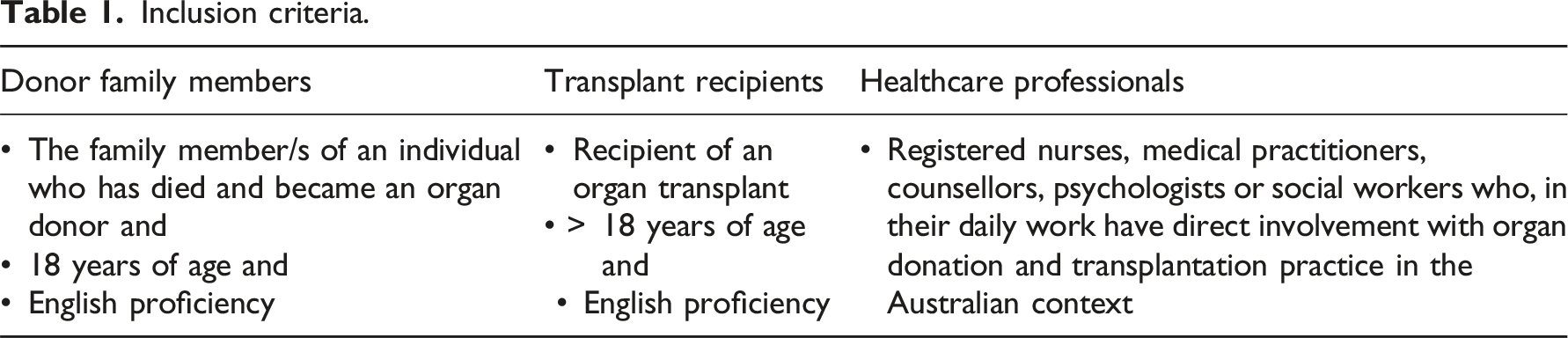
Data collection
A semi-structured interview guide was developed by the researchers based on an existing literature review 8 that included questions about the perceived advantages and disadvantages of identity disclosure, current use of social media by individuals seeking identifiable contact, potential features of a direct contact programme, support for donor family members and recipients, and current laws and policies. Feedback on interview questions was provided by a consumer representative with experience in organ transplantation and a medical expert in organ donation. Interviews were conducted between June and September 2022 via telephone or videoconferencing using Microsoft Teams to capture participants in all states/territories and alleviate exposure risks associated with the COVID-19 pandemic. All 98 individuals who expressed interest in participating were offered an interview opportunity. However, 34 did not respond, resulting in a final participant count of 64. Interviews were recorded and transcribed verbatim by a university-certified speech-to-text transcription service. Accuracy was checked by listening to the interviews while reading the transcripts, and any identified errors were corrected.
Data analysis
Demographic data were reported using descriptive statistics. Interview data were textually analysed using NVIVO software. Colloquial terms such as ‘you know’ and repetitive words were removed from quotes for clarity and brevity. A six-step approach to thematic analysis adapted by Braun and Clarke 23 was used to facilitate analysis and included (1) data familiarisation, (2) coding, (3) initial theme generation, (4) theme review, (5) theme definition, and (6) writing of results. Themes associated with individual perceptions of identity disclosure were identified, extracted, and categorised from the dataset.23–25
Trustworthiness criteria, including credibility (AC, AM, JH, HO, KR), transferability (AC), dependability (AC, AM, JH, HO, KR) and confirmability (AC), were applied.26,27 Credibility was achieved through continuous discussion of findings amongst the research team. Transferability was obtained by documenting the processes throughout the data collection and providing a detailed description of the findings. Dependability was maintained through continuous peer review of the data analysis process by experienced researchers, an independent clinical expert in organ donation, and a consumer representative. Maintaining detailed notes and interview contact summaries ensured confirmability.
Ethical considerations
This study was approved by Griffith University Human Research Ethics Committee (**Ref No: 2021/823). Participation was voluntary, and informed consent was obtained from all participants before commencing each interview. Participants were informed that they could withdraw from the study at any time and that their data would be securely stored. 28
Findings
One hundred people responded to the study advertisement. Twenty-three donor family members, 25 recipients and 16 healthcare professionals agreed to an interview. Thirty-six people did not respond to a follow-up invitation. Interviews ranged from 20 to 60 minutes (average of 45 minutes).
Demographic characteristics of the study population.
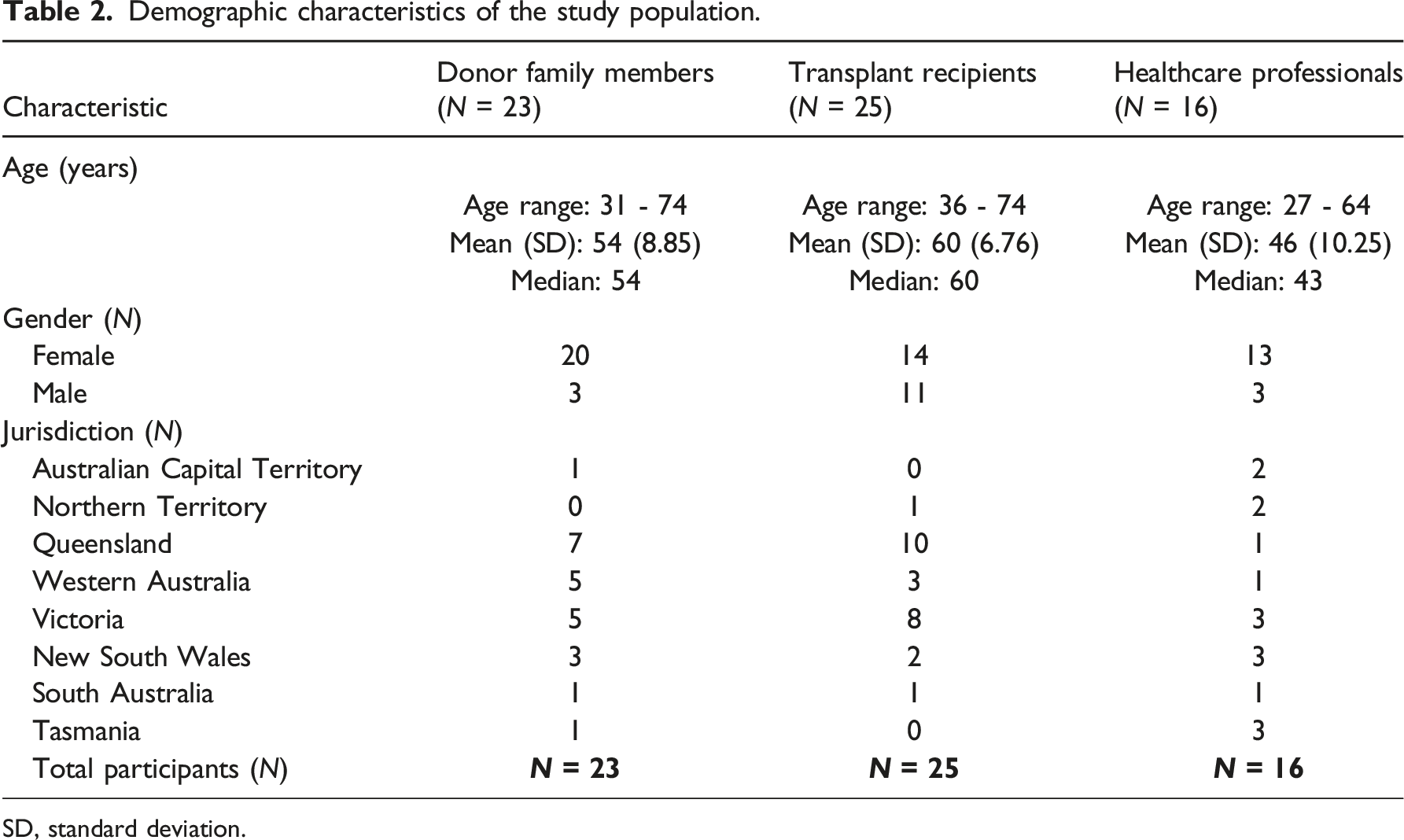
SD, standard deviation.
Healthcare professional participants.
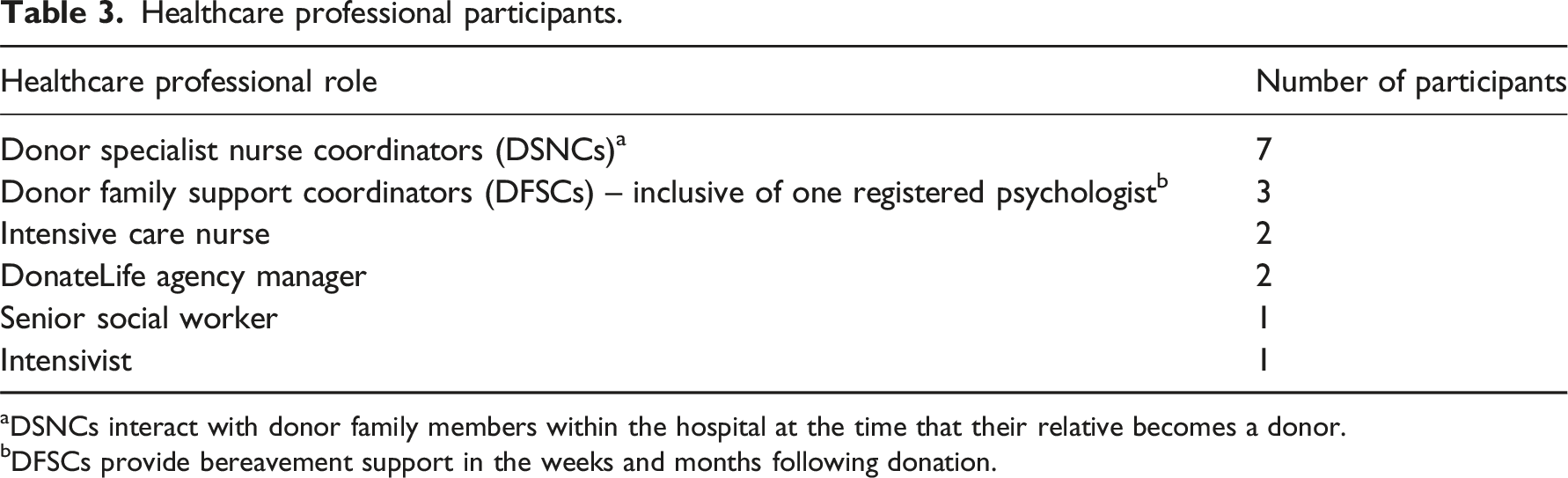
aDSNCs interact with donor family members within the hospital at the time that their relative becomes a donor.
bDFSCs provide bereavement support in the weeks and months following donation.
Theme 1: Desire for choice
Many participants supported the notion of choice and acknowledged that current systems restrict choice. Donor family members were more supportive of choice, with many stating that identity disclosure ‘…should be up to those people, the donor family, and the recipient to make their own choice…’ (DF51) in the same way that ‘…being a donor is a personal preference… there should be a choice where you can say, yes or no…’ (DF67), and if ‘…both parties are in agreement, who can stop that?’ (DF72). Others stated that it should not be’…up to outside parties to decide when a donor family or when a recipient is ready to meet each other’ (DF52). Donor family members expressed frustration with having no avenue to pursue identifiable contact; ‘…it is up to those people, the donor family and the recipient to make their own choice… there is no choice at the moment. It’s just like there’s nothing’ (DF51).
Some donor family members advocated for choice as exists within other contact frameworks; ‘Oh look, absolutely! I mean all this hoo-ha and the secrecy. It’s like adoption. You’ll consult consenting adults, now if they want to meet up, they’ve got every right to’ (DF42).
Supporting the idea of choice is also important for some transplant recipients and would provide them with an opportunity ‘…to thank those people to say well you’ve lost a loved one, but you’ve given a life to somebody else’ (TR14). However, there was more hesitancy among transplant recipients who stated, ‘I do not think it would be a good idea for our family’ (TR22). The main reason for wanting to maintain anonymity included the fear of disappointing the donor family. For example, one participant stated:
‘I feel that it could really disappoint my donor family to know that I’m not some sort of cheery grandparent or athletic person, or someone’s about to have a baby or some kid at school because they’re the pictures that we’re fed of who recipients are’ (TR11).
Some recipients expressed concerns about exacerbating the grief of donor family members who may perceive that their loved one continues to live in the recipient. For this reason, some recipients conveyed that they would not’…go down the route of knowing the [donor] family members because I feel that they would associate me with their deceased’ (TR20).
Healthcare professional participants expressed support for identifiable contact where there are ‘…two consenting adults, who are fully informed of the risks and the benefits of communicating with each other…’ (HP07) and acknowledged that eventually ‘…we sort of have to allow that to happen’ (HP07).
Participants in each group identified that current laws prohibiting identity disclosure were problematic. Healthcare participants generally expressed this sentiment by describing the current system as’…a bit too government-like and restricting people from doing things when they’re able to consent to doing them’” (HP07). The intent of current legislative requirements in protecting anonymity is widely understood, however, ‘…the question that’s coming up all over the world is; what right do people have to share their information if they choose to?’ (HP98). One healthcare professional suggested that Australia could work around existing laws by introducing ‘…an internal process that circumvents legislation in the Australian States and territories…’ (HP05).
Some healthcare professional participants expressed support for the implementation of a professionally trained service that could enable donor family members and transplant recipients to register their consent for sharing identifiable information. The service could also facilitate the exchange of identifiable information between the two parties if requested; ‘I believe that our agency has an obligation to at least verify or deny [identifiable information]… (the organisation) does not provide this service but I believe they should’ (HP101).
Many donor and recipient participants expressed that ‘…the donor and recipient contact process needs to be totally rewritten…’ (DF72) with some recipients sharing that ‘…we need a way of people choosing whether they want to meet or not, and the ones who want to meet, their wishes should be respected’ (TR50).
Theme 2: Benefits of identity disclosure
Transplant recipients acknowledged that identifiable contact may enable individuals to express their gratitude in a personal and meaningful way. For example, one recipient stated, ‘I’d like to be able to say thank you to these people… for my own sense of well-being… even having a name, that would really help me, but knowing who the person was would make me feel a lot better’ (TR80). Others agreed that ‘…it’s a lot better face-to-face to give your appreciation…’ (TR28) and to ‘…put a face to a name…’ (TR35). Some recipient participants thought that identifiable contact could provide donor family members with ‘…a greater sense that their loved one has helped somebody… they can see what their loved one has done’ (TR09). This view was shared by donor family members who expressed the perceived benefit of witnessing‘…their [recipient] lives have changed… it adds a personal nature to it’ (DF37). Furthermore, identifiable contact may help to reinforce the donation decision for donor family members, by seeing that ‘someone has got something out of such a hard time for us’ (DF43).
Many participants thought identifiable contact may provide opportunities for meaningful connections; ‘…you could make fantastic friendships’ (TR09) while others highlighted the potential for identifiable contact to ‘…acknowledge who they [donor] were in a different way’ (TR47). Meaningful connections may soften grief, as shared by one donor family member who commented that’…to meet someone who has received part of my child that has given them a better life, seeing something beautiful come out of a tragedy, I think it would really help me get some closure’ (DF67). Others agreed that ‘…the positives…very healing absolutely… it heals you know, it heals’ (DF52).
Healthcare professionals conveyed that identifiable contact may offer comfort to some donor family members, enabling them ‘…to see that the death of their loved one wasn’t futile, that it was meaningful in someone else’s life and family I think would give great comfort and solace’ (HP97). In addition, providing donor families an opportunity to ‘…share who their loved one was, their interests, and celebrate them. It’s very meaningful and powerful and another way to acknowledge the death’ (HP95). For recipients, identifiable contact may ‘…promote compliance… in terms of someone’s recovery’ (HP17).
Overall, many participants highlighted the enriching opportunity for donor family members and recipients who wish to pursue identifiable contact, suggesting that ‘…it’s such a rare opportunity in life that people get on both sides that it could be quite enriching’ (DF41).
Theme 3: Risk and risk minimisation of identity disclosure
All participants acknowledged a level of risk associated with identifiable contact. For example, donor family members and transplant recipients expressed concern about the risk of mismatched expectations regarding frequency of contact, invasion of privacy, fear of rejection, and misaligned values, which may result in disappointment.
Donor family members were apprehensive about the risk of exacerbating their grief because ‘…if your loved one has donated an organ and you’re very emotionally and mentally attached to the outcome of this, then having outcomes that maybe might not be your ultimate vision… can be hard to take’ (DF71). In the context of a face-to-face meeting, ‘…it could be heartbreaking if you meet these people and you realise that they’ve gone back to their ways if that was the reason why their organ failed…I think that would crush me personally’ (DF83). Another donor family member shared concerns that ‘… if they’re [recipient] not doing the right thing, I think I would just be so angry and toxic’ (DF49). One healthcare professional reported a donor family member ‘…now feels like this heart recipient is like her son…and sharing her whole world with him’ (HP99). Some transplant recipients shared the risk of survivor guilt by knowing the identity of their donor and a sense of obligation to live their best life post-transplant; ‘…there’s a guilt that I have to carry… about being alive, you know the responsibility that someone died, and I have to now live a good life to make up for that’ (TR29).
Donor family members, transplant recipients, and healthcare professional participants acknowledged that identity disclosure in the event of law reform may still risk psychological harm, even if systems are implemented and managed effectively by trained professionals. Thus, it is pertinent to identify strategies to mitigate potential risks and improve outcomes for parties who may choose to pursue sharing identifiable information.
Risk minimisation strategies were suggested by several participants. For example, establishing a system that allows individuals to ‘…register their interest… like an adoption register…’ (TR46)’…where people can either say yes or no…’ (DF67) or ‘… opt-in on both sides’ (TR20). Additional strategies voiced include the provision of counselling services for individuals who opt-in, drawing on invitro fertilisation experience where ‘…you gotta have your counselling… make sure that you’re not gonna be destroyed by the information you find out…’ (DF49), be provided with ’…someone to mediate that meeting… a trained person…’ (TR23), and reassurance that either party can’…withdraw consent at any time’ (HP05).
It was suggested that existing programmes that facilitate contact between adult adopted children and their biological parents, or donor-conceived children with their biological donors, could be adapted to the organ donation and transplantation sector to eliminate risks. As one transplant recipient highlighted, ‘I would like to see it [identifiable contact] as the adoption model or the sperm donor or the egg donor’ (TR23).
Some transplant recipients advocated for a time period before identity disclosure, noting that ‘…a six-month period… so that you could get a feel for the other party’ (TR47) might be appropriate. A period of adjustment to life post-transplant is often required, as illustrated by one participant who commented ‘You go through a range of emotions. And that’s why I think contact between the two parties could be delayed for at least two years afterwards after patients are no longer under the effects of medications’ (TR24).
The perceived risks associated with identity disclosure in the context of current systems pose unique challenges for healthcare professionals who may feel obligated to support donor family members and transplant recipients seeking identifiable information. One healthcare professional shared that in some cases, ‘…they [donor family members]…request that I assist them in finding their recipient family so that they can link up and obviously I’m bound by the legislation that I’m unable to assist’ (HP100). An inability to assist donor family members and transplant recipients seeking identifiable information creates tension between patient advocacy and the reality of practice because ‘…we’re completely restricted by law’ (HP97).
Many healthcare professionals expressed the need for law reform, guideline development, ongoing regulation, and resource availability to support donor family members and transplant recipients’ requests for identifying information. For example, one participant opined, ‘…there would definitely have to be some governing body to control it [identifiable contact]’ (HP94). This would enable healthcare professionals to continue supporting donor family members and transplant recipients within ‘…a framework that allows people to seek the information’ (HP06).
Overall, the need to identify and address the risks involved with identity disclosure is important because ‘…we owe it to our donor families and our recipients to do it properly’ (HP97).
Discussion
The findings of this study highlight the views of Australian donor family members, transplant recipients, and healthcare professionals about the disclosure of identifying information between donor family members and transplant recipients. Three themes were revealed: (i) a desire for choice, (ii) perceptions of benefits, and (iii) perceptions of risks and risk mitigation.
Some donor family members and transplant recipients desire a choice to share their personal information, noting this carries potential benefits and risks for both parties. Similarly, donor family members and transplant recipients expressed a preference for the option of identifiable contact, even if this is not pursued.
Identifiable contact is available to donor family members and transplant recipients in some international jurisdictions.11–13,29 A recent legislative proposal in Italy aimed at allowing identifiable contact between donor family members and transplant recipients was unsuccessful in the Italian parliament. Nonetheless, public opinion in Italy remains supportive of the choice for identifiable contact. 30 A 2022 study about contact between donor families and recipients in 15 European countries revealed that a formalised process for donor family members and recipients to meet face-to-face is available in the Netherlands, Sweden, Belgium, and the United Kingdom. 13 However, circumstances vary based on local laws and processes and remain a subject of ongoing discussion.
Our research indicates support among some members of the Australian donation and transplantation community for a choice regarding identifiable contact between donor family members and transplant recipients. This is consistent with previous studies where donor family members and transplant recipients have highlighted the value of choice.2,31 Additionally, in the context of identifiable contact between donor family members and transplant recipients, there is an increasing need for practical strategies to protect individuals right to privacy while providing opportunities for individuals to pursue autonomous choices about the extent of contact in the context of mutual and informed consent.
In this Australian study, healthcare professionals supported a legislative change so that adult donor family members and transplant recipients could choose whether to share identifying information and the potential for initiating direct communication. This finding differs from healthcare professional perspectives in previous and Brazil, 14 where preferences tended towards systems that maintained anonymity.
The fundamental ethical principles of autonomy, beneficence, non-maleficence, and justice are reflected in the National Safety and Quality Health Service Standard, partnering with consumers. 32 Respect for autonomy recognises a person’s right to choose based on their values and beliefs. The tension between fostering autonomy and constraints imposed by current systems is a challenge for some healthcare professionals who are only legally permitted to assist donor family members and transplant recipients by forwarding anonymised correspondence via the donation agency or transplantation unit. In circumstances involving deceased donation, healthcare professionals may feel the need to act as an advocate for donor family members seeking more information about transplant recipients. However, in practice, the law restricts their ability to do so, posing practical challenges for healthcare professionals who may feel obligated to assist with donor family members and transplant recipients’ requests for identifiable information but remain confined by legal requirements 33 and are therefore unable to assist with requests for additional information that may reveal the identity of a donor, their family, or the recipient/s. Additionally, while aiming to protect identity, current laws also prevent individuals from exercising their autonomous choice to be identified.
Frameworks for contact decisions in gamete donation and adoption cases34–39 may guide deceased organ donation and transplantation. In Victoria, Australia, the consent model balances donor-conceived individuals’ access to donor information with donors’ preferences for anonymity.36,38,39 The Victorian Assisted Reproductive Treatment Authority (VARTA) enforces legally binding contact preferences through a central and voluntary Register. 40 This model promotes information exchange via education, awareness, and counselling 39 and could support identity disclosure in organ donation. Empowering decision-making measures is preferable to limiting choice. 39
Our findings reveal that participants perceive several potential benefits of identifiable contact. Donor family members voiced that identifiable contact may provide comfort during their grief. These findings are consistent with existing literature, which suggests that identifiable contact may provide comfort for grieving donor family members.10,41,42 Similarly, transplant recipients may convey their appreciation in a personalised manner11,43, thereby alleviating feelings of survivor’s guilt.41,44,45
Perceived risks to donor family members and transplant recipients include mismatched expectations, invasion of privacy, fear of rejection, misaligned values, and exacerbating grief. Transplant recipients were generally more reticent about identifiable contact than donor family members and suggested that certain measures be implemented to ensure their safety.
These findings are consistent with the risks of identifiable contact highlighted in existing literature, including transplant recipient survivor guilt for having their life prolonged by the death of another person12,43 and concerns about causing emotional distress 9 or disappointment for the donor family. 46 Transplant recipients who have experienced unsuccessful transplants or those who require liver transplants due to alcoholic liver disease may also fear disappointing donor family members. 47 Donor family members are informed about the outcome of organ donation, including circumstances where donation did not proceed. For example, in 2023, among the 793 deceased organ donors in Australia, 513 proceeded to donation, while 280 did not complete the donation process due to medical or logistical reasons. 48
The risk of psychological harm will be minimised by a well-implemented system; however, not all risks can be eliminated. 41 Potential risks include loss of privacy, harassment, stalking, extortion, and misidentification, tension between one party desiring anonymity and the other desiring identifiable contact and unmet expectations, resulting in disappointment.2,14,16 Embarking on identifiable contact without knowledge of potential risks and benefits may also introduce risks. 2 Previous research highlights that there is considerable interaction between cultural and social beliefs on the decision to endorse organ donation. However, further research is required in the Australian context to ascertain the influence of socioeconomic status and cultural diversity on decision-making about contact between donor family members and transplant recipients. 49
Several risk minimisation strategies were proposed by participants in this study. Notably, implementing controlled communication channels, establishing formal support networks, offering tailored guidance from healthcare professionals, and the need to consider cultural differences that may impact choices. Additionally, strategies in the context of legislative and/or policy change to permit a waiver of anonymity in a donation and allow identifiable contact include a national contact registry, implementing a designated waiting period before identifiable contact is allowed, offering individual counselling both before and after contact, the presence of a trained intermediary during face-to-face interactions, and ensuring participants can withdraw their consent at any time.
These findings are consistent with outcomes from a community consultation forum held in Melbourne, Australia 2 and the international literature. Donor family members and transplant recipients emphasise the importance of being informed about strategies to safeguard their identity and evidence-based guidelines or advice for those who choose to independently pursue identifiable contact, within the framework of current laws. 2 In the event of legislative changes, a national contact program that is developed and maintained by a government agency may further reduce risks.2,15,31 This program could provide counselling and emotional support 50 as well as an independent facilitator during face-to-face meetings.2,12,51 Importantly, any contact should not be imposed and providing support for individuals to protect their identity if desired is crucial.2,31
Risk minimisation strategies are implemented by donation agencies in the USA 11 and Israel. 12 For example, donor family members and transplant recipients may pursue identifiable contact following mutual agreement of both parties in writing. All individuals are supported by pre and post-meeting discussions facilitated by the donation agency to address the potential risk of mismatched expectations.11,12 The Israeli Transplant Centre demonstrates some donor families’ desire to maintain contact with the transplant recipient. 12
In Australia, evidence suggests that social media and other mechanisms, for example, a donor-recipient contact register maintained by a voluntary organisation, Donor Families Australia, 52 enable identifiable contact without any framework for harm minimisation. Although there may be some risk with modifying the law to readily allow contact, there is also a risk with maintaining the status quo. However, formalising this initiative requires sufficient funding and resources to optimise benefits and minimise harm.
Strengths and limitations
This qualitative study builds on previous Australian work exploring identifiable contact in organ donation. 2 Additional strengths include the large sample size, volume of data generated, and representation from all Australian jurisdictions. While a rigorous and structured approach was used to identify themes, those who volunteered to participate in this study may hold strong views about direct donor family and recipient contact, resulting in a skewed sample not representative of the broader donor family and recipient population. This study focuses exclusively on jurisdictions that employ positive (opt-in) consent systems. Similarly, healthcare representation included a range of practitioners with various roles in the donation and transplantation sector, but may not be representative of all relevant clinician views. An additional limitation of our study was the absence of representation from culturally and linguistically diverse participants and an inability to identify participants who identify as Aboriginal and/or Torres Strait Islander.
Conclusion
This study highlights a growing desire for choice among some members of the donation and transplantation community while also recognising the importance of balancing perceived benefits and minimising risks. Healthcare professionals also support the notion of choice in this matter. However, Australian laws and current systems in many jurisdictions prohibit the disclosure of information that would allow for the identification of deceased organ donors and transplant recipients. The findings demonstrate a need for policy development and practical strategies to protect individuals right to privacy while providing opportunities for individuals to pursue choices in the context of mutual and informed consent. Risk perceptions and risk minimisation strategies underscore the need for a balanced approach to risk versus the potential benefits of exchanging identifiable information. A more detailed exploration of the spectrum of societal views, as well as the potential benefits and risks, is required before recommending a change to the law or current process. Any change would also require the development of processes and the investment of resources. This presents a challenge for healthcare professionals when supporting donor family members and recipients who may seek identifiable information. The challenge remains in developing a system that respects individual autonomy while simultaneously addressing concerns about potential risks associated with identity disclosure. There is a need to explore and determine the conditions under which the disclosure of identifying information may occur for the benefit of all parties. Further research is also needed to improve the outcome for individuals who may pursue identifiable contact.
Footnotes
Acknowledgements
The authors wish to acknowledge the generosity of individuals and their families who agreed to organ donation, and we thank all participants who volunteered to participate in this study. We also thank Pam Ingram for their contribution to this study.
Author contributions
For all articles, the journal mandates the CRediT (Contribution Roles Taxonomy), for more information please see ![]() . Anthony Cignarella: Conceptualisation (equal); formal analysis (lead); methodology (equal); writing – original draft preparation (lead). Andrea Marshall: Conceptualisation (equal); methodology (equal); supervision (equal); writing – original draft preparation (supporting); writing – review and editing (equal). Jayne Hewitt: Conceptualisation (equal); methodology (equal); supervision (equal); writing – review & editing (equal). Helen Opdam: Conceptualisation (equal), writing – review & editing (supporting). Kristen Ranse: Conceptualisation (equal); methodology (equal); supervision (equal); writing – review and editing (equal).
. Anthony Cignarella: Conceptualisation (equal); formal analysis (lead); methodology (equal); writing – original draft preparation (lead). Andrea Marshall: Conceptualisation (equal); methodology (equal); supervision (equal); writing – original draft preparation (supporting); writing – review and editing (equal). Jayne Hewitt: Conceptualisation (equal); methodology (equal); supervision (equal); writing – review & editing (equal). Helen Opdam: Conceptualisation (equal), writing – review & editing (supporting). Kristen Ranse: Conceptualisation (equal); methodology (equal); supervision (equal); writing – review and editing (equal).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.