
Abstract
Introduction
In the past decade, the concept of professional competence in nursing has been examined in light of various challenges, including rapid technological advancements, changes in the spectrum of diseases, an aging population, and more. 1 These developments have contributed to the emergence of increasingly complex ethical dilemmas for nurses, often leading to role confusion, moral conflicts, and value conflicts. 2 Previous studies have revealed that nurses face moral dilemmas almost on a daily basis.3,4 The purpose of the present study is to examine the relationship between nurses' moral sensitivity in decision-making during moral dilemmas—considering professional factors, patient well-being, and consultations with experts and colleagues—and their moral self and moral integrity.
Background
Beauchamp and Childress 5 proposed a procedural framework for shaping moral decisions and established a foundation of agreed-upon bioethical principles that can guide moral decision-making. These principles include autonomy, beneficence, prevention of harm, and justice. They provide an infrastructure upon which nurses can base their moral decisions. However, in certain situations, nurses may encounter conflicts between their professional, social, and/or personal values, leading to ethical dilemmas that require them to make difficult moral decisions. 6 These conflicts can arise when different values or principles come into tension, and the nurse must navigate through the complexities of the situation to determine the most appropriate course of action. Ethical decision-making in nursing involves the ability to make appropriate decisions regarding ethical issues by drawing on intuitive ethical nursing principles, professional values, codes of moral judgment, and moral reasoning. 7 One significant factor influencing decision-making abilities, as evident in the literature, is the moral sensitivity of nurses.8,9
Moral sensitivity was initially defined by Lützén et al. (1995) 10 as an individual’s capacity to navigate ethical conflicts within specific situations, particularly in the interpersonal relationships between patients and nurses. A more recent definition by Amiri et al. 3 characterizes moral sensitivity as nurses' awareness of patient vulnerability and their ability to anticipate the outcomes of moral decision-making, which enables them to make morally sound decisions on behalf of their patients. 11
Moral sensitivity encompasses cognitive abilities that are influenced by individual experiences, personal development, the experiences of others, and various value systems. Consequently, moral sensitivity stands as one of the foundational elements of professional nursing competence, fostering qualities such as patience, composure, and a sense of responsibility toward caregivers. It should be noted that moral sensitivity extends beyond an individual’s perception of what is right; it also encompasses personal experiences and the capacity to recognize the significance of the ethical issue at hand. 8
Numerous studies have identified associations between moral sensitivity and variables related to caregiver decision-making processes, the quality of patient care, compassionate behavior, and patient satisfaction.3,9,12
In light of these findings, the present study aims to examine two personal variables, moral self and moral integrity, as components of moral identity, which may serve as predictors of moral sensitivity.
Many studies have been conducted since the 1950s to examine moral development. While classical theorists such as Kohlberg 13 or Bandura 14 have proposed models for examining moral judgment, these models do not explain the gap between a person’s moral judgment and actual behavior. 15 Studies conducted since the 1980s have suggested “moral identity” as a mediating variable, explaining the gap between moral judgment and moral action. Moral identity (MI), also called the moral self concept, is defined as the extent to which being a moral person is a central aspect of the person’s identity.16,17 Moral identity describes whether several desirable moral traits (e.g., being fair, caring, kind) are seen as important to oneself as a person. 18 Studies have found that moral identity is positively related to empathy and prosocial behavior and negatively related to antisocial behaviors.19,20 Hence, an individual’s sense of moral identity can provide information about how he or she may choose to act in different situations. 17
The main model in the field is the Blasi model,21,22 which assumes that a person facing a moral dilemma first determines the morally right action and then whether that action is obligatory. This decision serves as the motivating force leading to moral action. When people see themselves as moral beings, they are more likely to interpret situations in a moral manner and act accordingly. According to Blasi, once a moral value is integrated into one’s identity, an individual will be motivated to act in accordance with that value when their moral understanding appeals to it in making a moral judgment. This is because the moral concern has become a personal concern. As Blasi 21 states, “it seems likely that the highest degree of moral integration is achieved when one’s moral understanding and concerns become a part of one’s self-concept, of the specific way one views and defines oneself” (p. 242). Blasi often expresses this idea by suggesting that a moral judgment transforms into a judgment of personal responsibility, thereby motivating the individual to engage in the corresponding moral action.
Accordingly, Black and Reynolds suggested that moral identity consists of two separate yet interrelated components: moral self and moral integrity. The moral self is sustained by the importance people place on being moral and measures how closely they identify with moral values. Moral integrity refers to the desire to align intention and action, examining how much value a person places on acting according to moral principles. The moral self expresses an internal commitment to moral principles, but it will only be manifested in the case of high moral integrity, where an individual feels obligated to act in accordance with these principles. For example, Borhani et al. 8 examined the relationship between moral self-concept and moral sensitivity in Iranian nurses but did not consider moral integrity as the mechanism that may mediate between the two variables.
Considering the research literature, which illustrates the importance of moral sensitivity in the work of nurses, the purpose of the present study is to examine the relationship between the moral sensitivity of nurses, as expressed in professional considerations, in reference to the patient’s well-being and in consultation with experts and colleagues, and between the moral self and their moral integrity.
The research hypotheses are as follows: (1) There will be a positive correlation between moral self, moral integrity, and moral sensitivity in decision-making among nurses. (2) There will be a negative correlation between seniority in the nursing profession and job percentages, and moral sensitivity in nurses’ decision-making across all its components. (3) Moral integrity, which encompasses a nurse’s commitment to act according to moral principles, will mediate the relationship between moral self and moral sensitivity.
Methods
Participants
The study sample included 187 nurse participants, 160 (85.6%) women and 27 men (14.4%), forming a convenience sample. The age of the participants ranged from 20 to 69 (M = 41.92; SD = 10.96); 81.8% of the participants were Jewish, 15.5% were Moslem, 38% were secular, 23.5% were traditional, and 38.5% were religious. The participants’ mean education was 17.1 years (SD = 3.09). The average years of seniority in the nursing profession was 16.08 years (SD = 11.8).
Tools
The study was conducted using a quantitative questionnaire consisting of three parts. All research questionnaires used in this study are openly available in academic databases and are licensed for academic use. (1) The demographic questionnaire included questions about the participants’ age, gender, place of residence, level of religiosity, years of education, seniority in the nursing profession and percentage of positions. (2) The moral identity questionnaire (MIQ) was designed by Black and Reynolds
23
to assess the importance people give both to their moral principles and to acting accordingly, independently of religious or political views. The questionnaire is a 20-item self-report inventory divided into two parts: Items 1–8 correspond to the moral self-subscale and Items 9–20 correspond to moral integrity. Study participants were asked to indicate the extent to which they agree with the statement on a scale of 1–5 (1 = Strongly disagree to 5 = Strongly agree).
The moral self subscale measures how closely participants identify with moral values. Sample items are “Not hurting other people is one of the rules I live by” and “I want other people to know they can rely on me.” The Cronbach’s alpha reliability of the questionnaire was.789 for this study. A high score indicates a higher moral self.
The moral integrity subscale measures the desire to make intention and action consistent and how much value participants place on acting according to moral principles. The MIQ-MI evaluates integrity in the sense of equality of private and public action. Sample items include: “Once I have made up my mind about what is the right thing to do, I make sure I do it,” and “There is no point in going out of my way to do something good if no one is around to appreciate it.” The Cronbach’s alpha reliability of the questionnaire was .704 for this study. Since the wording of the variable was opposite to that of the moral self, a scale reversal was made such that a high score indicates higher integrity. (3) The moral sensitivity of nurses questionnaire
12
has 27 items rated on a five-point scale from “not at all” (1) to “strongly agree” (5). Han et al.
12
reported acceptable internal consistency for the total scale (α = .76) and found five subscales composing it, explaining 45.5% of the total variance. In our current study, the internal consistency for the total scale was similar, α = .74, yet the consistencies for the five subscales were too low. Considering the cultural differences between Korean
12
and Israeli nurses and the time that elapsed between the studies, we conducted principal components factor analysis with oblique rotation for the current sample. The principal components factor analysis included three factors, explaining 66.00% of the variance.
Factor 1: “Exercising professional judgment” had eight items, with eigenvalue = 1.50, α = .69. Sample items include the following: “If I am not familiar with the personal history of a patient, I rely on the common procedures” and ‘When I need to make a decision against the will of my patient, I do what I believe to be in his or her best interest.
Factor 2: “Patient-centered care” has 9 items, with eigenvalue = 1.47, α = .67. Sample items include the following: “Whenever I make a difficult decision, it is important for me to always be honest with the patient” and “I believe that the nurse–patient relationship is the most important component in psychological nursing care.”
Factor 3: “Using knowledge bases” has 10 items, with eigenvalue = 1.31, α = .69. Sample items include the following: “When I am unsure about what to do, I rely mostly on the other nurses” knowledge about a patient’ and “I always base my actions on nursing knowledge of what is the best approach, even if a patient protests.”
The three scores, as well as the total scale score, were computed with item means, such that higher scores represent higher moral sensitivity.
Research process
The study was approved by the Ethics Committee of the university (approval no. AU-HEA-LO-20220317). After obtaining the approval of the University’s ethics committee, the study was carried out after obtaining participants’ informed written consent.
The research questionnaires were administered to a convenience sample of Israeli nurses in the course of 2023. The questionnaire was distributed through social networks and groups designed for nurses, such as Facebook and WhatsApp groups.
Participants were guaranteed that the survey was anonymous, that it was intended for research purposes only and that participants could stop answering the questionnaire at any stage. Participation in the research was voluntary. It was also clarified that there were no correct answers to questions in the questionnaires, and participants were asked only to express their opinions.
Findings
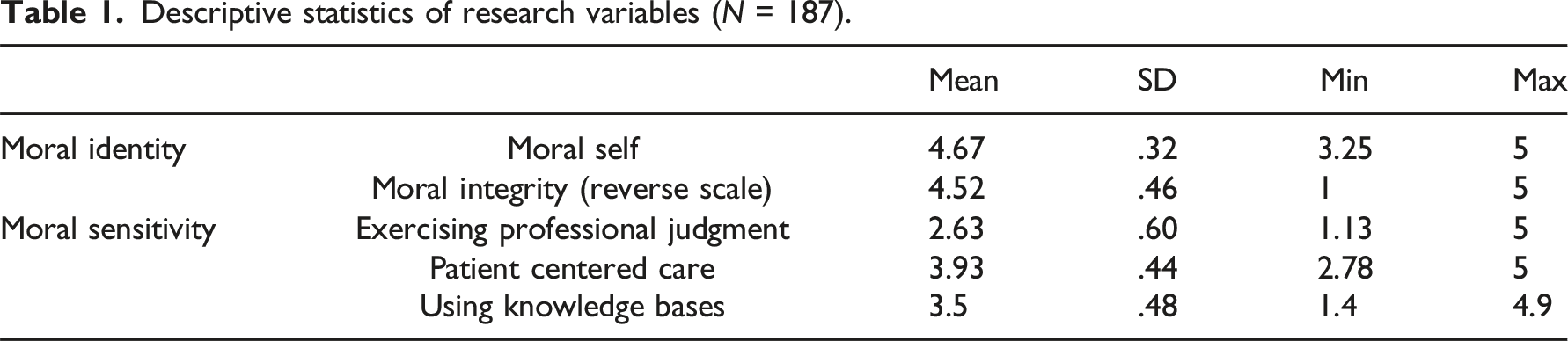
Descriptive statistics of research variables (N = 187).
Correlations between research variables (N = 187).
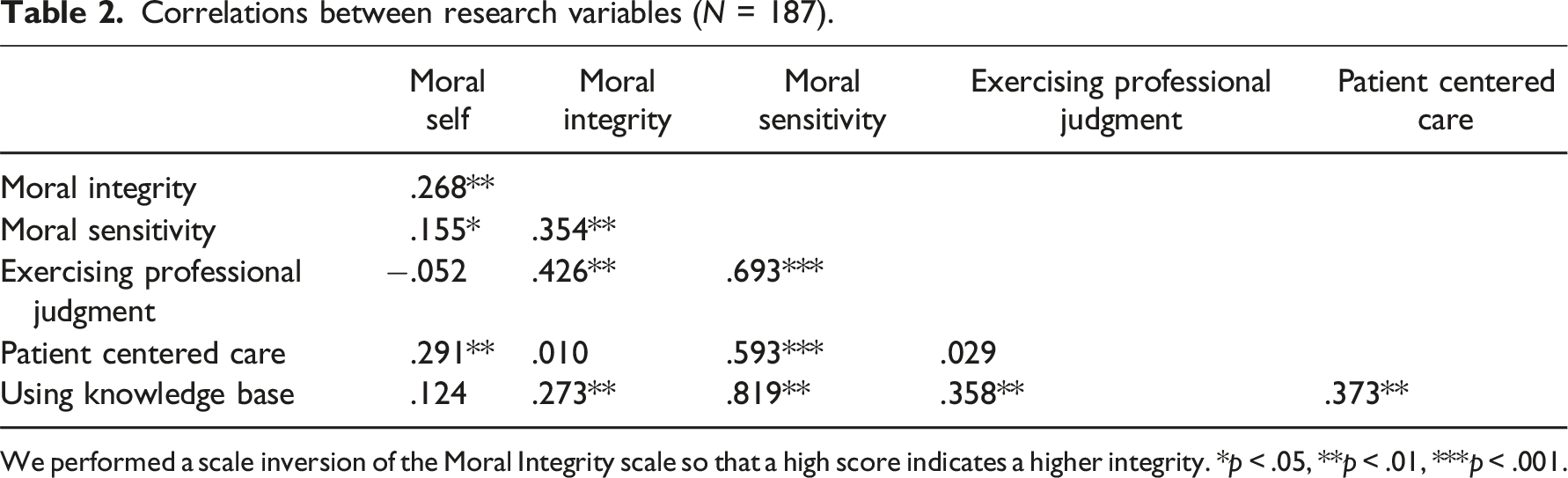
We performed a scale inversion of the Moral Integrity scale so that a high score indicates a higher integrity. *p < .05, **p < .01, ***p < .001.
The findings presented in Table 2 provide several noteworthy results:
Consistent with the first hypothesis, there is a significant positive correlation between moral self and moral integrity. That is, the more the study participants identified with moral values, the more they felt obligated to act on them.
Regarding the associations between moral identity and decision-making among nurses, we found that there is a positive correlation between moral self and patient-centered decision-making (attention to his requests and well-being). No correlation was found between moral self and the other components of moral sensitivity in decision-making: objective professional judgment or the use of different knowledge bases. This finding indicates that the moral identity of the nurses is expressed more in the interpersonal aspects and relationships with patients, and less in professional issues.
In contrast, moral integrity shows the opposite trend. Moral integrity, which expresses a match between moral perceptions and moral behavior, has been found to be related to both professional judgment and the use of knowledge bases for decision-making. However, it was not found to be related to patient-centered decision-making.
Surprisingly, and contrary to the second hypothesis, we did not find significant correlations between demographic variables, such as age, seniority in the nursing profession, and job percentages, and moral sensitivity in decision-making (r = .061, .035, .183, p > .05, respectively).
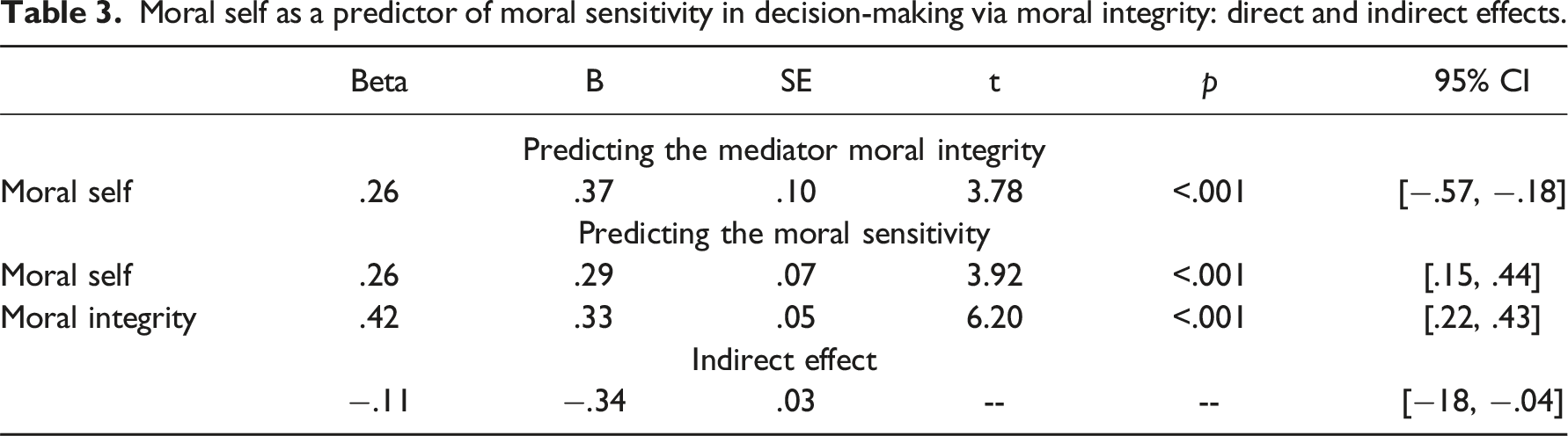
To test the third hypothesis that moral self-perceived moral sensitivity in decision-making occurs via moral integrity, a mediation analysis was conducted using Model 4 of the add-on process macro. 24
The findings of the mediation model are presented in Figure 1 and Table 3. The findings indicate that moral self is related to increased moral integrity, which, in turn, is associated with increased moral sensitivity. The significance test of the mediation effect yielded a confidence interval that did not include the value 0. This finding is equivalent to a statistically significant effect. Moral self predicting moral sensitivity in decision making via model integrity. The figure presents standardized values. The total effect is presented in parentheses. *p < .05, *p < .01, *p < .001. Moral self as a predictor of moral sensitivity in decision-making via moral integrity: direct and indirect effects.
Ethical considerations
Prior to its execution, the study received the approval of the Ethics Committee of Ariel University (number: AU-HEA-LO-20220317). All study participants signed an informed consent to participate in the study. They were informed that their participation was entirely voluntary, that they could stop filling out the questionnaire at any time, and that the research was anonymous. No identifying information was collected from them to ensure confidentiality. The research underwent a thorough ethical review to ensure adherence to ethical standards and practices. Permission to use the research tools was granted, and these tools are publicly available, with appropriate references provided as required.
Discussion
This study aimed to investigate the relationship between moral self, moral integrity, and moral sensitivity in decision-making. Understanding the variables associated with moral sensitivity in decision-making among nurses is crucial. Previous studies7,25,26 have demonstrated that nurses with high moral sensitivity make thoughtful decisions and exhibit professional responsibility, striking a balance between potential risks to the patient and treatment benefits, thus reducing the risk of harm. In the current study, most of the participating nurses exhibited a high level of moral sensitivity.
Upon examining the components that constitute moral sensitivity, it was found that the most significant component identified by the nurses was “patient-centered care.” This component primarily refers to addressing the patient’s needs, requests, and suffering.27,28 The high value placed on “Patient-Centered Care” by the nurses in this study reflects the procedural framework of Beauchamp and Childress for shaping moral decisions. According to this framework, moral decisions are based on the principles of patient autonomy, beneficence, prevention of harm, and justice. Bogaert highlights the potential conflicts between these principles; for example, prioritizing patient autonomy might sometimes conflict with the need to prevent harm. However, the findings of this study indicate that nurses view autonomy as a cornerstone of their practice.
The next most important component was “Using knowledge bases,” followed by “Exercising professional judgment.” Moral sensitivity focused on “patient-centered care” reflects the principle of prioritizing patient orientation, sometimes even above all others. Conversely, sensitivity focused on the use of knowledge bases and professional judgment reflects the incorporation of facts, information, and skills necessary for nurses to be competent and self-aware. 29 The knowledge base includes both a professional knowledge base, acquired through basic and continuing education and experience, and a situational knowledge base, which pertains to patient-specific knowledge obtained through assessment. 28
The findings of the research indicate a distinction between the elements of moral sensitivity among nurses. While patient-centered care correlates with nurses' moral self, the formal aspects of moral sensitivity, such as the use of knowledge bases and professional judgment, are associated with their moral integrity. This differentiation aligns with the concept proposed by Parens 30 and Catlett, 31 which posits two paradigms of moral justification: the “good” and the “right.” The “good” paradigm emphasizes actions that prioritize patient well-being, considering personal values, social understanding, and cultural preferences. In contrast, the “right” paradigm focuses on decisions grounded in medical and physiological considerations, guided by laws, procedures, norms, rights, obligations, and treatment protocols within the biomedical model. In this study, patient-centered care embodies the “good” paradigm, while the use of knowledge bases and professional judgment represents the “right” paradigm.
In light of the identified relationships between the elements of moral sensitivity, as well as between moral self and moral integrity, integrating these two paradigms can enhance patient care from a moral perspective. Patients benefit from both empathetic consideration of their needs facilitated by nurses' moral self and from informed, professional treatment resulting from nurses' moral integrity.
This explanation is reinforced by the mediation model proposed in this study, suggesting that moral integrity mediates and strengthens the relationship between moral self and moral sensitivity. Consequently, a high level of moral sensitivity, characterized by both interpersonal sensitivity toward patients and informed, professional decision-making, occurs when there is a combination of high moral self and high moral integrity.
From a practical standpoint, these findings hold relevance for nursing education. Nursing education plays a crucial role in cultivating moral and ethical decision-making, encompassing both clinical competence and ethical sensitivity. Strengthening moral self and moral integrity among nursing students can facilitate balanced and morally sensitive decision-making, while also establishing moral and ethical support systems to assist students in distressing and emergency situations. 32
Despite its importance, this study has several limitations. First, a convenience sample methodology was utilized, limiting the generalizability of the findings to a larger population. Furthermore, due to the sample size, differences between various nursing roles, such as emergency teams, were not explored. In these cases, the decision-making process may vary. Last, the study focused on a limited number of research variables to explain moral sensitivity among nurses. Future studies should expand the scope by investigating the contribution of personality factors and situational factors in understanding the combination of moral sensitivity in decision-making. 33
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.