
Abstract
Family care—when partners, relatives, or other proxies care for each other in case of illness, disability, or frailty—is increasingly considered an important pillar for the sustainability of care systems. For many people, taking on a caring role is self-evident. Especially in a palliative care context, however, family care can be challenging. Witnessing caregivers’ challenges may prompt compassionate nurses to undertake actions to reduce burden by adjusting tasks or activities. Using a care ethical approach, this theoretical paper aims to provide nurses with an alternative perspective on caregiver burden and support. Drawing on the concepts of relationality and contextuality, we explain that family care often is not a well-demarcated or actively chosen task. Instead, it is a practice of responding to an all-encompassing “call” to care flowing from a relationship, within a social and cultural context where norms, motivations, and expectations shape people’s (sometimes limitless) care. We consider relational interdependence at the root of persisting in care provision. The question is then whether self-sacrifice is a problem that nurses should immediately solve. In ideal circumstances, self-sacrifice is the result of a conscious balancing act between values, but family care in the context of serious illness barely provides room for reflection. Yet, instant attempts to alleviate burden may overlook family caregivers’ values and the inherent moral ambiguities and/or ambivalent feelings within family care. Family care is complex and highly personal, as is finding an adequate balance in fulfilling one’s sometimes conflicting values, motivations, and social expectations. Therefore, we suggest that caregiver experiences should always be interpreted in an explorative dialogue, focused on what caring means to a particular family caregiver. Nurses do not have to liberate family caregivers from the situation but should support them in whatever overwhelms or drives them in standing-by their loved ones until the end.
Keywords
Introduction
Family care—when partners, relatives, or other proxies care for each other in case of illness, disability, or frailty—is increasingly considered an important pillar for the sustainability of care systems. Especially in a palliative care context, however, the role of a patient’s spouse or relatives is intensified. Family care can be challenging. The concept of burden, then, is well-known. Witnessing caregivers’ challenges may prompt compassionate nurses to undertake actions to reduce a family caregiver’s burden by adjusting tasks or activities. Although timely identification of burden is important, attempts to immediately relieve it may overlook a caregiver’s context and values.
Using a care ethical approach, this theoretical/philosophical paper aims to provide nurses with an alternative perspective on caregiver burden and support. First, to better understand why people persist, we will explain that family care often is not a well-demarcated and chosen activity but an ongoing response ensuing from a relationship. Secondly, we will elaborate on the ambiguities of self-sacrificial family care. Third, we point out that nurses’ support of family caregivers should not primarily be task-oriented but should be tailored to the personal meaning that family care may have for the involved partners or relatives. We also provide some practical suggestions for supporting family caregivers. The paper concludes with a short reflection.
Background
Fictive story of a family caregiver, derived from our research-based graphic novel.
Taking on a caring role for one’s relatives is often expected in current societies and self-evident for many family caregivers. 11 Our previous study, that included in-depth interviews with partners and adult children of patients receiving palliative care, showed caregivers’ persistent feeling of being called upon to care. 3 Looking at these caregivers’ stories from an ethical perspective, this being called upon does not seem based on a well-considered choice but presents itself as pre-reflexive. Caregivers often feel a strong urge to act and automatically do so, yet without having been able to thoroughly reflect on why or how. Some people report that they intuitively feel what is needed due to knowing the care receiver so well or having spent so much time together. And then they just do it.
At the same time, family care has its challenges. The multidimensional concept of “caregiver burden”5,12 is well-known within nursing, given the varied tools to screen for burden in practice.12,13 Our previous interview study, from which our story of daughter Eva was derived (Table 1), reported that family caregivers expect themselves to be attentive to the patient first while ignoring their own needs, available all the time, and assertive in managing the caring situation.
3
In another study, attentiveness, understood as being present and providing emotional support, was regarded to be the most important element in home-based palliative family care but was simultaneously disrupting caregivers’ daily lives.
14
Caring for a loved one can indeed be overwhelming and all-consuming,15,16: it impacts a caregiver’s whole personal realm - limiting living normal daily life
17
and social engagements,1,17,18 - while many caregivers feel unprepared for their caring role.
19
People, such as daughter Eva, feel limited—“chained” even—in their own lives,
17
as there is little time for their own families, social lives, hobbies, or work. In short, people tend to regard family care as something self-evident they wish or just have to do, sometimes at considerable personal and social costs. Image of daughter Eva (her story can be read in Table 1), one of the characters in the Dutch graphic novel Naasten about family care in a palliative care context. On this page, her father, who suffers from a severe lung condition and is gasping for air, asks her to stay in the middle of the night. “If that’s what you want”, she replies, “Sure.” ©Kranenburg M, Van Ooijen N and Haan MM. Naasten. Heverlee: Oogachtend, 2019. (permission was granted for the image)
As nurses spend much time with patients in palliative care settings, they usually are the first and main contact points for patients and their families.20,21 Compassion serves as the key motivator for many nurses in their work, stimulating them to turn passion into practice by actively trying to relieve suffering. 22 It is thus fully understandable that screening is advocated to detect burden at an early stage, especially given the challenges and unmet needs of family caregivers. 12 Although timely identification of burden is important, attempts to immediately relieve it may overlook a caregiver’s context and values. Assessing caregiver burden needs careful interpretation and consideration of the caregiver’s context.5,23 What drives people to provide family care, sometimes at considerable costs? To support sustainable caring relationships between caregivers and patients, we believe it to be important to recognize the complex interplay of underlying motivations for (not) providing family care, especially cultural and societal factors that shape why and how partners or relatives care for each other. 9 In the remainder of this paper, we will provide another perspective on family caregivers’ experiences and burden, by adopting a care ethical approach.
Family care as a response to feeling called within a relational and social context
Rather than viewing human beings as independent, utterly self-determining individuals that weigh alternatives and choose freely and deliberately—as the Western ideal of autonomy suggests—24,25 care ethicists view people as interdependent and morally motivated by the vulnerability of others.26,27 The concept of responsibility, understood as the task to respond to a need, is a corner stone of care ethical thinking: without people taking or accepting this responsibility, there is no care.25,28 Due to this mutual interdependence, relationality and contextuality are two additional key elements in care ethics. Care is a relational practice which cannot be understood in the abstract but should be considered in the lived experiences of the people that give and receive care within their relationships.27,29 These caring relationships are situated in a context in which power relations, norms, and expectations play a role. 29 Our previous interview study also highlighted a normative dimension of family care, 3 which was incorporated in the stories of our research-based graphic novel (Table 1). In this first section we will explain why family care, from the perspective of care ethics, is not a well-defined task people choose for and can simply withdraw from when it gets too burdensome.
Family care as a relational practice
Care ethics’ focus on relationality, first, helps us to understand the reality of family care, that is, how most partners or relatives just “find” themselves in the role of family caregiver, due to their specific relationship with the one who is ill. 25 They often accept this responsibility without weighing all possible personal consequences in advance and without actively choosing that role at a particular moment in time. 30 People seem to just do it. Daughter Eva (Table 1 and Figure 1) gradually stops-by more often, day or night, because her father needs her and “you just do that for each other.” Moreover, Barnes explains that it makes little sense to sharply distinguish the group of care receivers and care givers, especially in elderly spousal relationships. 29 It is hard to tell where care begins or ends, and, as roles often change, to depict who depends on whom. Family care can be framed as “dependency work”: a partner or family member is set free to do other things only if the dependency work of caring is taken over by others. 31 In that way, both the care receiver and family caregiver are dependent on each other.
In this relational interdependence, overburdening is a serious risk.12,14 As indicated in the introduction, family members sometimes persist in caring for their dying loved one at substantial costs, due to interference with their personal wishes, social activities, hobbies, or work.3,11,14 Eva (Table 1), for example, experiences increasing difficulties with focusing on her job while also managing her father’s household, care, and medication. Surrounding friends, family, or professionals may react with well-meant advice such as “don’t forget to think of yourself eh?!”, as the exhausting caring activities sometimes evoke surprise, awe, or worries by others. 3 “Thinking of themselves,” however, can be quite difficult for family caregivers. A care ethical perspective helps us to understand why. The crux is in the word “self,” which suggests that there is an autonomous “true self,” independent of the context of the caring relationship, which may be found by disconnecting from one’s relations. 31 Care-ethicists argue, in contrast, that the self should be understood as ultimately relational. 31 For family care this means that instead of having a terminally ill father, care is about being a grown-up child of a terminally ill father. 31 Family caregivers cannot abandon their relationships and quit being a child or partner altogether. Eva, as her father’s daughter, cannot avoid being called to care.
Of course, people may discard certain caring activities (e.g., bathing one’s parent) or take some time off to catch their breaths, thus in a way temporarily resist a call. Important to acknowledge, however, is that such actions would not erase the overall call to care, due to people’s ongoing alertness to the patient’s needs. Drawing on care ethics, we point-out that family care should not be reduced to a clear-defined task or action with a start and an end, resulting from a well-considered choice. 32 Rather, it is an ongoing (and often messy) process within a relationship, prompted by attentiveness to each other’s needs. 29
The importance of context in understanding how and why people feel called to care
Second, care ethics’ insistence that care is always situated in a specific context is also helpful in understanding family care, especially people’s sometimes immediate and self-nihilating responses to the felt calls. Eva, for example (Table 1), eventually quits her job and tends to neglect her relationship with her boyfriend. Our previous analysis of in-depth interviews with partners and adult children of patients receiving palliative care showed a sense of urgency in these family caregivers’ responses: the décor of deterioration in the palliative care context and the prospect of an approaching death urge people to act now, having only one chance to do so. 3 Furthermore, one’s capacity to care within one’s family is always affected by specific expectations, existing power relations, and the degree to which caring is valued and supported—not only in the relationship between caregiver and care receiver but also within one’s broader social, cultural, and political context. 29 Being the oldest daughter, for example, like Eva (Table 1), the darling sibling, or belonging to a family-oriented culture may lead to care expectations. 3 This implies, again, that living with or caring for a seriously-ill loved one often is not a matter of a straightforward, easy, or even explicit choice. 29 Rather, actual family care is highly dependent on the specific context in which partners and relatives have to navigate.
By whom and why do people feel called, then? A family caregiver feels connected to (and sometimes torn by) different domains on which they are expected to act. Our aforementioned analysis of interviews with family caregivers showed care may indeed start with being attentive to the patient’s explicit or implicit requests for help, but that well-intending and worried family and friends, one’s own convictions, and healthcare professionals entering normal life may also call upon a caregiver. 3 These calls, in turn, evoke caregiver responses. To better understand caregivers’ sometimes limitless responses, it is wise to have an eye for the underlying moral dimension of family care. Various studies, some across cultures and different health conditions, have shown the following generic and normative elements—or a combination of them—to be important drivers for people to provide family care, that is, out of love or affection, a sense of obligation or moral contract, reciprocity (e.g., retrospectively “paying back” to one’s parents), but also driven by the pre-existing relationship quality or by one’s family history, values (e.g., solidarity), and relational dynamics.3,11,14 Adding to this, we believe it is important for nurses to be aware that such motivations are not purely personal. Whether or not explicitly recognized by caregivers themselves, family care is deeply subject to social norms and expectations (e.g., “seeing one’s parents out,” emphasizing “till death do us part,” or regarding it a women’s responsibility)9,33 against the background of wider cultural values and beliefs (e.g., specific norms within one’s family or community, or spiritual and religious beliefs). 9
Ambiguity, ambivalence, and self-sacrifice in family care
Family care, thus, involves more than what meets the eye. A complex and normative layer always lies beneath one’s actions or emotions at the surface; and a sense of failure may arise when caregivers’ feelings or experiences conflict with what they believe is expected of a “good caregiver” in their particular social or cultural context. 33 To better understand family caregivers’ experiences, the concepts of ambiguity and ambivalence are of help. In this second section, we will explain that family care—as a phenomenon—is highly ambiguous, as it realizes certain goods or values while neglecting or suppressing others. That is why family care—as an activity—often leads to ambivalent feelings. We will further explain how burden and self-sacrifice are not necessarily problems that should be solved. In finding an adequate balance for family caregivers, the ambiguities and ambivalences surrounding family care should be openly acknowledged.
Ambiguity and ambivalence
The phenomenon of family care for someone close has been described as ambiguous: some things of value are realized while others are concurrently—inevitably but often unintentionally—oppressed or neglected. 30 Bereaved caregivers in our previous study were grateful for having persevered and having enjoyed precious “last things” with their loved one, spoke of an intensified and closer relationship, felt honored or proud for having been able to provide family care, but simultaneously reported challenges or exhaustion even. 3 It is often pointed out that the immense physical, emotional, or psychosocial challenges that family caregivers face while caring for their loved ones require support.34–37 Especially within intimate relationships and given its normative complexity, family care can be burdensome. Tragic situations may arise, due to competing demands stemming from one’s different roles: 11 people may feel torn between being a caregiver while also being a parent, employee, partner, or friend, and experience difficulties (or even exhaustion) in balancing the needs of the patient with one’s own. In responding to a sometimes 24-7 call, they have to deal with expectations from different sources, 3 as the relational self is connected to several contexts with diverse and sometimes even contrary interests and obligations. Rather than in feeling called per se, the burden of care might lie in the seeming limitlessness to which people feel called, that is, the self-sacrifice that lies in being constantly available and attentive to the patient’s needs first, 3 and the pressure on certain personal values this causes, like friendship, self-development, or parenthood. Adult children, or the “sandwich generation,” for example, may experience dilemmas in the responsibilities regarding both their parent and their nuclear family. 11
It may be hard for family caregivers to openly discuss their dilemmas, however. Next to ambiguity, the concept of ambivalence has been put forward as helpful in understanding the activity of family care, and particularly the associated caregiver dilemmas and suffering when people’s experiences do not precisely fit within the normative social expectations associated with their role as a family caregiver. 33 In exploring experiences across death and bereavement, it was shown that the messiness of their loved ones’ dying process meddled with family caregivers’ abilities to meet their initial expectations and desires regarding care. People then may feel regret or shame for not doing or feeling the “right” way, for example, not doing enough, or feeling hateful instead of loving towards the patient.
Solving the problem of burden?
Whether or not induced by social expectations, family care may lead to self-sacrificial behavior, in which people like Eva (Table 1 and Figure 1) put their personal lives—for example, their job, nuclear family, or social activities—in stand-by mode in favor of what is needed or demanded in the caring situation. 3 Excessive self-sacrifice would, simply put, be paradoxical as it would lead to a complete loss or even destruction of oneself which, in the end, even leads to not being able to care for one’s loved one anymore. 30 Supporting a family caregiver then means helping them to find a healthier balance, to prevent them from overstretching or “drowning” themselves and thus being unable to maintain caring, which would lead to less care for patients. Therefore, several tools—some validated and widely used—are advocated to quickly identify perceived caregiver burden,12,13,23 one of which related to a classification of caregivers in different risk profiles. 12
Such screenings and classifications fit well in current healthcare systems, in which evidence-based practice is promoted for early detection of problems and adequate treatment, and nursing skills like critical and analytical thinking, problem solving, and decision-making are deemed vital for efficient care.38,39 Concerns, however, have also been raised that this evidence-based paradigm disregards nurses’ tacit and relational knowledge in their patient encounters, as well as the patient’s and nurses’ preferences and values that are important for decision making. 39 In line with this critique, we suggest that caregivers’ preferences and values are essential to take into account to provide suitable family support. A more in-depth interpretation—which, for example, acknowledges the relational context—is needed when tools or questionnaires are used to identify (potential) burden or risks. Helping family caregivers to find balance is not a simple fix of activities and tasks. A narrowed focus purely on releasing people from their burden would bear the risk of paternalism and would not take into account the ambiguities and ambivalences of family care. Rather, following Gastmans’ thoughts on vulnerability and nursing care, 27 we believe nurses should provide care that enhances the dignity of both patients and their families. Caring for a family caregiver is not always about asking what is to be done (or which tasks have to be given up) but rather about how to preserve a person’s dignity as a whole. And thus, caring for family caregivers can be understood as responding to their vulnerability. Then, nurses’ support should involve paying attention to all dimensions in which people’s vulnerability affects them—which in the case of older adults would be on a physical, but also a psychological, relational, moral, sociocultural, or existential level.27,40
Helping family caregivers, thus, should take into account the trade-off and balancing of different values and expectations—stemming from the various dimensions of their vulnerability—that lie beneath all their caring duties and tasks. Nurses would do well to use their relational powers to enhance such a value clarification, that is, jointly with family caregivers weighing the various values, and acknowledging that contrasting values sometimes lead to dilemmas and tragic situations. Building on Gastmans’ work again, it is this dialogical process that should be shared between nurses and care receivers (in this case family caregivers), to find an appropriate answer to the question (and not necessarily the problem) of burden. 27 The third section of this paper provides some practical suggestions to engage in such a dialogue with family caregivers.
Another perspective on self-sacrificial care
Care can be depicted as a gift-sharing process, 14 especially self-sacrificial care is purely about “giving.” 30 Van Nistelrooij, however, shows us the multiple meanings of this concept (e.g., giving back, giving in, giving away, and giving up) and explains why self-sacrifice does not have to lead to problematic self-loss. 30 In her taxonomy of self-sacrifice, sliding from self-limitation to self-destruction, even the extremes are not necessarily problematic but may be viewed as acts that realize a value greater than the self. This is not to imply that family care should be advocated as some heroic act that realizes an ultimate good and thus is always acceptable. Van Nistelrooij warns to always be aware of the boundary between “proper” and “improper” forms of self-sacrifice. But how to pursue balance in family care? Van Nistelrooij defines self-sacrificial care as care provided “despite the acknowledgment by the self that one will not realize other goods (for instance, care for the self), and despite the acknowledgment that the good of this caring is not unambiguous or indisputable” (p. 286). 30 So, in ideal circumstances, self-sacrifice would be the result of a conscious balancing act. A certain amount of self-loss can thus be evaluated positively, if family caregivers consciously acknowledge that they will not realize other values (e.g., related to their own work, hobbies, family life, or personal goals) and also acknowledge that the intended value or their care is not beyond doubt but can be questioned by themselves or others.
Implications for nurses’ support
From a care ethical perspective, family care can be viewed as a practice flowing from a relationship within a specific cultural and social context, which has meaning for the people involved. Family care, thus, is no clear-defined task that can or should simply be taken-over in case of burden. Although caring is an integral part of being human, the concrete realization of family care is highly personal, as is finding an adequate balance in fulfilling all motivations and expectations. Next to positive interpretations (giving satisfaction, a sense of purpose or fulfilment, enabling personal growth, etc.), 11 family care can also have a negative, neutral, or—often—ambiguous or ambivalent meaning. Daughter Eva (Table 1), for example, experiences ambiguities: she finds it simultaneously rewarding and exhausting to give up her values with regard to her job while fulfilling her duty as oldest and darling daughter. She also narrates how they haven’t been very close, as her father always scared people away by not being friendly. Caring may thus be hard on her, possibly leading to ambivalent feelings deemed as “inappropriate” (such as anticipating relief in her father’s death). To prevent family caregivers like Eva from social misrecognition and alienation, we should recognize the complexities of family care in all its meanings. 33
Supporting family caregivers is about meaning rather than solutions
As we regard consciously finding a balance between contrasting values to be important, we suggest that family caregivers should be enabled to explore and act upon what caring means to them. For nurses and other healthcare professionals, this implies they should regard family caregivers as people within certain relational and social contexts that shape their care and evoke certain behavior. Previous reviews showed the complexity of palliative care nurses’ role,20,21 for example, being available, coordinating care, facing clinical challenges in a high workload, while also experiencing the personal impact and helplessness when working with patients in the end stage of serious illness. Dealing with families—for example, with them being demanding or vulnerable—can specifically be a source of stress for nurses. 21 Grasping the complex interplay of underlying values, family histories and wider social contexts may help nurses in understanding family members and why or how they care.
Furthermore, instant attempts to solve the “problem” of actual burden by changing people’s activities may overlook the inevitable ambiguity in family care, possibly depriving partners and relatives of a potentially self-affirming practice of family care. Moreover, even if burdensome tasks are relieved by practical solutions, family caregivers may still feel called upon: the tragic choices and their consequences still remain. Nurses should therefore not focus on liberating caregivers from the situation but support them in whatever overwhelms them when providing family care in their specific context.
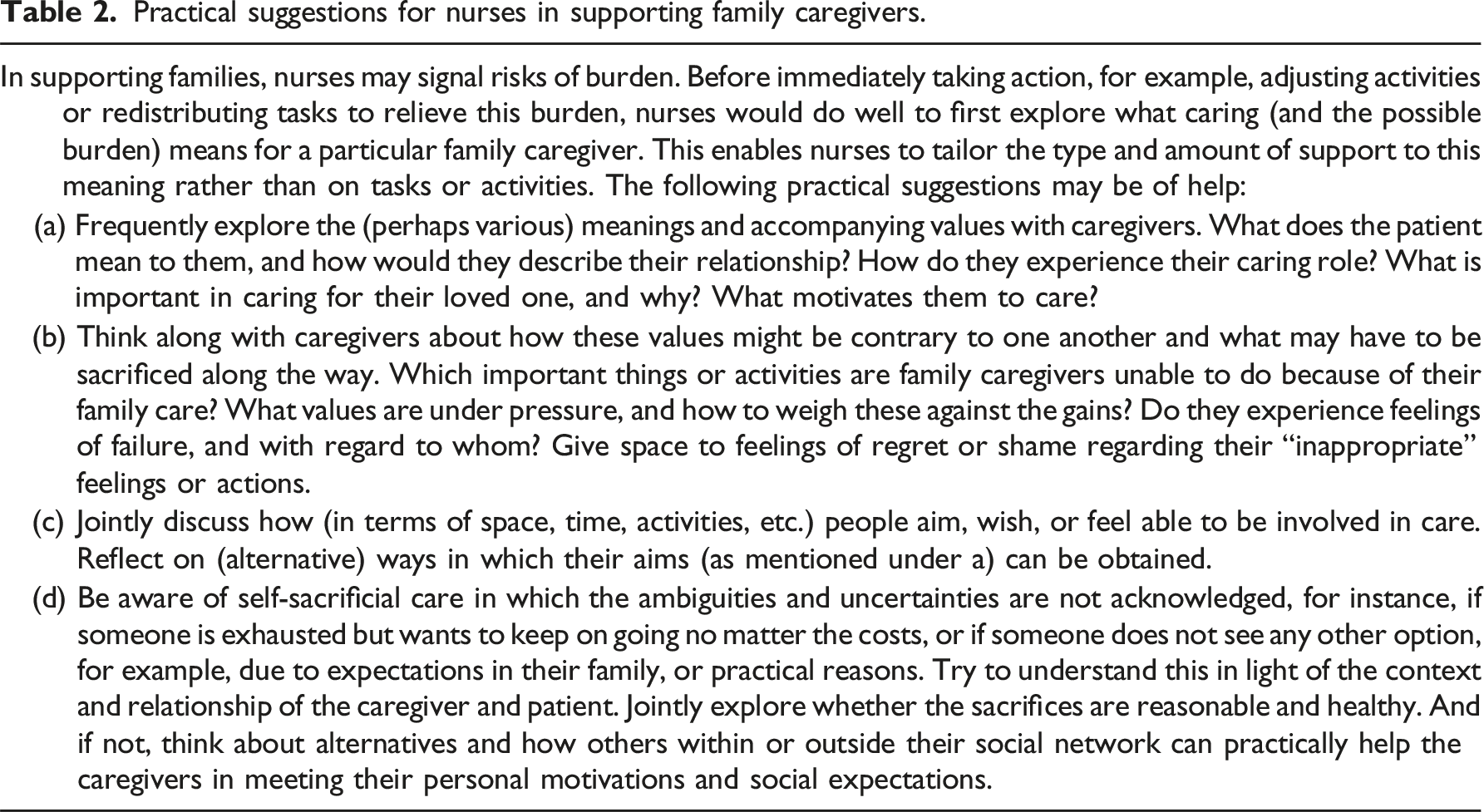
Practical suggestions for nurses in supporting family caregivers.
Reflection
The suggestions put forward in this paper come with challenges. First, emphasizing the importance of consciously finding a balance between fulfilling all expectations may seem to suggest that it is acceptable when people exhaust themselves as long as this is knowingly done. We want to add that pure exhaustion—even after weighing it in light of other values—may be a signal of excessive and thus improper self-sacrifice. 30 Then, caregivers are no longer capable of noticing that the “good” of their care is not beyond doubt—all their other roles or activities are put on hold in favor of the goods for the patient, without any space to think about alternatives. Thus, their care would be self-destructive hence disputable. Without doubt, thus, caregiver burnout is a serious risk, prompting authors to advocate support, time-off, and respite care.9,14
Furthermore, especially within a palliative care context of intensified care and an approaching death and grief, current caregivers as well as nurses may have neither the energy nor the capacity to thoroughly reflect on motivations or social expectations. We suggest, if possible, to cooperate with other disciplines such as social workers. Putting such deeper layers into words may, however, not be possible or helpful for everyone: due to all ambiguities and ambivalences, people cannot always voice their opinions and preferences, nor are they fully aware of the meaning or consequences of those. 27 We are aware that our suggestions to help caregivers reflect on meaning and weigh their sacrifices even bears the risk of increasing their burden, as issues become more explicit. Therefore, caution and moderation are required. As is common in advance care planning, we would recommend nurses to invest time in the beginning of a palliative trajectory to explore the family caregiver’s personal situation and ties, together with this caregiver (as suggested in Table 2). This may give nurses an indication of the family caregiver’s social network, familial relationships, and wider social or religious community, and any potential burdening expectations or helpful resources that may spring from them.
Lastly, familial relationships can be very complex and tensed—and some relatives may not be willing to undertake caring activities or may just be absent or hardly involved. Eva’s siblings (Table 1), for example, feel that their dad should be admitted to a caring institution as caring is asking too much of them, whereas Eva wishes to persist in caring for him. From a care ethical perspective, a choice to not become a hands-on family caregiver (e.g., to arrange healthcare professionals to help one’s partner shower, or to transfer one’s mother to an institution) can still be understood as “caring” or even “good care” when seen in the particular contexts of the individuals involved and their relationship. 29 Again, such a decision is not an utterly individual and free choice at a specific moment in time. It is important to understand all choices in the light of the dynamics of the relationship, within the larger context. Whether any decision is “good,” reasonable, or healthy should, in our belief, be discussed jointly with the caregiver. Care ethics offer space for choice. Taking responsibility—crucial for care to even exist—is a moral task after all 25 : people have the freedom to respond to or resist being called upon.
Summary and conclusion
This paper aimed to provide a care-ethically inspired perspective on family caregiver burden and support in a palliative care context. We explained that family care should not be reduced to clear-defined or well-chosen tasks or activities that can or should simply be taken-over in case of burden. Rather, caring for one’s partner, parent, or other proxy is an ongoing and often messy relational practice, due to being related and therefore called upon, in a particular context. Social or cultural norms and expectations shape how family care both is provided and experienced. We believe caregiver burden may specifically lie in the limitlessness to which people feel called, that is, the self-sacrifice that lies in being constantly available and attentive to the patient’s needs first, and the pressure on certain personal values or other roles this causes (e.g., caring while also being a parent, partner, employee, and friend). Family care, thus, is complex and highly personal, as is finding an adequate balance in fulfilling all of one’s motivations and expectations.
We conclude that nurses would do well to first explore the meaning of family care for a specific person, whether positive, negative, or—often—ambiguous or ambivalent, before immediate action is undertaken to relieve burden by adjusting or redistributing tasks to others. If possible, caregiver experiences—and specifically signals of burden or the results from screening tools—should be interpreted in an explorative dialogue with the family caregivers themselves (Table 2). Such a dialogue should keep into perspective the specific caring relationship between the involved people, the person’s social context, and how to balance a person’s values and expectations that shape the impactful experience of caring for a dying loved one.
We are fully aware, however, that this paper describes an ideal, whereas the actual world of family caregivers and of nurses’ support may be tough and messy, especially in acute, brief, or intensive caring processes. Family caregivers may neither have time nor the capacity to thoroughly reflect on what caring means for them. Notwithstanding, we suggest to carefully tailor support to what lies beneath burdensome experiences. Nurses, compassionate as they often are, do not have to strive to liberate family caregivers from the situation but should support them in whatever overwhelms or drives them in standing-by their loved ones until the end.
Footnotes
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MH declared that she is the coauthor of the graphic novel to which this paper refers. The other authors declared no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Netherlands Organisation for Health Research and Development (ZonMw, dossier number: 844001310).