
Abstract
Introduction
During a working day nurses may encounter situations compelling them to increase peoples’ autonomy and healthcare access, streamline healthcare, mobilise resources, influence policy and change systems. These activities, which are inherently political, could be labelled advocacy or activism.1,2 In undertaking these activities nurses are guided by or should comply with professional regulations. In 2024 we undertook a review of 217 medical and nursing codes of ethics, using natural language processing, to compare disciplinary and temporospatial differences and understanding how advocacy and activism may be promoted or constrained. 3 We found that though nursing codes of ethics referred to advocacy more frequently than medical codes, explicit reference to advocacy and activism was infrequent across all codes.
In this paper we take a closer look at Australian, British, and American nursing regulatory documents to explore what they say about advocacy and activism, either explicitly or implicitly. We also examine the documents more broadly to explore how they shape advocacy and activism. For context we first briefly address semantics and provide a brief overview of nursing advocacy and activism as well as the role and importance of nursing regulatory documents such as codes and standards. Next, we present the study findings, followed by a scholarly discussion of the issues that emerged from the data. While set in the global north this article has international significance as the nursing profession turns its attention towards addressing the health impacts of contemporary social, economic and environmental pressures; issues which require advocacy and activist interventions.
Advocacy and activism are dynamic terms and often used interchangeably. However, they represent a spectrum of political action; essentially, advocacy influences while activism overhauls, each with the aim of achieving political or social change. 4 Tactically, advocacy’s approach is usually diplomacy; gaining support for ideas and amplifying the voices of people drawing attention to their own issues. Activism’s approach is often, but not always, confrontational, disruptive and subversive, 5 taking more radical action to challenge ideas and working outside of the system to enact change. 4 Due to these differences, advocacy is usually associated with professionally acceptable behaviour and poses few negative consequences to the advocate, whereas activism is more often associated with abject behaviour and has greater consequences. Though this is context dependent with some acts of advocacy, such as internal whistleblowing, attracting severe consequences, 6 and some acts of activism, such as healthcare workers speaking out during the pandemic, 7 attracting great support.
To those of us who have studied the history of nursing, there is no question that nurses have always been politically active. However, the extent to which this is a legitimate part of our roles has only been considered relatively recently. Advocacy was first proposed as a key nursing role in the 1970s and was swiftly adopted by professional nursing organisations and nursing schools. 8 This assertion was grounded in an argument that due to their proximity to patients, as well as their position within the healthcare hierarchy, nurses were well positioned to empower patients and often better positioned to speak effectively on their behalf. 9 Definitions of nursing advocacy quickly proliferated, and in 1987 Webb consolidated them to the following key attributes: ensuring (i) patients had enough information to exercise autonomy, (ii) patients’ legal and moral rights were respected and (iii) health resources allowed appropriate quality and quantity of care. 10 Regulatory definitions of nursing advocacy have not ventured far from Webb’s conceptualisation. 11 However, beyond regulatory definitions, the broader literature indicates that nursing advocacy has additional attributes such as safeguarding patients, mediating between patients and others, responding to problems within health systems and championing social justice. 12
Nursing activism has been described as a conscious, robust effort within social and political spheres to challenge the status quo to achieve change at the level of health and social determinants.13,14 Unlike advocacy, regulatory bodies and wider profession’s acceptance of activism has been slow and somewhat reluctant. 13 However, proponents of nursing activism conceptualise it as part of the profession’s covenant with humanity, and a requisite to address health inequalities.13,15 Activism can include activities such as writing letters, raising public support, joining a professional organisation, creating coalitions, voting, lobbying and educating individuals and groups, testifying, networking with politicians, crafting policy and legislation and supporting like-minded nurses. 14 It can also include more radical and disruptive actions such as protests 16 and strike action. 17
Though nursing advocacy, and to a lesser extent activism, may be so common as to be routine, these activities present unique challenges which are often far outside the experiences of most lay people. Regulatory documents, therefore, such as codes of conduct and ethics and professional standards, may not only provide direction on how nurses should act in these situations but assist nursing educators to prepare the emerging workforce for advocacy and activism. Regulatory documents are generally created by professional regulatory bodies or groups and have many functions in healthcare. They are commonly created during the professionalisation process of an occupation group to create a group identity and delineate the boundaries of the profession18,19 or after a scandal, to reinstate public confidence. 18 Codes of ethics can also operate as decision-making tools, acting as a practice standard with professional and legal ramifications, developing a group identity and providing legitimacy to individual healthcare professions, 19 delineating professional responsibility 19 and directing and standardising healthcare education. However, healthcare professionals’ views of the effectiveness of codes in directing and supporting their practice is varied with some believing they play a crucial role or encourage professional conduct and others believing they are irrelevant or antithetical to professional conduct. 18
Nonetheless, as extensions of regulatory bodies, regulatory documents may offer key insights into how advocacy and activism are framed and shaped by professional organisations, in this case the Nursing and Midwifery Board of Australia (NMBA), UK Nursing and Midwifery Council (NMC) and American Nursing Association (ANA).
Methods
Research aim
In this study we sought to explore what regulatory documents said about advocacy and activism, either explicitly or implicitly. Secondarily we sought to examine the documents more broadly to explore how they shape advocacy and activism.
Study design
We chose a Reflexive Qualitative Document Analysis approach, with a critical feminist lens to analyse contemporary nursing regulatory documents from Australia, the UK and USA. Reflexive QDA is an iterative approach whereby the coding is not predetermined and changes reflect the researchers’ developing interpretation of the data. 20 Because we come to this research with experiences and scholarly knowledge of advocacy and activism and nursing, reflexive QDA allowed us to position ourselves inside of the research process, co-constructing meaning through our interpretation of the data.
Critical feminism is an approach within feminist theory that analyses and critiques the oppression of women together with intersecting systemic issues like class structure, race and sexuality 21 to reconceptualise hegemonic understandings of these concepts. 22 Like all feminist theory, critical feminism emphasises the importance of examining power relationships and making the political visible. 23 Critical feminism atuned us to gender oppression, broader systems of oppression and politics within the regulatory documents.
We followed Morgan’s approach to Reflexive QDA to identify and analyse the data 20. This includes (i) sampling, (ii) document selection and (iii) reflexive Thematic Analysis. Sampling
This study incorporated an interpretive element where the authors reflected on how regulatory documents applied to practice. As we did not presume to interpret documents beyond our own frames of reference, we selected nursing regulatory documents from countries in we worked (i.e. Australia, the UK and USA).
Document selection
Documents were eligible for analysis if they were: 1. Created or endorsed by the Nursing and Midwifery Board of Australia, the Nursing and Midwifery Council (UK) or the American Nurses Association. 2. Of a regulatory nature, providing nursing-specific rules and guidance. 3. Currently in use.
LM, SR, JDW identified current nursing regulatory documents from their respective countries. These were uploaded to the computer-assisted qualitative data analysis software, NVivo.
Reflexive thematic analysis
Consistent with Morgan’s 20 approach to Reflexive QDA, we used Thematic Analysis 24 to analyse the documents. This involves six steps. First, the team immersed themselves in the codes, familiarising themselves with the data and making notes about their thoughts about what is interesting, possibilities and connections (as they related to the research questions).
Second, we began systematically generating inductive codes about the data. We used the research questions as a starting point but did not have preconceived ideas about the final codes. RE, a bioethicist and non-nurse, performed semantic coding about the explicit meaning of the language of the regulatory documents. LM, SR and JDW performed both semantic and latent coding, which allowed us to focus on the implicit meaning of the documents. This step was undertaken individually.
Third, from our combined codes we then individually constructed preliminary themes, presented them to each other and selected the themes that told the best story about the data. We used thematic mapping in this step to show connections between the themes and subthemes.
We then revised (fourth) and defined (fifth) our themes to ensure each had a clear definition and boundary and central organising concept. Finally (sixth), as we wrote this publication, we tweaked our themes to ensure they remained grounded in the data and answered the research questions, and thought about them in the context of the broader literature.
Findings
Overview of documents
Document identification.
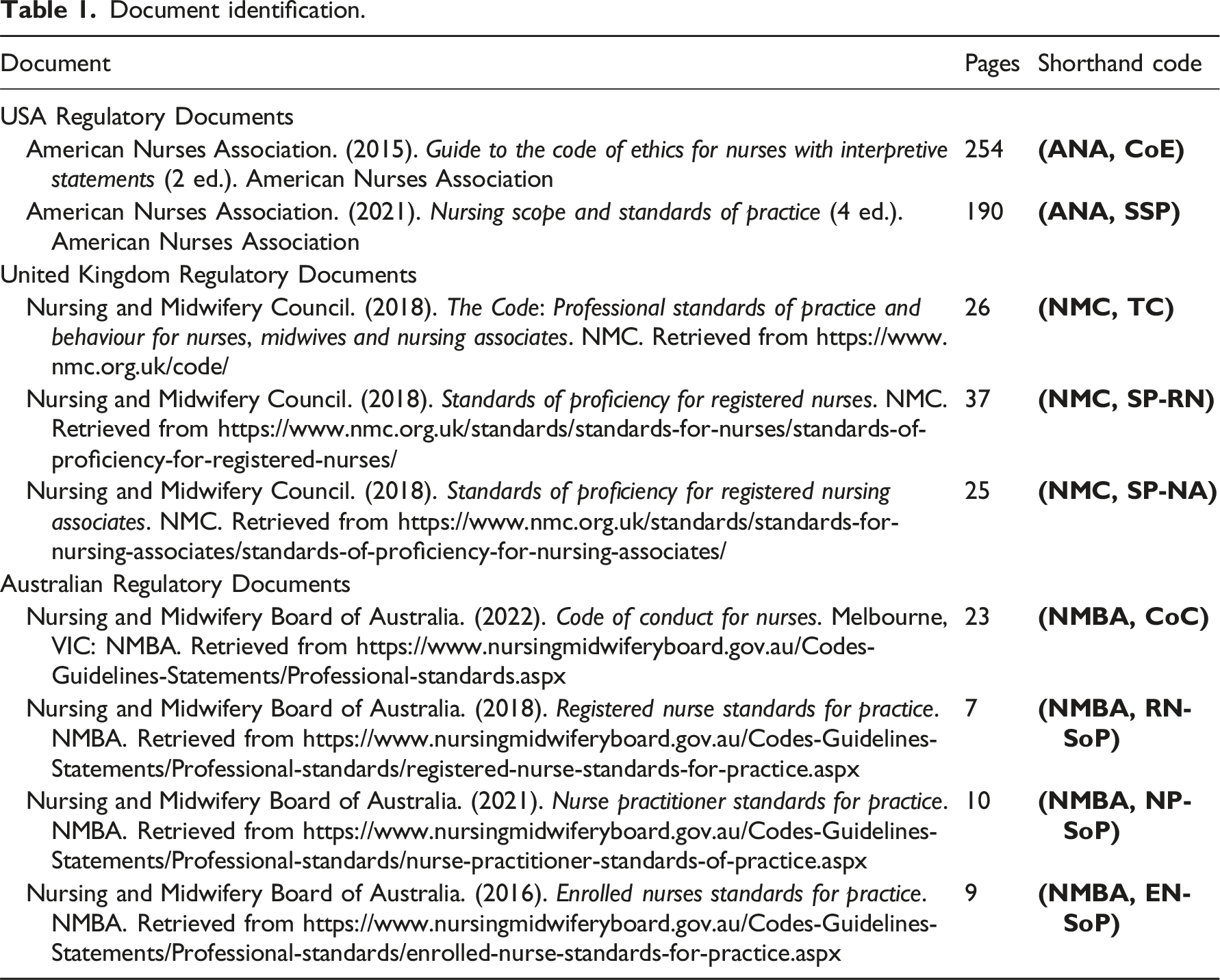
General description
Most of the regulatory documents refer directly to nursing advocacy, though the ANA provides the most comprehensive guidance. ANA’s reference to ‘advocacy’ or ‘advocate’ was noticeably more frequent (131 times - 26 references in the Code of Ethics and 105 in the Standards for Practice) than the Nursing and Midwifery Council (four times combined) and the NMBA (10 times combined). It is worth noting that the NMBA Enrolled Nurse Standards for Practice do not directly reference advocacy. Uniquely, the ANA Standards for Practice contains a specific advocacy section which lists and describes specific advocacy competencies for nurses and highlights that (t)he registered nurse demonstrates advocacy in all roles and settings.
Direct reference to activism is only referenced in the ANA Code of Ethics: The Guide emphasizes three functions of social ethics… c) social activism and reform that improves health promotion, illness prevention, care of the suffering, and equitable distribution, safety, and quality of health care.
While the direct references to ‘advocacy’ and ‘activism’ might be limited across the dataset, oblique references permeate the regulatory documents.
We constructed two major themes from the thematic analysis which reveal how nursing advocacy and activism is conceived and shaped in regulatory documents. Theme 1, Ideological arena describes the ideological influences (gendered and neoliberal subtexts) within the regulatory documents which influence advocacy and activism. Theme 2, A five-pointed star, describes the shape of advocacy and activism in the regulatory documents. The interrelatedness of these themes are conceptualised in Figure 1. Each theme will be explored individually using excerpts from the regulatory documents to illustrate the concepts. Conceptualisation of how advocacy and activism are shaped in the nursing regulatory documents.
Theme 1. Ideological arena
The regulatory documents contained both gendered and neoliberalist undertones which may depoliticise the role of the nurse and consequently, have implications for how advocacy and activism is shaped.
Theme 1.1 Gendered subtexts
On balance, the regulatory documents compel nurses towards agreeableness and civility. While there was some provision for confrontation, traditionally feminine traits such as kindness, respect and compassion (NMC, TC), integrity, honesty, respect and compassion (NMBA, CoC) and lovingkindness, harmony, authentic presence (ANA, SSP) were repeated throughout the documents and reinforced through statements related to civility and politeness: deal with differences of professional opinion with colleagues by discussion and informed debate, respecting their views and opinions and behaving in a professional way at all times (NMC, TC).
Consequently, references to advocacy or activism tended towards a language of mutuality and support and were more inclined to reference supportive and generative advocacy and activism, using verbs like ‘promote’, ‘uphold’ and ‘contribute’:
Promotes active engagement and the independence of people receiving care within the health care setting by involving them as active participants in care, where appropriate (NMBA, EN-SoP). However, there were three notable exceptions. The first concerns issues of safety, where more urgent and slightly antagonistic behaviours, like reporting notifiable conduct of health professionals, health workers and others (NMBA, RN-SoP), were called for. This was noted across all regulatory documents.
The second exception concerns discriminatory behaviour, where statements called nurses to challenge, discriminatory behaviour (NMC, SP-RN); this was also noted across most documents.
Theme 1.2 neoliberal subtexts
Neoliberalist undertones related to nurses’ individual responsibilities to look after themselves and their colleagues in stressful work environments were also noted. This includes the professional responsibility to adopt a healthy lifestyle (NMC, SP-RN), act to reduce the effect of fatigue and stress on their health, and on their ability to provide safe care (NMBA, CoC) and accept and manage uncertainty, and demonstrate an understanding of strategies that develop resilience in self and others (NMC, SP-RN). Interventions to assist nurses facing stress and burnout problematised the individual, not the system: Professional associations and healthcare systems are recognizing the relationship between resilience and burnout and are implementing evidence-based programmes to enhance nurse resiliency. Mindfulness is an example of this approach (ANA, SSP).
There are also statements in the regulatory documents regarding legal compliance that potentially deter the rise of nurses. Firstly, throughout the regulatory documents, nurses are cautioned to keep to the laws of the country (NMC, TC) in which they practise. Compliance with these statements appears to infiltrate the nurses personal and civic life as the regulatory documents call nurses to act professionally at all times (NMC, SP-RN): Nursing practice extends to any paid or unpaid role where the nurse uses their nursing skills and knowledge (NMBA, RN-SoP).
Moreover, the documents warn that unlawfulness could be construed as unprofessional conduct: not participate in unlawful behaviour and understand that unlawful behaviour may be viewed as unprofessional conduct or professional misconduct and have implications for their registration (NMBA, CoC).
A second deterrent placed on advocacy and activism is limitations placed on the expression of political beliefs. For example, the NMC remarks on the inappropriate expression of political belief in The Code, though does not define the term ‘inappropriate’: make sure you do not express your personal beliefs (including political, religious or moral beliefs) to people in an inappropriate way.
Theme 2. The 5-pointed star
All regulatory documents contained statements which directly or indirectly related to advocacy and to a lesser extent, activism. “The five-pointed star” is a theme that describes the shape that advocacy and activism take in these documents. The five points of the star are “for people”, “for inequality”, “for ourselves”, “for the profession”, “for systems change”.
Advocacy and activism for people
Advocacy and activism for people is a broad sub-category that relates to champion(ing) the voice of the healthcare consumer (ANA, SSP) and protecting those who are vulnerable within the healthcare system. We have chosen the word ‘people’ carefully as the regulatory documents explain that nursing care extends beyond care of individuals, it also includes individuals, their family and the community in which they reside (ANA, CoE): the words person or people include all the patients, clients, consumers, families, carers, groups and/or communities that are within the registered nurse scope and context of practice (NMBA, RN-SoP).
Advocacy and activism for people takes many forms. First, it relates to providing non-discriminatory, person-centred and sensitive care (NMC, SP-RN) which involves treating people as individuals and respecting ownership of their health information, rights and preferences while protecting their dignity and empowering choice (NMBA RN-SoP). This includes supporting and documenting a person’s right to accept or refuse care and treatment (NMC, TC).
Advocacy and activism for people in our care is also about incorporating safety measures into practice such as maintain (ing) communication with interprofessional team members and others to facilitate safe transitions and continuity in care delivery (ANA, SSP) as well as recognising the need to protect people and reporting the risk of potential for harm (NMBA EN-SoP) and focussing on the patient as the first allegiance of the nurse and on the primacy of the patient’s interests (ANA, CoE); in other words, maintaining professional boundaries.
Advocacy and activism for equity
Advocacy and activism for equity relates to improv(ing) care delivery and access for underserved and vulnerable populations (ANA, SSP) and respect(ing) and uphold(ing) people’s human rights (NMC, TC). It may include applying the principles of primary and public health, including health education, health promotion, disease prevention or taking health literacy into account (NMBA, CoC). It also involves understanding health disparities, unjust social structures and processes, and social and institutional inequalities (ANA, CoE) and addressing power imbalances caused by oppressive legacies such as colonisation and racism: This practice reflects particular understanding of impact of colonisation on the cultural, social and spiritual lives of Aboriginal and Torres Strait Islander peoples, which has contributed to significant health inequity in Australia (NMBA, RN-SoP).
It is also about adjusting healthcare delivery to meet the needs of people with disabilities as demonstrated in the following quote: facilitate equitable access to healthcare for people who are vulnerable or have a disability, demonstrate the ability to advocate on their behalf when required, and make necessary reasonable adjustments to the assessment, planning and delivery of their care (NMC, SoP-RN)
Advocacy and activism for inequality also has environmental and global health dimensions and includes advocating for the implementation of environmental health principles in communities in which they work and live (ANA, SSP).
Coalitioning and lobbying to address the social determinants of health (ANA, SSP) are key advocacy and activism interventions for inequality, though are only required at an advanced nursing level.
Advocacy and activism for ourselves
Advocacy and activism for ourselves is about the nurse ow(ing) the same duties to self as to others (ANA, CoE). It includes the responsibility promote their own health and wellbeing to remain fit for practice. This means acting to reduce the effect of fatigue and stress on their health, and on their ability to provide safe care (NMBA, CoC), recognising signs of vulnerability in themselves or their colleagues and the action required to minimise risks to health (NMC, SP-RN) and supporting colleagues who are encountering health or performance problems (NMC, SP-RN). It also means contributing to culturally safe work environment that is free of racism (NMBA, NP-SoP) and taking account of your own personal safety (NMC, TC).
Advocacy and activism for ourselves also means recognising our own limitations in practice and competence (NMBA, EN-SoP) and continuing personal and professional growth (ANA, CoE) such as using lifelong learning approach for continuing professional development of self and others (NMBA, RN-SoP) and advocating for systems that support…professional growth (NMBA, NP-SoP).
Advocacy and activism for ourselves can also include ensuring that the nurse and others they work alongside, remain within their scope of practice. It includes refraining from undertaking activities where competence has not been demonstrated and appropriate education, training and experience has not been undertaken (NMBA, EN-SoP) and relatedly, only delegate tasks and duties that are within the other person’s scope of competence, making sure that they fully understand your instructions (NMC, TC).
Advocacy and activism for the profession
Advocacy and activism for the profession means promoting the integral role of nursing practice and the profession in influencing better health outcomes for people (NMBA, RN-SoP). This has additional dimensions for advanced practice nurses such as informing the political arena about the role of nurses and the vital components necessary for nurses and nursing to provide optimal care (ANA, SSP) and critiquing healthcare policies for their implications on the (nurse practitioner) role and the populations for whom they care (NMBA, NP-SoP) as well as promoting the full practice authority for advanced practice nurses (ANA, SSP).
Advocacy and activism for the profession also means addressing structural inequalities that have disempowered nurses: Policies also need to address address systemic structural inequalities that privilege some healthcare professionals over others; for example, committees related to the quality of patient care, standards of care, committee leadership, and the like should include significant nursing representation (ANA, CoE).
Advocacy and activism for system change
Advocacy and activism for system change means a willingness to address persistent, pervasive systemic issues (ANA, SoP) and having political awareness: understand the mechanisms that can be used to influence organisational change and public policy, demonstrating the development of political awareness and skills (NMC, SP-RN).
It can involve working individually or through collective action to bring about social change (ANA, CoE) and for the global health agendas (NMC, RN-SoP): Acting in solidarity, the ability of the profession to influence social justice and global health is formidable (ANA, CoE).
Discussion
In this paper, we set out to explore what nursing regulatory documents from the USA, UK and Australia said about advocacy and activism, and explore how they shape advocacy and activism. We found that advocacy and activism permeate the regulatory documents with a focus on people, equity, ourselves (nurses), the profession and system change. However, advocacy and activism were tempered by gendered and neoliberal forces.
USA regulatory documents had a lot more to say, directly, about advocacy and to a lesser extent, activism. Perhaps this relates to the length of the documents; the USA regulatory documents are far more comprehensive than those from the UK or Australia (190-554 pages for USA, vs 20-48 for UK and Australia). However, beyond having more to say, they were more assertive in placing the profession inside the political arena, claiming advocacy for nurses, and were more tolerant of a certain amount of disruptive action in the form of activism for social reform. Unlike the NMC and NMBA which are federal regulatory bodies, the ANA is a peak body that has an influencing role on regulation. 28 Consequently, the ANA may not have the same requirement to appear politically impartial. In fact, we propose that one of the functions of ANA’s regulatory documents could be to act as a political lobbying instrument. This might tell us that if, internationally, we want to place the profession at the centre of politics, separation between those who write nursing codes and standards and the State, may be required.
Despite the relative lack of direct references to advocacy and activism in UK and Australian documents, we found implicitly documents from all countries direct nurses to undertake advocacy and activism. It appears that each of the ANA, NMC and NMBA are very comfortable with the language of generative and diplomatic advocacy. This is not surprising given the preponderance feminising language in the documents, which buy into the trope of the selfless or angelic nurse, 29 compelling agreeableness and disciplining affect. We can see this gender politics play out in early criticisms of nursing advocacy. Early critics saw this new role dimension as a challenge to nursing identity and a disruption to power and harmony within health services. Initial claims that advocacy was a nursing role were met with scepticism from both inside and outside the profession 30 and some considered it insulting to other professionals. 10 Furthermore, it was seen as taking the role from those more capable and giving it to oppressed and ‘unaspiring, subassertive, organisationally dependent women (p.181)’, 31 ill-equipped to empower patients.
More contemporary critiques have acknowledged the social and institutional structures (medical hierarchy, hospital bureaucracy, and sexism) that concurrently oppress nurses and patients, create a situation where other health professionals remain indifferent to nursing advocacy while at the same time significant consequences are produced for individual nurses who advocate for their patients; repercussions may prevent nurses from speaking. 32 We have previously written about the dark side of civility-based professional culture, 33 how ‘civility’ and ‘professional behaviour’ can be used as a ‘cudgel’ 34 to double-down on undemocratic practices and wilful ignorance. 35 We contend that disagreeableness whether that be through tone or through challenge to hegemonic framework 35 may be a necessary tool or last resort of advocacy and activism for safe healthcare systems.
Intersecting with gender politics, we also found neoliberal influences in the regulatory documents. Placing responsibility on nurses for maintaining their own resilience in stressful workplaces serves to shift the inadequacies of healthcare and political systems onto individual practitioners. Bennet et al 29 provide commentary on how this played out during the COVID-19 pandemic and state that ‘politicians expect servitude, compliance (and even silence) rather than open criticism of their failings (p.2754)’. Others have postulated that this is why activism’s acceptance by regulatory bodies and the wider profession has been slow and somewhat reluctant. In fact, there is some evidence that nursing regulators who once accepted activism as a nursing role, like the Canadian Nurses Association, have turned their back on it. 15 Activism continues to challenge the normative values of nursing identity 16 and presents a risk to and from neoliberalist structures. 15 This is compounded by a tendency for nurses not to recognise their personal or political activities as activism 13 or objecting to being political. Instead, activism has tended to be conceptualised as stand-alone political actions performed infrequently 16 by people with a certain militant disposition.
The manner to which advocacy and activism may contribute to social stratification between nursing roles also requires scrutiny. Though present in the USA regulatory documents, this phenomena was glaring in the Australian standards. Nurse practitioners or advance practice nurses, who have higher incomes, education and power, were afforded the greatest opportunities to advocate politically for their roles. Conversely, there is no provision with the regulatory documents allowing enrolled nurses, who hold the least power in the (regulated) nursing hierarchy,36,37 to advocate for their role. This is despite a persistent scope creep driven by cost-cutting measures that enrolled nurses have not routinely been consulted on and have remained unenthusiastic about. 38 Effectively this both silences a group of nurses who have the most to gain in advocating for their roles and also reduces the number of nurses advocating for the profession.
We also observed how advocacy and activism could be curtailed by certain statements related to adherence to the law in both professional and civic spheres. At face value, and because a function of law is to set the limits of acceptable behaviour for personal and profession life, following the law is a reasonable request. However, the law is set against a political backdrop which is shifting in ways that are important for nursing and healthcare generally, and nursing activism more specifically. For example, across the USA, UK and Australia laws pertaining to activism are becoming more restrictive and aggressively enforced,39,40 limiting the ‘rise of an organized and politically activist working class’ 41 to undertake meaningful protest and direct action 42 and in doing so protect the material interests of the ruling class.41,42
The extent to which these forces warp and colour our five-pointed advocacy and activism star warrants contemplation. Advocacy and activism that cares, nurtures and protects health service users (vulnerable users in particular) dominated the regulatory documents. Consequently, we are convinced that the two star-points ‘advocacy and activism for people’ and ‘advocacy and activism for equity’ are biggest. However, like all the points, they are blunt, dulled by a call to civility and diplomacy at almost all costs. Most certainly this, as well as general lack of perceived nursing power make ‘advocacy and activism for system change’ the smallest point – there were markedly fewer statements in the regulatory documents about it and often these were the purview of advanced practice nurses. We picture ‘advocacy and activism for ourselves’ as a tattered and torn star point, painted in camouflage; the metaphorical war veteran being held responsible for their own shell-shock. Finally, ‘advocacy and activism for the profession’ is short and stair-shaped star point signifying its contribution to social stratification between nursing roles.
At this juncture, we are moved to emphasise that while the US, UK and Australian nursing regulatory documents are supportive of nursing advocacy and activism (even when taking into account the gendered and neoliberal influences), this does not mean they are being translated into nursing practice. A growing body of evidence is calling into question the utility regulatory documents have for clinical practice. For example, in a scoping review of health professionals’ knowledge, awareness and use of professional codes of conduct, Collings-Hughes, Townsend 43 found that professionals knew of the existence of the codes, but were unaware of their content and did not use them routinely. In practice, nurses tend to rely on their own values, common-sense and conform to the social norms of doing ‘what’s right’ in their particular area of work. 44 Increasing demands on increased nursing productivity and lack of experience implementing regulatory documents further dissuade nurses from using regulatory documents or implementing them effectively. 44 Naturally, we implicate gender drivers and neoliberalism in the cocktail of reasons why regulatory documents are not used in practice and further research may provide us with more fully-formed conclusions.
Limitations
Like all research this document analysis has limitations. First, we only conducted the analysis on documents from three jurisdictions, the USA, UK and Australia; a small and white colonial representation of all the codes on offer. We did this because we are nurses from these countries and did not feel it was appropriate to impose our interpretations on codes from countries where we have not worked and have limited cultural understanding. We also used a critical feminist lens which resulted in the identification of gender and neoliberal drivers used within the regulatory documents. This is just one of several important lenses we could have applied to the research. It is likely that conducting this research with another important lens, an anticolonial lens, for example, may have resulted in slightly different and just as useful findings.
Conclusion
Our study contributes to the growing need for research on nursing advocacy and activism, particularly as the profession responds to new and evolving health issues. Our main contribution was demonstrating that regulatory documents from the USA, UK and Australia are supportive of nursing diplomatic advocacy and activism towards people, equity, ourselves (nurses), the profession and systems change. More oppositional and disruptive advocacy and activism, however is constrained by gendered and neoliberal subtexts which depoliticise the role of the nurse. We caution that while the regulatory documents might be supportive of advocacy and activism, this does not automatically translate to practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the American Nursing Association, The Nursing and Midwifery Council (UK) and the Nursing and Midwifery Board of Australia. Restrictions apply to the availability of the American Nursing Association documents.