
Abstract
Background
Ethically challenging situations often arise in interactions between healthcare professionals (HCPs) and families. Although the Calgary models offer guidance for practical work and are beneficial in various challenging situations, explicit awareness and recognition of the ethical concepts and theories underlying Family Systems Care (FSC) is generally lacking.
Method - Research aim
This study examined the basis of FSC in virtue ethics, deontology, and teleology.
Research design
Utilizing a qualitative design, an expert consensus was conducted through two focus group interviews, a Delphi group, and an expert panel.
Participants and research context
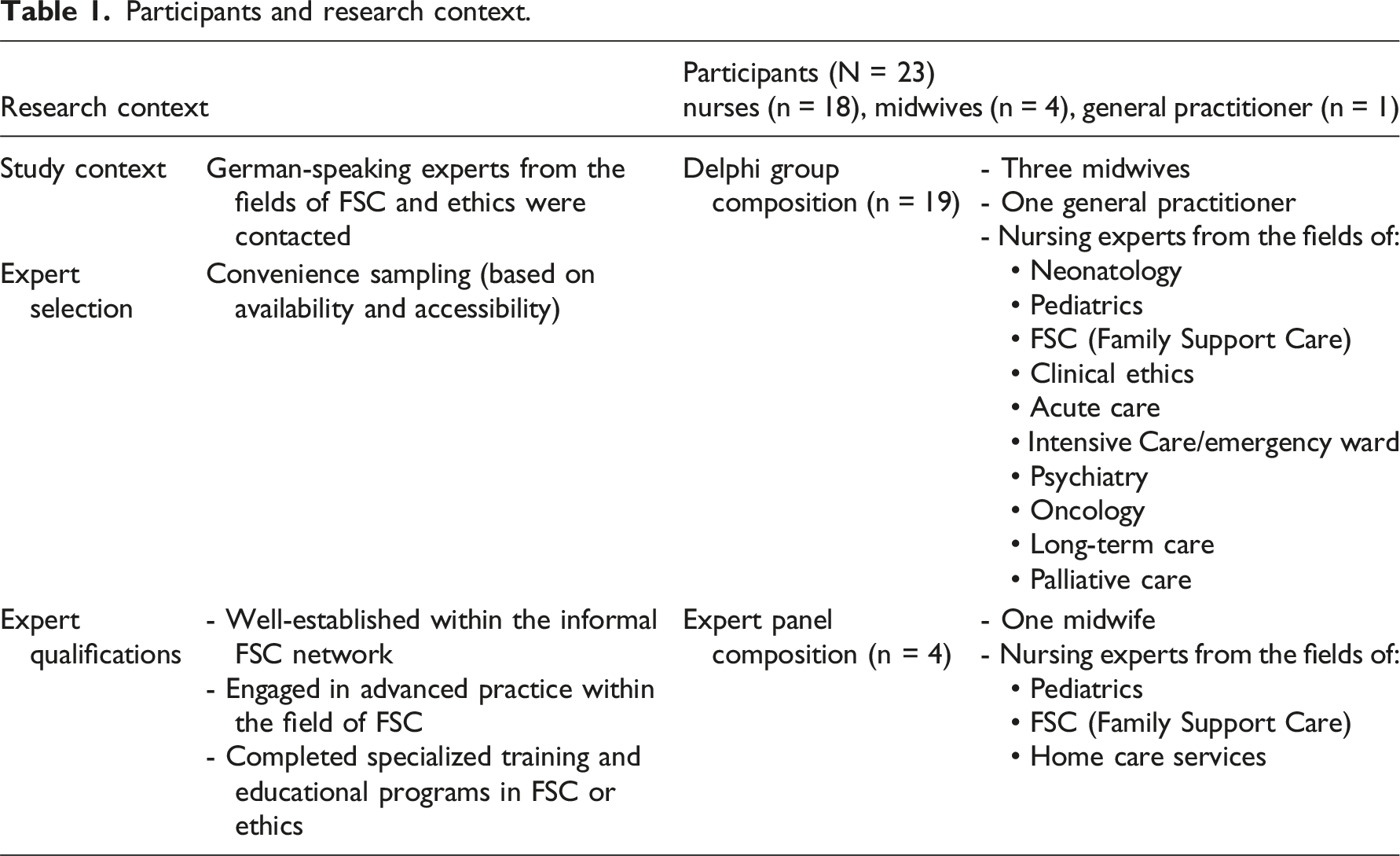
The expert consensus consisted of 23 professionals in FSC from various specialities, including nurses (n = 18), midwives (n = 4), and a general practitioner, who explored ethical considerations in clinical practice.
Ethical considerations
The research project was conducted in accordance with the ethical principles of participants’ informed consent and the Declaration of Helsinki.
Findings
Participants recognized the significance of classical virtues such as faith, fortitude, hope, and caritas in FSC. They emphasized that these virtues not only guide HCPs in their practice but also empower families to rediscover their strengths amid suffering. Additionally, the integration of deontological principles and teleological perspectives highlighted the importance of balancing individual and collective well-being, and fostering compassionate relationships while navigating ethical complexities in therapeutic conversations.
Conclusion
This study highlights the importance of virtue ethics, deontology, and teleology in guiding HCPs’ moral reasoning within FSC. Participants emphasized respect and appreciation as essential values for maintaining trust with families during ethical challenges. By integrating ethical theories into practice, HCPs can navigate complex situations effectively, fostering compassionate and dignified care.
Keywords
Introduction
Interactions between family members and healthcare professionals (HCPs) in clinical settings can lead to challenging situations where ethical theories are either intentionally applied or implicitly relevant. In daily clinical practice, ethical conflicts may cause HCPs to distance themselves from families.1,2 Such conflicts often precede moral distress 3 and can lead to physical, psychological, social, and spiritual suffering among nurses, ultimately resulting in burnout. 4 In 1998, Tuckett described the challenge for nurses in particular to find a balance between responding ‘with a sense of compassion’ and ‘adhering to a rule at all costs’ (p.225). Based on virtue theory, utilitarianism, and deontology, he outlined a conceptual ethical framework for nurses in practice. 5 These ethical approaches are essential for developing ethical awareness in nursing and support HCPs in making informed decisions that respect both patient needs and professional standards.
As general guidelines and thus also for ethical orientation in both standard and advanced family nursing practice, the most widely used set of models is the ‘Calgary models’, 6 pioneered by Lorraine M. Wright, Maureen Leahey, and Janice M. Bell for Family Systems Nursing. These models are multidimensional with the aim to maintain, promote, or restore the health of the family. 8 Structural, developmental, and functional aspects of the family situation (CFAM) are used to identify strengths and resources, as well as difficulties and illnesses. 6 The CFIM offers cognitive, affective, and behavioural interventions for nursing conversations with families. 6 Through commendations and circular questions, CFIM enables nurses to facilitate a context in which the family and its members can find their own solutions to problems. 8 The IBM addresses the illness beliefs of patients, family members, and HCP and their role in promoting family health. 7
Although Wright et al. 6 and Wright and Levac 9 have mentioned ethical and theoretical concepts, there appears to be a lack of active mention and explicit awareness of the ethical concepts and theories underlying Family Systems Care (FSC). While several studies address specific ethical issues in the application of FSC,8,10–13 its grounding in ethics remains only vaguely described. Burchard, 8 for example, argues that engaging with ethical considerations can enhance the conceptual understanding of FSC and increase the awareness of relationship-oriented work with families. This is essential for nurses who engage with families on a daily basis and highlights the need for systematic reflection on ethics among HCPs working with FSC. While Burchard 8 discusses the connection between teleology and the FSC, however – two principal areas of ethical thought crucial to nursing practice – virtue ethics and deontology were not considered.
Research aim
Through exploration in expert consensus, this study seeks to identify and deepen the understanding of the ethical dimensions that underpin the application of FSC in clinical settings, focussing on virtue ethics, deontology, and teleology as central ethical theories already recognized as relevant to good nursing practice. The FAMETHI project (FAMily System Care and ETHIcs) addresses the question of ethically challenging situations in working with families, the ethical philosophies considered normative by HCPs, and how this knowledge can enhance family-focussed, systemic daily work and multilateral family counselling. This article focuses on ethical theories – virtue ethics, deontology, and teleology – based on the practical experiences of HCPs involved in the project, while additional topics are covered in a supplementary paper.
Methods
Research design
The FAMETHI research project utilized expert consensus from professionals with experience in Family System Care (FSC) to explore the intersection of FSC and ethics. A qualitative design was employed, incorporating focus group interviews, a Delphi process, and expert panel meetings to gather diverse perspectives.
Participants and research context
Participants and research context.
Content of the survey rounds.
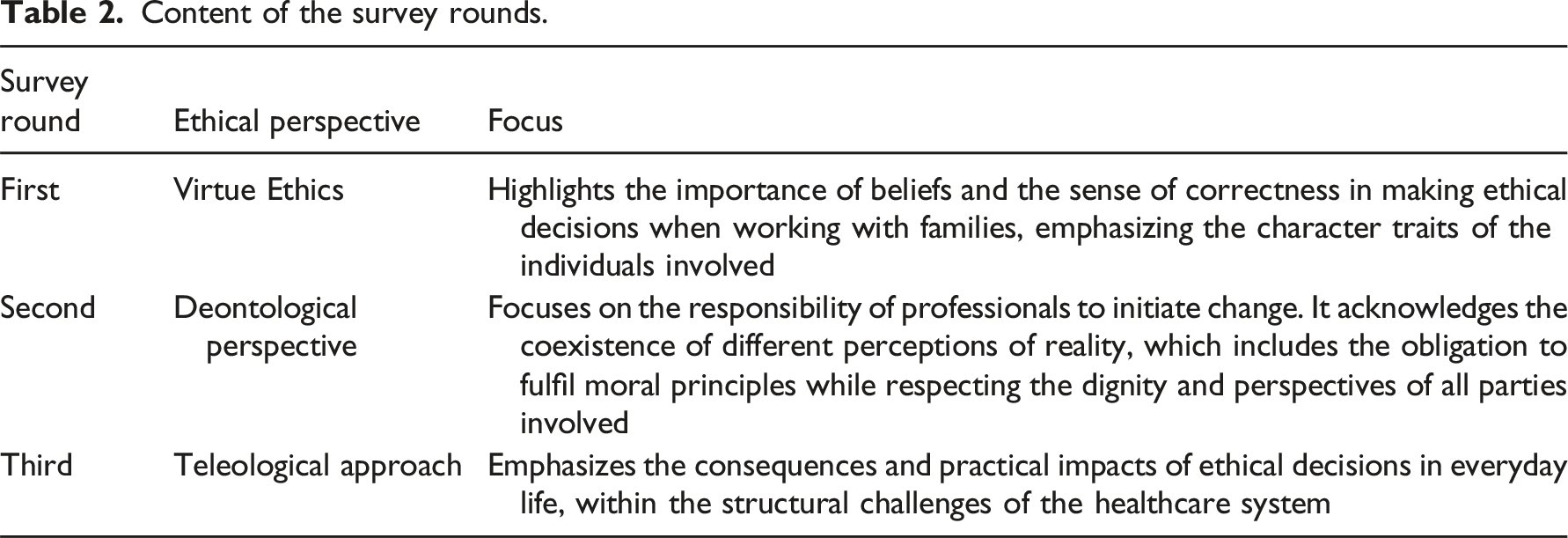
The expert panel (see Table 1) held six 3-hour meetings, starting with the introduction to a specific area of ethics followed by presentations of Delphi group responses. The participants of the expert panel then considered their own experiences from practical work with families in terms of this area of ethics. The introductions to ethical theory were drawn from Dietmar Hübner’s Introduction to Philosophical Ethics, 18 which provides a clear framework for key ethical concepts and debates. Additional sources included Düwell’s Handbook of Ethics, 19 Riedel’s Ethics in Healthcare, 20 Conradi and Vosman’s Practice of Attentiveness, 21 and various articles from the Stanford Encyclopedia of Philosophy. 22 Additionally, to establish a connection with FSC, each session included the discussion of appropriate material from the Illness Beliefs Model (IBM), 7 which was then linked to the ethical concepts. In a concluding focus group interview with all participants, which also lasted 90 minutes, the results were presented for a member check, in which the collected data were critically reviewed, discussed, and further refined. The aim of this study was not to assess the theories for coherence and consistency but rather to explore their relevance to FSC and to gain inspiration from them. Participants concentrated on the elements that were meaningful to them and relevant to their daily work.23–25 Data analysis was conducted based on the QUAGOL method 26 ; however, the team approach was omitted due to resource constraints.
Ethical considerations
The research project was conducted in accordance with the ethical principles of participants’ informed consent and the Declaration of Helsinki. According to the Cantonal Ethics Committee (KEK) of the Canton of Zurich, this study does not fall under Swiss legislation regarding human research, as confirmed by the Cantonal Ethics Committee on the December 14, 2021 (waiver no. Req-2021-01424). No participants were at risk of harm by participating and all signed an informed consent form prior to enrolment in the study. The data were collected in accordance with the ethical principles of informed consent, confidentiality, and the participants’ right to withdraw at any time without giving reasons. There were no conflicts of interest.
Findings
Family Systems Care (FSC) engages with metaethics, particularly through cognitivism and constructivism, to form its ethical foundation for moral guidance. 6 In FSC, cognitivism holds that moral values are not subjective or relative but emerge from biological and biographical factors, suggesting an objective moral truth, though not readily apparent. 1 6,9 Constructivism, aligned with pragmatism and communication theories, argues that moral norms are created, not discovered, based on biological structures. It emphasizes that our perceptions of reality are socially constructed, influenced by individual and social processes. 18 This view opposes a purely scientific approach, promoting a pluralistic understanding of ethics that considers relational dynamics and contextual factors, rather than focussing solely on objective truth. Social constructivism, rooted in 1980s psychology, further underscores that knowledge. Ethical norms are shaped by social and cultural contexts. 6 In FSC, this relational focus shifts attention from isolated individuals to the interactions and relationships within families, suggesting that ethical decision-making is a product of ongoing, dynamic exchange. This constructivist perspective helps to inform healthcare professionals’ (HCPs) engagement with families, allowing for more flexible and responsive care that integrates both scientific knowledge and individual perspectives.
In ethically challenging situations, HCPs in FSC identified three main concerns: recognizing ethical dilemmas, applying ethical reasoning, and implementing decisions in practice. The most challenging ethical aspects in day-to-day practice is having to implement ethical decisions without being involved in the decision-making process, managing difficult communication, and navigating contextual limitations that contradict personal beliefs. Participants reported using three approaches to address these dilemmas: a pragmatic-intuitive response, an emotional approach, and a cognitive performance of ethical discourse. While emotional and intuitive responses often stem from lived experience, ethical theories helped HCPs articulate their thoughts and better communicate their concerns. Furthermore, participants emphasized that ethical awareness should be present in all interactions with families, not just in ethically challenging moments. Ethical engagement requires empathy, presence, and an open attitude, while a balance between emotional and cognitive approaches is crucial. In resource-constrained environments, HCPs often face conflicts between professional beliefs and practical limitations, as seen in cases like late-term abortions and patients' requests for suicide. Although ethical theory helped express intuitions more clearly, participants stressed the importance of an empathic and respectful attitude in everyday family interactions. This combination of intuitive, emotional, and cognitive strategies helps navigate the complexity of real-world ethical dilemmas.
During data collection, it became clear which ethical theories were most relevant to HCPs in their clinical work with families. This section outlines the areas of virtue ethics, deontology, and teleology in relation to the practical experiences of participants, as these three proved central to the discussion of morally informed decision-making. Further topics that emerged from the participants’ experience within FSC in relation to ethical thought are dealt with in a companion paper.
Virtue ethics
Virtue ethics originated in antiquity and is the oldest moral philosophical approach in Western philosophy. A virtue is a fixed disposition of character that enables human beings to perform the right action under appropriate circumstances.
18
Perspectives on virtue introduced to the expert panel included those of Plato, Aristotle, Thomas Aquinas, and more modern philosophers such as Alasdair MacIntyre and Martha Nussbaum. The expert panel explored several virtues based on the theoretical introduction and deduced which they consider significant in therapeutic conversations with families. As illustrated in Figure 1, the participants singled out classical virtues such as faith (fides), fortitude (fortitudo), hope (spes), and ‘caritas’ in discussion. The values of respect and appreciation – often expressed through commendations in the FSC – were also emphasized, with participants perceiving them almost as virtues. The virtues patience, as well as prudence (prudentia) and temperance (temperancia) referred to as humbleness (humilitas) in FSC. All these virtues were perceived by participants and seen to have the potential to assist individuals and families in transcending suffering, guiding them from the ‘Golden Mean’ towards Plato’s ideal of soul harmony,18 as they discover new paths for coping and healing. Practical relevant aspects of virtue ethics (Source: Created by the author).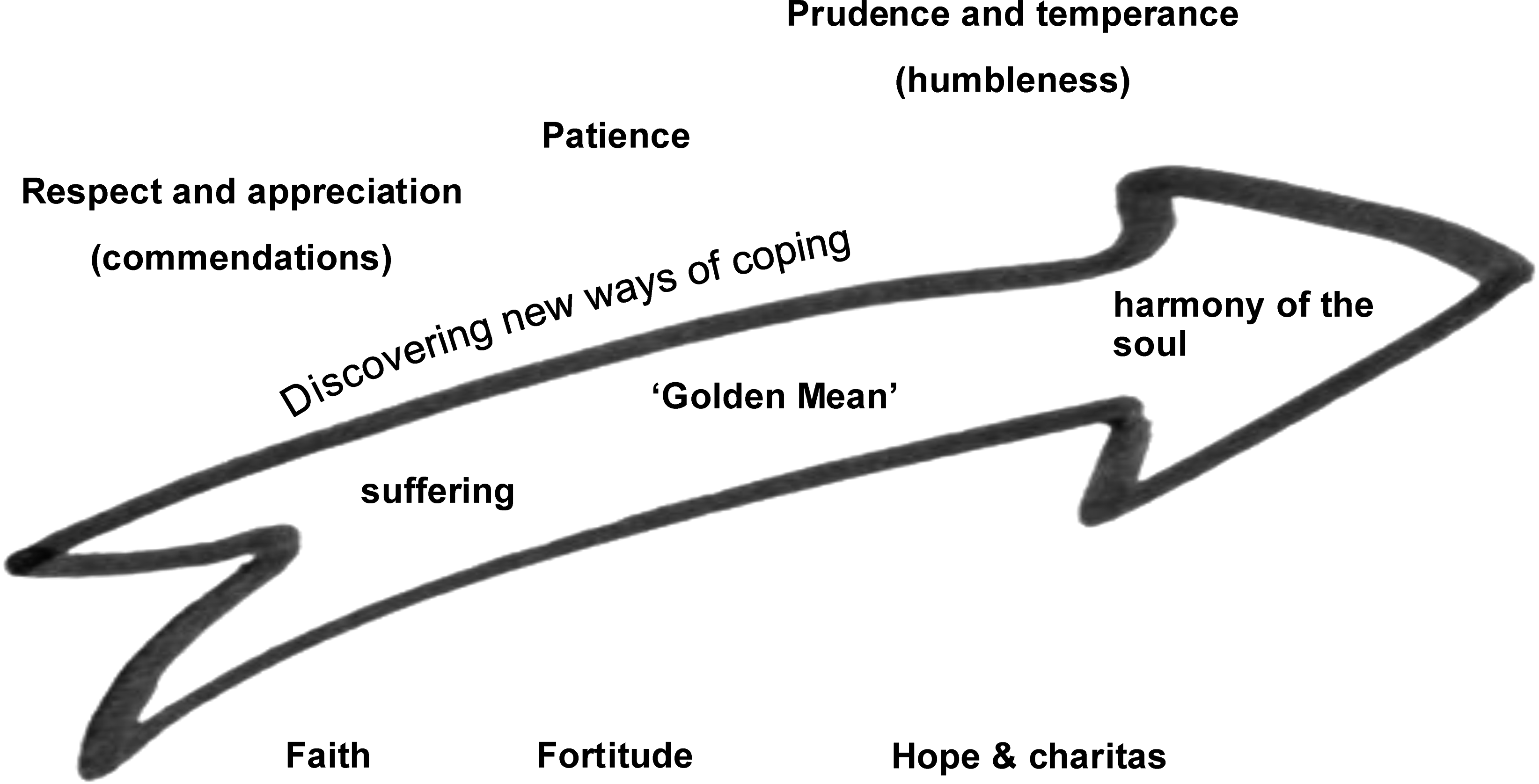
Aristotle describes each virtue as existing on a continuous scale between lack and excess. The search for a balance between two extremes was evident through all the participants’ discussions, just as Aristotle stipulates a ‘Golden Mean’ as desirable in the exercise of every virtue. The ‘Golden Mean’ emphasizes moderation and balance in ethical behaviour. For example, ‘honesty’ (alētheia) is a virtue. The exaggeration of ‘being honest’, positively intended, can be experienced in its effect as a negative ‘hurtful’ behaviour. Doing the right thing, according to Aristotle, therefore means finding the middle way between exaggeration and deficiency. Aristotle says that the virtue of ‘wisdom’ (sophia) allows people to find this ‘Golden Mean’. People learn to do this through experience, reflection, and analysis. Through habituation, repeated practice, a transition takes place from the mind-virtue ‘wisdom’ to the more lived character virtues. Habituation can also go wrong and result in an undesirable tendency towards one extreme. 18 The expert consultation can itself be taken as an example of the process of experience, reflection, and analysis, as we sought to learn from the knowledge and experience of the participants.
In the expert panel, participants entertained a long discussion on how best to apply virtue ethics in FSC. They concluded that this pertains on two levels: on the one hand as the virtues of the HCPs in their practice, on the other hand as the potential strengths of the family. Furthermore, the participants concluded that, corresponding with Plato’s descriptions of ‘harmony of the soul’ as the goal of virtuous life, 18 the goal of FSC is always to strengthen the family and soften suffering, and one way to achieve this goal is by focussing on the virtues of the family.
Core virtues for Family System Care.
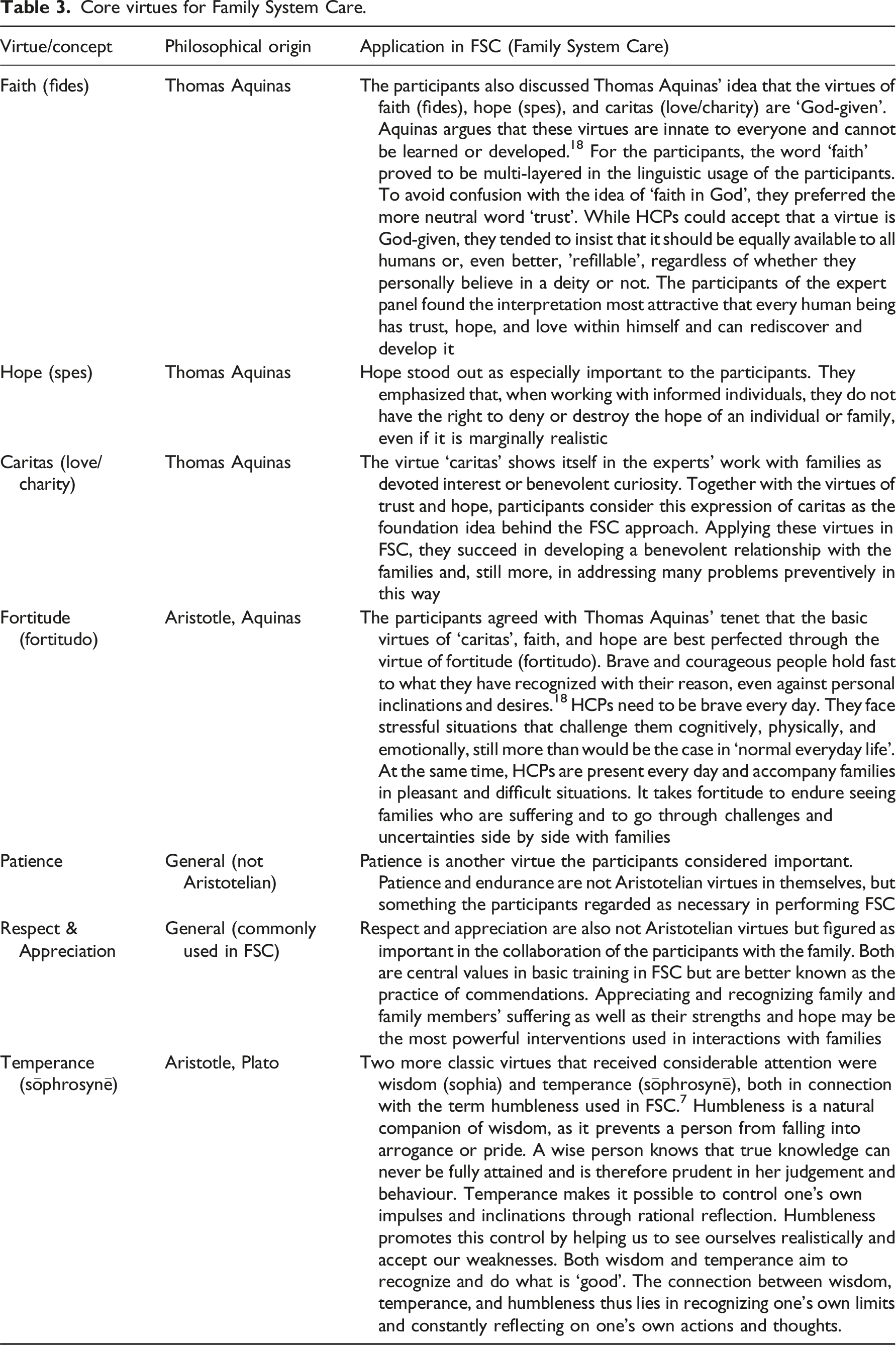
HCPs practicing FSC do not see themselves as omniscient experts on families. The participants found that humbleness protects them from unrealizable expectations of themselves. The stance of humbleness gives a framework for the responsibilities participants take in conversations with families. To them, humbelness to them means that they can provide a context for change, but do not hold power over change or the direction of change. This does not absolve them from the responsibility to perform at their best.
Interestingly, the ‘Tree of Virtues’ from the Speculum virginum of the 13th century already reflects the ‘Golden Mean’ and the fluid transition between virtues. 28 This depiction includes the same main virtues that our participants intuitively selected, except for justice (iustitia). Although justice plays a central role in various philosophical traditions – as a cardinal virtue in Plato and Thomas Aquinas, and a character virtue in Aristotle 18 – it was not addressed by the participants. This may be because they focused on virtues more directly relevant to interpersonal relationships and family support, or perhaps justice was perceived as too abstract, impersonal, or institutional for direct application in therapeutic conversations. It is also possible that the participants do not perceive justice as a virtue, but primarily as a normative value or an ideal worth striving for. Furthermore, in the depiction of the ‘Tree of Virtues’, humilitas (humility in this context also humbleness) is presented as the root of all virtues, a necessary foundation for all others, 29 aligning with the participants’ insights.
The results show that virtues as character traits are familiar to the participants. They use many different virtues to describe aspects of their FSC practice. They describe how virtues support them in finding the ‘Golden Mean’, in finding arguments in ethical discourse or decisions, and in choosing appropriate and helpful behaviours. Reflecting on virtues can help HCPs in their interaction with family members. Knowing the various forms in which virtues are manifest, participants can discover and elaborate on strengths and resources within a family. Healthcare professionals share the experience that in times of stress and suffering, families often lose access to their own strengths and thus ‘forget’ them. Reconnecting families to their strengths (or virtues) boosts their ability to act and make shared decisions.
Aspects of deontological theory
Deontology or the ethics of duty and commandments inspired participants to explore the intersection of FSC and Immanuel Kant’s categorical imperative. They found a clear link between the ethical obligations and core beliefs in FSC. What HCPs or families perceived as a duty was often closely aligned with their core beliefs. In the discussion, the concern focused on conflicting obligations that appear to apply at the same time. Moreover, participants identified a connection between the terms ‘duty’, ‘obligation’, and ‘belief’, observing numerous similarities between these concepts. However, the understanding of what constitutes beliefs does not fully align with the concept of duties, as will be further explained below.
Kant’s first formula of the categorical imperative corresponds to the principle of universalizability: ‘Act only according to that maxim whereby you can at the same time will that it should become a universal law’. 30 In other words, prior to acting, one must consider whether the action would be acceptable if all others acted the same way. In the context of Kant’s argument that moral actions must be based on universal principles, the statement ‘Lying is wrong’. was taken up by the participants. While they agreed with the statement, they also felt the need to qualify it, to add a but-clause as a way of mitigating the sweeping claims. When confronted with the example of hiding refugees from state persecution, for example, the duty to ‘protect life’ was generally considered more important than ‘not to lie’. For Kant, lying remains morally reprehensible even where it might produce an apparently positive outcome, because it violates the universal duty to be truthful. Moral duties are not relative or situation-dependent in his view, but absolute and universally valid. Thus, participants could not unreservedly agree with the ethics of duty, in which moral actions are judged as right or wrong, based on whether they are consistent with moral duties, rather than on their consequences. In contrast to Kant, the participants perceived duties and their hierarchical prioritization as not solely dictated by reason, but also as influenced by contextual factors and frequently intertwined with empirical requirements encountered in everyday life. Furthermore, the situational independence advocated by Kant is viewed in a fundamentally different way within FSC, as evident in the strong focus on contextualization.
As understood within FSC, ‘context’ encompasses the entirety of the situation as well as the background factors that are pertinent to a specific event or individual. 6 It also refers to context in conversations, creating an open space, for example, by consciously focussing on building authentic, compassionate relationships and getting to know the family in an inquisitive, respectful and non-judgemental way, which makes changes possible. 7 By creating this context, HCP can facilitate a shift in the personal perspective of the individual holding a specific belief. In one example from a therapeutic conversation, a mother expressed the belief, ‘I must not show my grief to my 13-year-old daughter so as not to burden her’. The mother wanted to protect her daughter, but thereby undermined the connection between them. After a few conversations, the mother’s understanding of the situation changed, and so did her behaviour. The goal of protecting her daughter remained prominent, as not to ‘let all the emotions rain down on her’. However, her priority became ‘being a good mother’, that is, her motivation shifted from a negatively charged to one that is positive and affirming. By exploring her core belief, the mother was able to give a different meaning to a challenging situation and thus to free herself from the worry of ‘overburdening her daughter’. In this way, participants may transition from a deontological perspective that emphasizes contextual independence to an attitude determined by the principles of virtue ethics. In this instance, the focus is on demonstrating how suffering can be alleviated through the modification of beliefs, thereby creating a context in which change is feasible.
While discussing Kant’s principle of universalizability, the participants discovered a similarity to relative autonomy. According to this principle, one’s own autonomy only extends so far as it does not restrict that of others. Relative autonomy, 31 that is, the ability of an individual to make decisions and carry out actions that are independent but are influenced or restricted by social, cultural, or situational conditions, emphasizes the interplay between personal freedom and contextual factors.
Furthermore, Kant’s assertion that there is a difference between the way individuals present themselves to the external world and their internal feelings 18 was also reflected in the participants’ statements that they use embodied reactions to recognize when they are approaching core beliefs. By paying close attention to embodied reactions such as facial expressions, gestures, and posture, they ensure that their interpretations are not solely influenced by verbal responses. In their opinion, personal behaviour must be chosen in such a way that it is also attributable to others, but it must not ‘be imposed on’ others. To avoid imposing their own maxims on others, participants expressed a conscious willingness to critically scrutinize their own convictions and sense of duty.
Kant’s second formula of the categorical imperative is: ‘Act in such a way that you treat humanity, whether in your own person or in the person of any other, always at the same time as an end, never merely as a means’. 30 All participants agree and are familiar with the prohibition of instrumentalization and recognize that human beings must never be merely a means to an end. This aspect was self-evident to the participants, and thus rarely addressed, reflecting the belief in FSC that demonstrating respect and appreciation for others is one of the most crucial interventions.
Aspects of teleological theory
In teleology, the focus is on the aim to be achieved. Utilitarianism is the best-known form of teleology. 18 Participants were familiar with utilitarianism and its goal to achieve the greatest possible benefit for the greatest possible number of people. 18 Tension remains in the participants’ discussions of the proper balance between benefit to the individual and benefit to the entire family, such that the well-being of the individual is not sacrificed to the happiness of all others. Nonetheless, the basic idea of selflessness and prioritizing the community appealed to the participants, which contrasts with the general emphasis on individualism in the western world.
The participants were introduced to the fundamentals of teleological ethics, followed by examples drawn from Hübner. 18 Surprisingly, the participants focused on statements from philosophers typically associated with teleological views; however, the examples they chose and their contributions were more closely aligned with virtue ethics.
An idea taken from an author typically associated with teleology that caught participants’ attention was Adam Smith’s ‘impartial spectator’. 18 According to Smith, the moral sense of most people corresponds to the attitude of an ‘attentive spectator’. This observer is characterized by the fact that he has compassion (sympathy) for others and can put himself in others’ shoes. According to Smith, however, compassion is not enough to make morally correct judgements. These also require the perspective of an ‘impartial spectator’, a kind of moral counsellor who helps people to judge their own actions and moral decisions and motivates them to make fairer, more just decisions by forcing them to look at actions from an impartial point of view. Smith assumes that we can all feel a certain sympathy for other people in the sense of compassion for the emotional reactions of others, but also stipulates that empathy alone is not enough to take a moral attitude. While empathy is valued as such, to take a moral attitude, it must be subordinated to a good dose of self-control. 18 A balance between benevolence and distance maximizes overall benefit. By initially focusing on benevolence, one acknowledges that the primary concern is the well-being of individuals, while maintaining a distance from those affected enables one to view them as a cohesive unit from the perspective of the ideal observer.
The participants derived two useful lessons from the impartial spectator. As a first lesson, the participants replaced the impartial, distanced attitude described by Smith with a ‘multi-partial’ perspective, as delineated by Wright and Bell. 7 This approach fosters a benevolently curious disposition towards all individuals involved simultaneously. Rather than adopting a neutral or impartial stance, it assumes a ‘multi-partial’ attitude, offering equal consideration to all parties. Another discussion centres on the opposition between closeness and distance. Participants describe their understanding of human beings as fundamentally social and relational beings, whereas among HCPs, there is a tradition of distancing oneself and of exercising self-control over all emotions or affections when working with patients. For the participants, this distanced, self-controlled attitude does not do justice to the complex realities of human encounters and runs the risk of indifference towards the other. They prefer to be professionally engaged with fellow human beings. Especially in the early years of a HCPs career, it is challenging to achieve a balance between dedicated and distanced behaviours and attitudes, reaching a form of professional involvement that is neither cold or disinterested nor overly burdened by feelings of responsibility for the patients. Here again, one observes the participants searching for the ideal balance, or Golden Mean, needed to be able to accompany family members with genuine professional commitment.
Strategies identified by the participants to balance distance and closeness with the family members include cooperation in expert teams, clinical reasoning, talking about their hypotheses and possible obstacles, and a clear understanding of their role and relationship in the family conversations. When participants distance themselves, they distance themselves from the outcome but never from the individual. The participants do this in continuous awareness that they do not have the power to effect change for the family on their own, but that they can create the context and the space for this to occur. This relieves the participants and enables them to patiently accompany families in difficult situations over a longer period. Figure 2 schematically illustrates the tensions between individual and collective well-being, the balance of closeness and distance, and the shift from impartiality to considering all involved parties, with the overarching aim of ensuring that families are supported by professionally engaged practitioners over the long term. One individual between others (Source: Created by the author).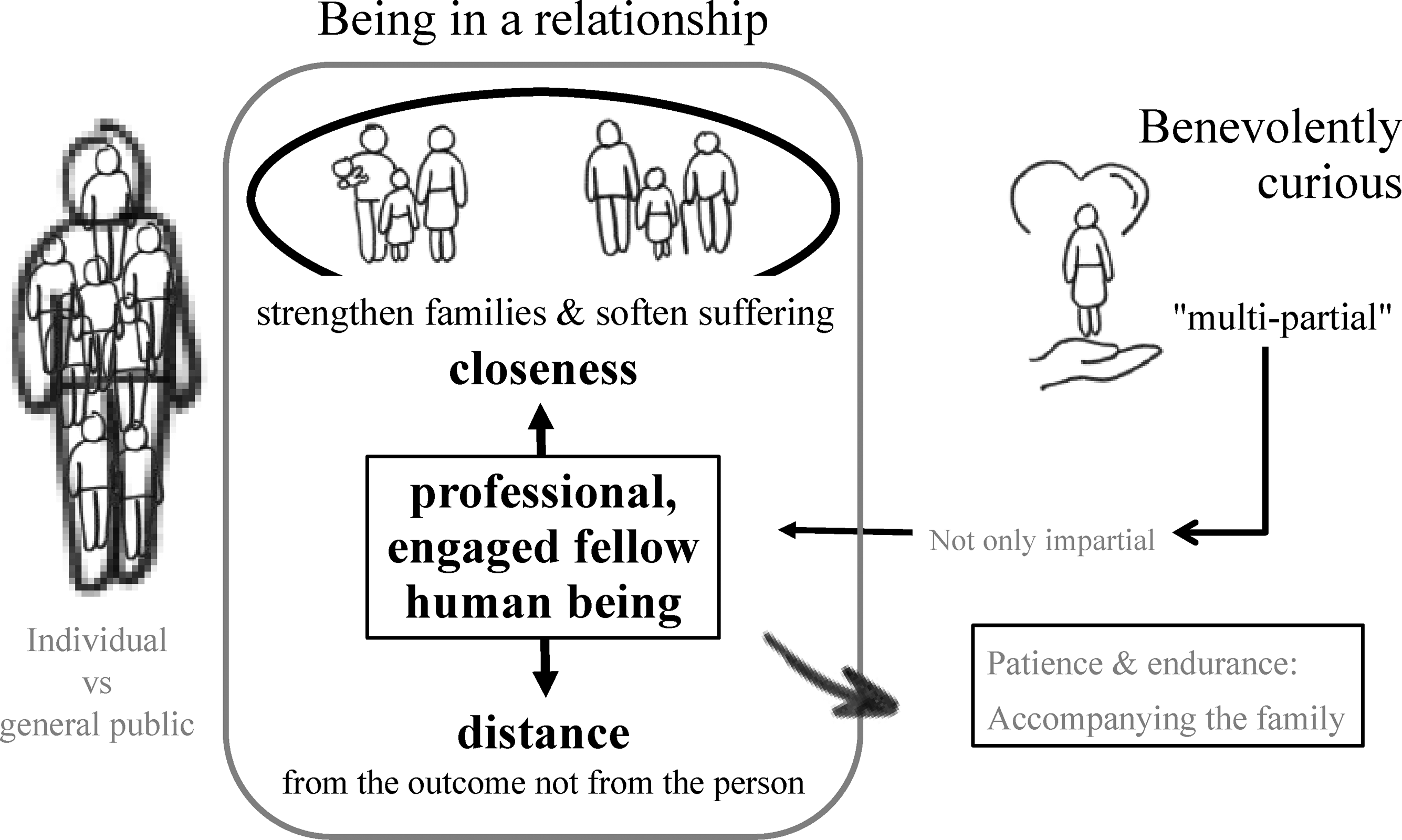
Conclusion
In the course of this study, it became evident that the practice within Family Systems Care (FSC) extends beyond the formal application of the Calgary models. Expert consensus emphasized the fundamental principles of attitude and behaviour as a guiding framework for communication. Nevertheless, the specific components of the Calgary Family Assessment Model (CFAM) and the Calgary Family Intervention Model (CFIM) remain integral to enriching systemic and multilateral family counselling. While no extensive empirical research explicitly addresses ethical reflection within CFAM or CFIM, existing studies32,33 indicate positive effects on nursing practice and implicitly considers ethical aspects.
For healthcare professionals (HCPs) engaged in FSC, ethical practice is aptly encapsulated in the words of Wright and Bell7,34: ‘To be a “particular kind of person” and a way of being in clinical practice are represented by a person who looks for strengths amid suffering, hope amid despair, and meaning amid confusion’ (page 303). This characterization illustrates that the attitudes and ethics underpinning FSC cannot be confined to a singular theoretical framework. Rather, they embody a relational dynamic within the HCP-family interaction, wherein the cultivation of ‘goodness’ facilitates the pursuit of equilibrium or ‘the middle’. HCPs endeavour to foster an environment that recognizes and nurtures strengths, promoting resilience and connection while facing challenges.
By offering an overview of ethical concepts and reflecting on expert consensus, we identified the contribution of virtue ethics, deontology, and teleology within FSC and deepened appreciation of their significance and reveal their utility.
Virtue ethics inform participants in creating a context of respect and appreciation, enabling them to stay present and in touch even when ethical challenges arise. Participants describe a trusting relationship as the most ethical way of working with families. This way of working likewise finds expression in the IBM. 7 Wright offers a formula that expresses the participants’ experience with virtues: ‘Kindness, compassion, and love are healing’, 35 corresponding to caritas and humility. While engaging with the examples provided from authors in the realms of deontology and teleology, the participants tended to discuss aspects more closely aligned with virtue ethics. It is possible that virtue ethics resonated more with them, as they may perceive it as more immediately applicable and adaptable to practical situations.
Closely related to virtues is the deontological approach, emphasizing recognizing human dignity and treating patients with moral care as a duty. While participants did not fully align with Kant’s ethics of duty, they found similarities between duties and beliefs. FSC imposes an obligation to value others, recognize perspectives, and respond appropriately. As Tuckett noted, 5 deontological theory does not clarify how an individual should act when faced with conflicting but equally binding obligations. He suggests that caregivers are guided by deontological principles, acting from a sense of duty and adhering to generally accepted rules. 5 The participants expanded on the idea, finding that, in the context of the FSC, duty may correspond to principles that encourage engaging with families in a non-judgemental manner, adopting a curious and benevolent attitude, and being aware of other people’s needs and perspectives in relation to relative autonomy.
Teleological perspectives were again characterized by virtue ethics. The balance between empathy and self-control is also thematized in Smith’s theory. Participants achieve this balance through a multi-participatory attitude. This approach fosters collaboration, focuses on families’ concerns, and removes obstacles in the relationship. 36 The goal of the FSC to empower families and alleviate suffering is achieved, in part, through a multilateral approach that engages with each individual with benevolent curiosity while also considering the well-being of the family as a whole. This aligns ethically with a utilitarian perspective. 18 Caregivers guided by utilitarian principles strive to maximize positive outcomes for the entire family while promoting individual well-being. 5
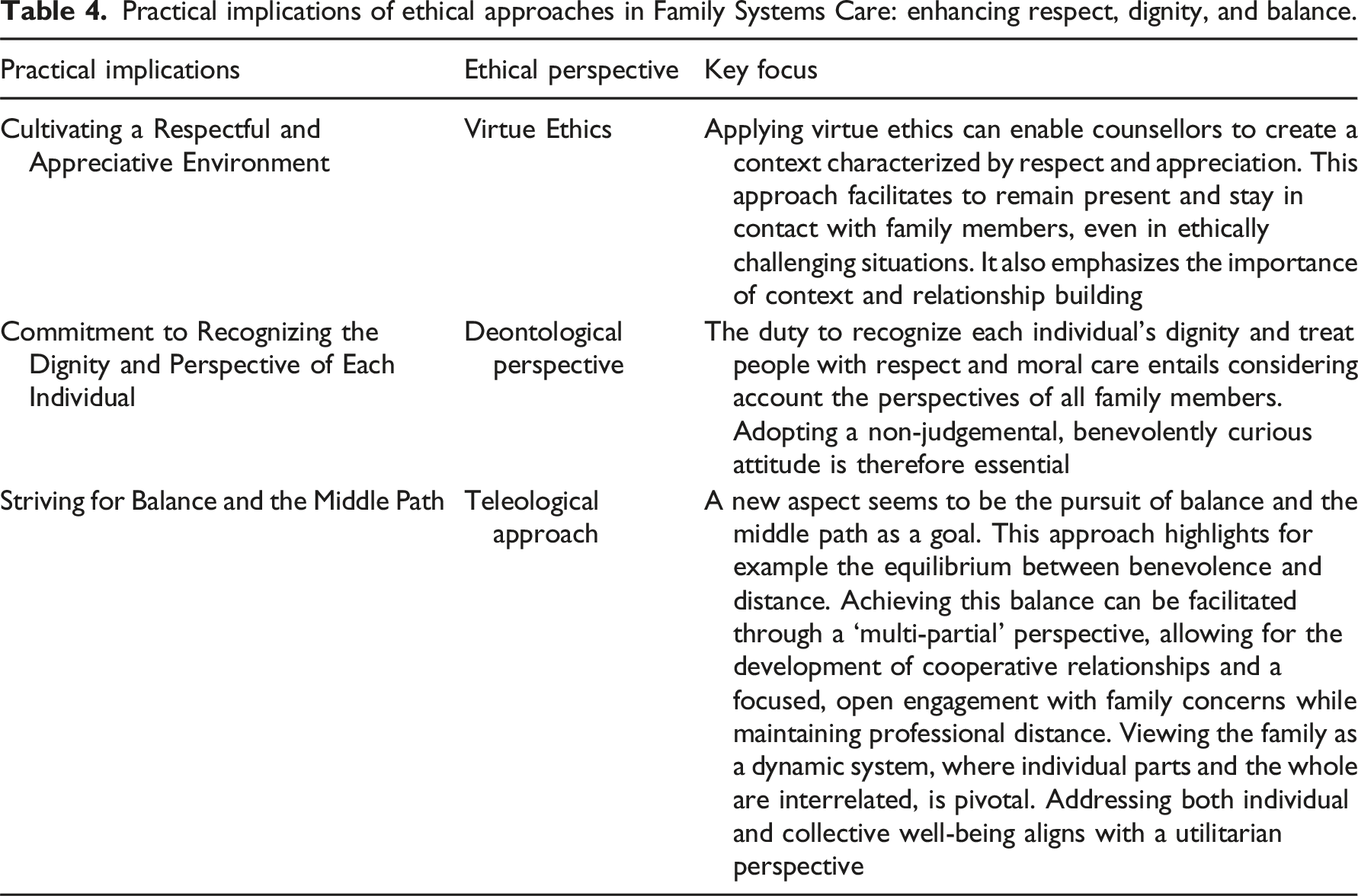
Practical implications of ethical approaches in Family Systems Care: enhancing respect, dignity, and balance.
Our participants were advanced with a clear ethical perspective. Since most HCPs apply FSC based on foundational training rather than advanced practice, findings may have limited applicability to family nursing. Another limitation is potential priming bias from presented content. Despite efforts to ensure clarity and coherence, presenting discussion material inherently introduces bias.
Overall, findings support the integration of ethical theory into clinical practice, as it can shift perspectives, beliefs, and attitudes, enabling HCPs to apply FSC principles more effectively and navigate challenging situations more successfully. The ‘Golden Mean’ must always be sought – whether between extremes (as with virtues), closeness and distance, different family members, or theory and practice. This interaction between beliefs, FSC and ethical theories occurs across all levels.
Footnotes
Note
Acknowledgements
The authors would like to thank all participants of the expert panel and Delphi group for their inspiring and active involvement in the development of this project. It was an honour to carry out this project with all these passionate and great people. We would also like to thank the Family Systems Care Unit at the Zurich University of Applied Sciences, for supporting this study by making staff time available for discussions and providing rooms. We would like to express our sincere gratitude to Dr Morgan Powell for his invaluable feedback and support during the editorial review process, which greatly enhanced the quality of this manuscript. We thank Barbara Preusse, lecturer and consultant in family nursing and family therapy, for her encouragement and inspiration. We thank Dr Tobias Zürcher, teacher of philosophy and researcher in medical ethics, for his support and feedback.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no specific financial support for the research, or authorship of this article from public, commercial, or not-for-profit funding agencies, the realization of the project was partially funded by ZHAW Zurich University of Applied Sciences.
Data Availability Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.