
Abstract
Background
A psychosocial problem faced by people with early-stage dementia (PwESD) is the perception of threats to personal dignity. Insights into its dynamics are important for understanding how it changes as dementia advances and to develop suitable interventions. However, longitudinal studies on this change in PwESD are lacking.
Aims
To determine how perceptions of dignity and selected clinical and social factors change over 1 year in home-dwelling PwESD and the predictors associated with changes in perceptions of dignity over 1 year.
Research design and methods
A longitudinal study was conducted. The sample included 258 home-dwelling Czech PwESD. Data were collected using the Patient Dignity Inventory (PDI-CZ), Mini-Mental State Examination, Bristol Activities of Daily Living Scale, Geriatric Depression Scale and items related to social involvement. Questionnaires were completed by the PwESD at baseline and after 1 year.
Ethical considerations
The study was approved by the ethics committee and informed consent was provided by the participants.
Results
People with Early-Stage Dementia rated the threat to dignity as mild and the ratings did not change significantly after 1 year. Cognitive function, self-sufficiency, vision, and hearing worsened, and more PwESD lived with others rather than with a partner after 1 year. Worsened depression was the only predictor of change in perceived personal dignity after 1 year, both overall and in each of the PDI-CZ domains. Predictors of self-sufficiency and pain affected only some PDI-CZ domains.
Conclusions
Perceptions of threat to dignity were mild in PwESD after 1 year, although worsened clinical factors represented a potential threat to dignity. Our findings lead us to hypothesise that perceived threats to personal dignity are not directly influenced by health condition, but rather by the social context.
Introduction
Dementia is one of the most feared diseases in contemporary society, often referred to as ‘living death’. 1 It affects cognitive functions such as memory and logical thinking. It leads to a reduction in a person’s independence and autonomy, which affects personal dignity. 2 The sense of personal dignity is not fixed. Therefore, the dynamics of perceived threats to personal dignity may change as dementia progresses. 3 A comprehensive view of how the development of dementia and symptom progression may affect personal dignity over time in home-dwelling PwESD is currently lacking. Understanding these dynamics could motivate home care nurses and other professionals to incorporate a brief psychotherapeutic intervention (e.g. Dignity Therapy) aimed at enhancing the sense of personal dignity of PwESD and their family carers. 2 This would fill the existing gap in comprehensive dementia care for people with dementia in the home setting. Therefore, our research aims to investigate how perceptions of personal dignity change in home-dwelling PwESD after 1 year.
Background
Demographic ageing is a global phenomenon that has increased the proportion of older adults in the population. By 2050, people aged 65 years and above will account for approximately 16% of the world’s population. 4 Similar to other European countries, the Czech Republic is experiencing a significant increase in the proportion of older people. Consequently, the number of people with dementia is also expected to increase, as age is a significant risk factor for dementia. 5 Given the projected trend of population ageing and the associated increase in the number of people with dementia, it is appropriate to explore how people with dementia living at home perceive their personal dignity.
Dementia is an umbrella term for several diseases that affect memory, thinking and the ability to perform daily activities. 5 During the early stages of dementia, symptoms are milder, and people may live independently (or with supervision and support) in their home environment and participate in social activities. 6 Confirmation of a serious diagnosis triggers many emotions and can cause existential suffering, including anxiety about death 7 or a desire to die because life seems empty and meaningless. 3 Depression can exacerbate negative experiences of emotional or physical dependence on others and is often associated with the loss of social engagement and subjective lack of dignity. 8
In nursing ethics, dignity is a fundamental concept. Its main attributes are personhood (a unique human being with specific characteristics and inalienable human rights, 9 sociability (relational and behavioural), respect (includes self-respect, respect for others, respect for privacy and confidentiality) and autonomy (includes independence, freedom of choice and decision making). 10
Personal dignity encompasses psychological and social dimensions 11 and significantly influences an individual’s sense of meaning in life 12 and their ability to integrate into society. A sense of personal dignity is influenced by internal (how I perceive myself) and external (how others perceive me) attributes. 13 Personal dignity is contingent and contextual, unlike universal human dignity, which is a fundamental human value associated with human rights. 14 It is a multidimensional construct 3 associated with autonomy, purpose of life, confidence and social support. 15 Autonomy represents personal independence, choice and control.6,16 It can be undermined by sensory deficits in vision and hearing, as they limit the individual’s ability to perform activities independently and increase their dependence on others.11,17 Similarly, cognitive impairments (e.g. memory or executive function deficits) have a significant impact on an individual’s autonomy and thus threaten their personal identity. 14 Perceptions of personal dignity are largely related to the meaning of life, which is a subjective sense of purpose, including an understanding of life circumstances and meaning. 12 It can be influenced by physical symptoms of illness (e.g. pain), loss of motivation to seek meaning and purpose in one’s existence or feeling a burden to others. 12 The category of confidence relates to how patients interact with carers and how they behave towards each other. Confidence includes having a balance between one’s own wishes and those of others, being able to participate and being free. 18 It can be influenced by mental and existential insecurity, depression and anxiety. 15 Social support includes support within a close circle of family and friends, feeling socially included in an extended social network (outside the family), and actively living a meaningful life within a social community. 19
The underlying psychosocial problem faced by people with early-stage dementia (PwESD) is their perceived threat to personal dignity, which is associated with a sense of loss of self-esteem and self-worth. 20 PwESD are at risk of losing personal dignity, both directly, through the impact of illness on self-identity, and indirectly through negative social interactions and experiences. 21 In addition to cognitive problems, social issues, such as stigmatisation by others and changes in social status, can threaten the personal dignity of PwESD,1,22 causing emotional or social isolation23,24 and impacting their social environment. 6 Conversely, they can find a sense of meaning and dignity if surrounded by a cohesive and supportive social network, 25 which, in this study, refers to a person’s social capital, including the resources related to social ties. 26
PwESD often cite a sense of social inclusion in a wider social network, 19 autonomy (including personal independence, choice and control),6,16 effective pain management 13 and adequate self-sufficiency as factors that support the maintenance of their personal dignity. 13
Over the last decade, several studies have focused on how the experience of dignity affects the well-being of PwESD.6,19,27,28 However, few studies have longitudinally investigated the dynamics of perceived dignity over the course of the illness. The research has primarily focused on PwESD in institutional care.29,30 According to our findings, no study has longitudinally monitored the dynamics of perceived dignity in home-dwelling PwESD. However, this insight is important to understand how PwESD perceive their personal dignity and how their views of dignity change with the progress of dementia. Knowledge of trajectories can help community nurses and other health professionals to implement interventions that support the maintenance of personal dignity in PwESD, such as Dignity Therapy.2,31
Aim
Our study aimed to investigate the following in home-dwelling PwESD: how perceptions of personal dignity changes over 1 year? (Research Question 1); how selected clinical and social factors change? (Research Question 2); and which predictors are associated with changes in perceptions of personal dignity over 1 year? (Research Question 3).
Methods
Research design
This study is part of the first longitudinal study examining the dynamics of perceived dignity in PwESD in CR (registered at https://www.clinicaltrials.gov/ before the first patient was enrolled). We used a battery of questionnaires to collect data.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and the study protocol was approved by the Ethics Committee of the Faculty of Health Sciences of Palacky University Olomouc, CR. The data were collected in accordance with the ethical principles of informed consent, confidentiality and the participants’ right to withdraw at any time without providing reasons. All participants signed an informed consent form prior to inclusion in the study and were not at risk of harm from participation.
Participants and research context
The sample consisted of older people who met the following criteria: (1) aged 60 years or above, (2) diagnosed with any type of at an early stage (Mini-Mental State Examination [MMSE] score of 20–25 points) and (3) living at home. Exclusion criteria were (1) total immobility, (2) presence of a major psychiatric disorder (schizophrenia or bipolar affective disorder) or (3) undergoing palliative treatment for cancer or non-cancer conditions.
The sample size was based on an expected difference of 0.5 points on the Patient Dignity Inventory (PDI-CZ) over 1 year. Pre-study calculations showed that a minimum of 220 participants would be needed to reach a significant difference, with an α of 0.05 (two-tailed) and a β of 0.8, assuming that approximately 40% of participants would not complete the questionnaires at both stages (at enrolment and after 1 year), and a total of 310 PwESD were screened. The final sample included 258 participants who completed the questionnaire at baseline and after 1 year.
The questionnaire battery
The questionnaire comprised three parts. The first part contained the Czech versions of standardised assessment instruments focusing on dignity and selected clinical factors (depression, pain, cognition and self-sufficiency). The second part comprised selected items related to the social involvement of PwESDs (participation in social activities, frequency of social contact with people not living in the same household and time spent alone). The third section included basic demographic data (age, sex, education and living arrangements).
Instruments
The PDI-CZ, the Czech version of the PDI developed by Chochinov et al., 32 is a self-assessment screening tool assessing the issues affecting patient dignity. The PDI was originally designed for patients who are terminally ill but can also be used for PwESD. 31 It contains 25 items rated on a five-point Likert scale. Participants rated the extent to which each item affected their sense of dignity (1 = not a problem to 5 = a major problem). The total score ranges from 25 (i.e. no threat to dignity) to 125 and can be divided into categories of threat to dignity: ‘none’ (25), ‘mild’ (26–49), ‘moderate’ (50–74), ‘severe’ (75–99) and ‘very severe’ (100–125). 12 The PDI-CZ has items divided into four domains based on factor analysis. The Meaning of Life domain includes 13 items (i.e. Feeling physically distressing symptoms, Worried about future, Feeling life no longer has meaning or purpose, Not feeling worthwhile or valued). The Autonomy domain consists of five items (i.e. Not able to perform tasks of daily living, Feeling how you look has changed, Not being able to continue usual routines). The Confidence domain includes four items (i.e. Feeling depressed, Not being able to think clearly). The Social Support domain includes three items (i.e. Not feeling supported by friends and family, Not being treated with respect). 15
For the assessment of depressive symptoms, we used the Geriatric Depression Scale (GDS) with 15 self-report items. Items focus on assessing life satisfaction, mood, feelings of happiness, helplessness, uselessness and hopelessness. The total score ranges from 0 to 15. The total score ranges from 0 to 15. Scores of 0–4 are considered normal (depending on age, education and complaints), 5–9 indicate mild depression and 10–15 indicate moderate to severe depression. 33 The GDS is a reliable and valid self-rating scale for screening depression in individuals with mild-to-moderate dementia34,35
Pain intensity was measured using the Horizontal Visual Analogue Scale (HVAS). It consists of a 10 cm line anchored by two extremes (no pain and extreme pain). It can be used in older adults with mild-to-moderate dementia. 36
Self-sufficiency was assessed using the Czech version of the Bristol Activities of Daily Living Scale (BADLS-CZ). 37 The BADLS 38 was designed for caregivers (a close person) of home-dwelling PwESD. The scale assesses the performance in 20 activities (basic and instrumental activities of daily living) and ranges from completely independent to completely dependent. This is particularly important in patients with dementia. The total score ranges from 0 to 60, with higher scores representing a greater degree of dependence.
The Mini-Mental State Examination (MMSE) 39 was used to assess cognitive functions. The MMSE assesses global cognitive function and degree of impairment. Orientation, memory, attention and calculation, short-term memory, speech, communication and executive function were assessed. The maximum possible score was 30, with higher scores indicating better cognitive performance.
Visual and hearing impairments were assessed by a clinician using a screening test for distance and near visual acuity (optotype) and a subjective hearing test (speech test). Responses were dichotomised as no/minimal or moderate/severe impairment.
Data collection
Home-dwelling PwESD were approached through geriatric and neurological outpatient clinics, where they were treated for dementia. Their physicians requested them to participate in the study during regular check-ups. Those who signed informed consent forms were included in the study. The research nurses, who were trained in administrating the instruments included in the questionnaire battery, taught participants how to complete the questionnaires (either independently or through structured interviews with the research nurse). The study was conducted from January 2021 to September 2022 in four regions of the CR (Olomouc, Hradec Králové, Prague, and Ostrava).
Data analysis
Qualitative data were described using absolute and relative frequencies. Differences between the first and second measurements were tested using McNemar’s test. Quantitative variables were presented as means and standard deviations (SD). A paired t test was used to compare the two dependent samples. The parametric method was used because the sample size was sufficiently large. Predictors of changes in perceived personal dignity were examined using multivariate linear regression. All tests were performed at a significance level of p < .05. IBM SPSS Statistics for Windows (Armonk, NY: IBM Corp) version 23.0 was used for statistical analyses.
Results
Characteristics of participants
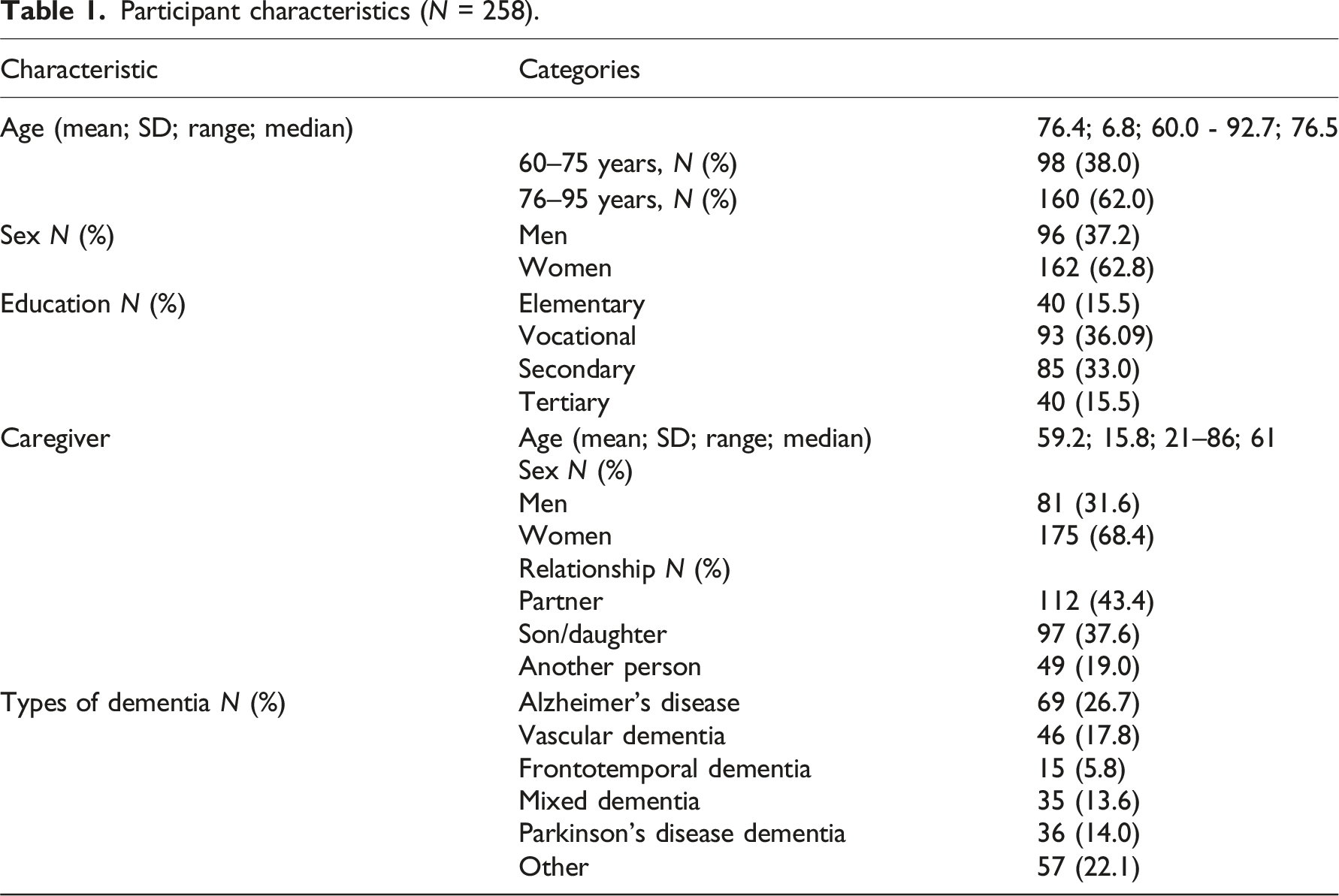
Participant characteristics (N = 258).
Changes in social, clinical and psychological variables
Social, clinical and psychological characteristics of participants and changes at 1 year.
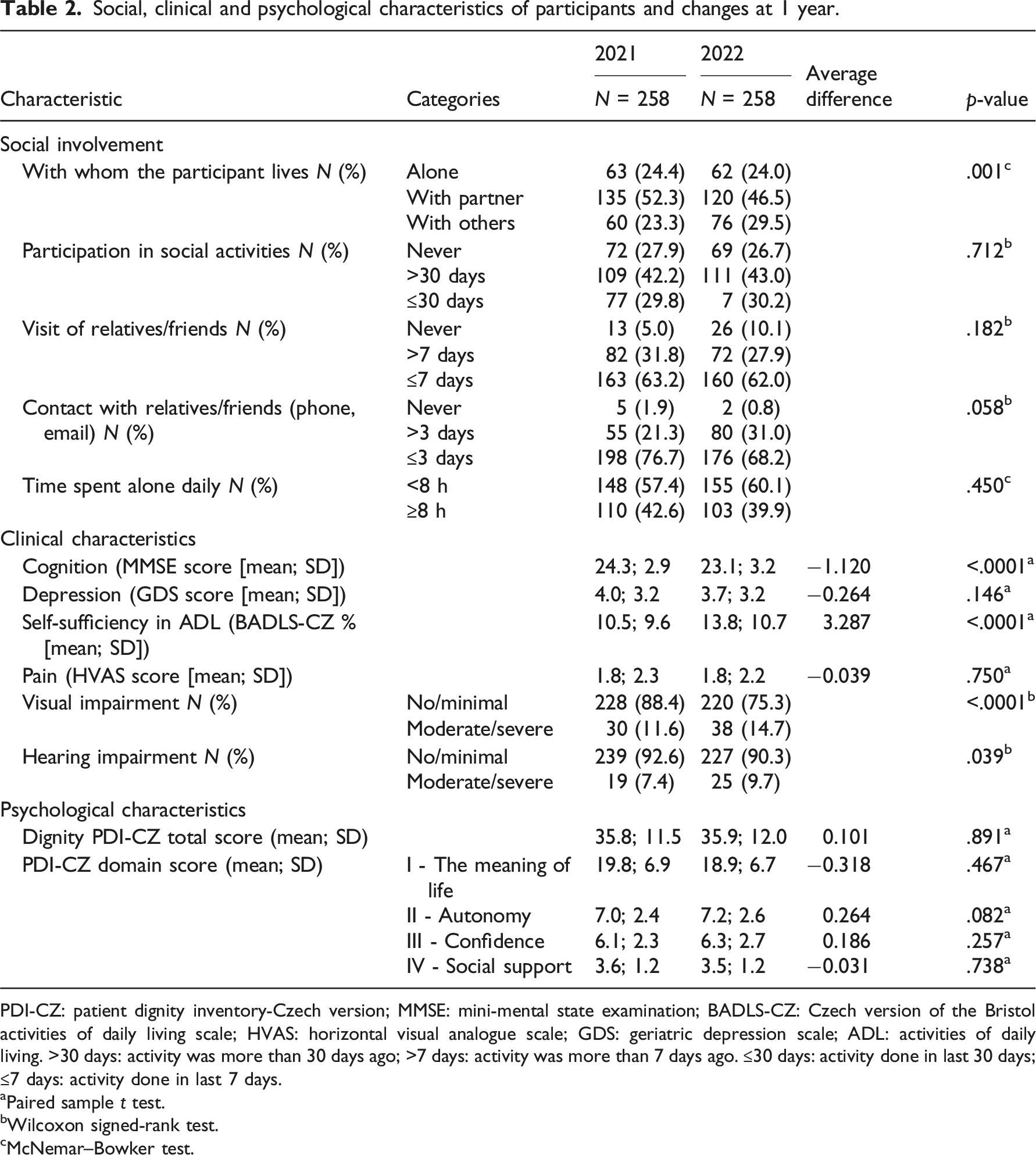
PDI-CZ: patient dignity inventory-Czech version; MMSE: mini-mental state examination; BADLS-CZ: Czech version of the Bristol activities of daily living scale; HVAS: horizontal visual analogue scale; GDS: geriatric depression scale; ADL: activities of daily living. >30 days: activity was more than 30 days ago; >7 days: activity was more than 7 days ago. ≤30 days: activity done in last 30 days; ≤7 days: activity done in last 7 days.
aPaired sample t test.
bWilcoxon signed-rank test.
cMcNemar–Bowker test.
Predictors of change in perception of personal dignity
Predictors of change in perceived dignity after 1 year.
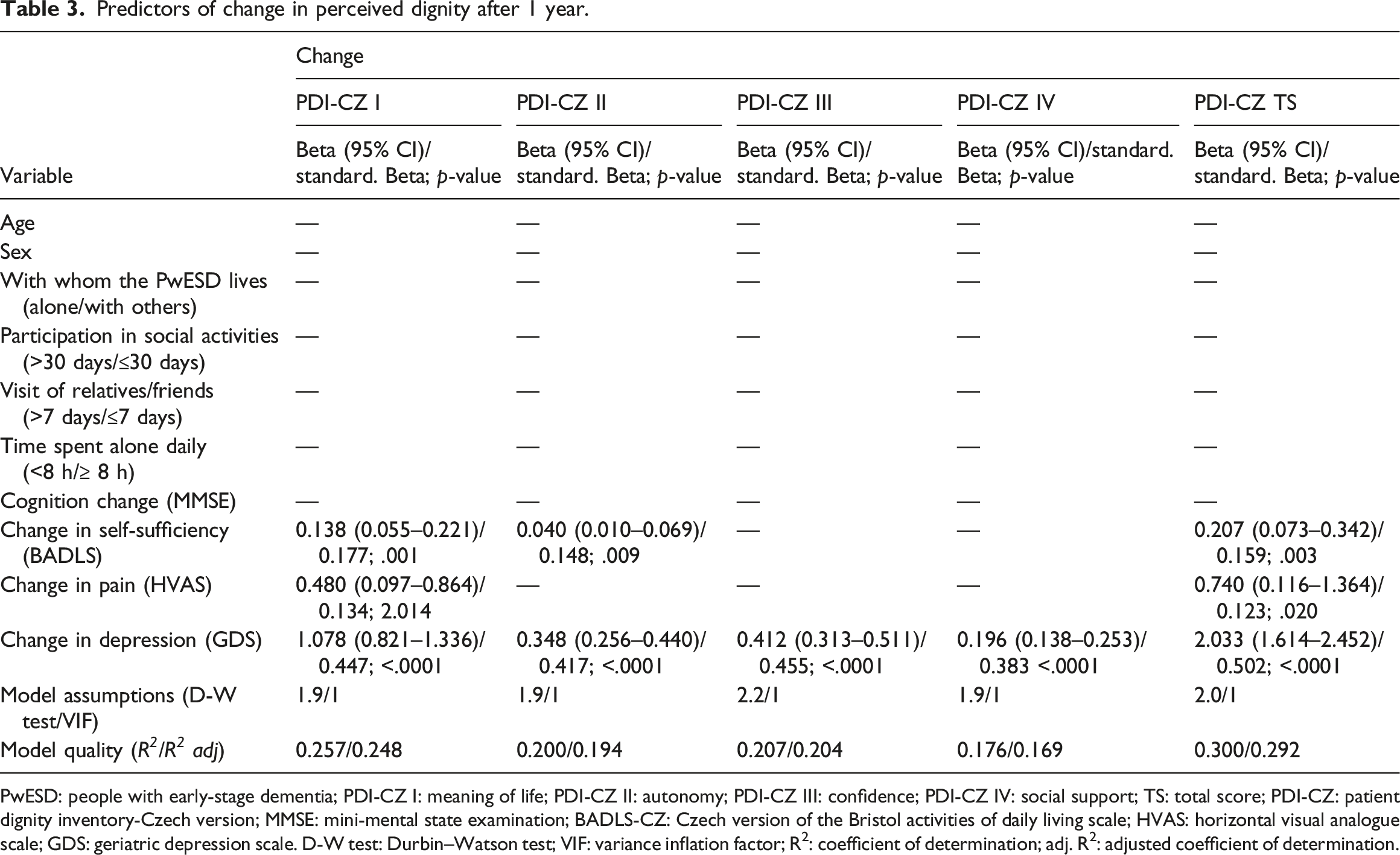
PwESD: people with early-stage dementia; PDI-CZ I: meaning of life; PDI-CZ II: autonomy; PDI-CZ III: confidence; PDI-CZ IV: social support; TS: total score; PDI-CZ: patient dignity inventory-Czech version; MMSE: mini-mental state examination; BADLS-CZ: Czech version of the Bristol activities of daily living scale; HVAS: horizontal visual analogue scale; GDS: geriatric depression scale. D-W test: Durbin–Watson test; VIF: variance inflation factor; R2: coefficient of determination; adj. R2: adjusted coefficient of determination.
Table 3 presents the results of the linear regression analysis. Deterioration in perceptions of personal dignity after 1 year on the PDI-CZ total and Domain I (Meaning of Life) scores were predicted by worsened depression (stand. ß = 0.502; 0.447, respectively), self-sufficiency (stand. ß = 0.159; 0.177, respectively) and pain (stand. ß = 0.123; 0.134, respectively); that on Domain II (Autonomy), by worsened depression (stand. ß = 0.417) and self-sufficiency (stand. ß = 0.148) and on domains III and IV (Confidence and Social support), by worsened depression (stand. ß = 0.455; 0.383, respectively).
Discussion
This study aimed to determine whether perceptions of personal dignity, social, and clinical characteristics change in PwESD after 1 year and the predictors of these changes.
The home-dwelling PwESD rated the threat to personal dignity as mild. Although the clinical indicators associated with progressive dementia worsened, no greater impairment of personal dignity was perceived. This finding is consistent with the dignity in illness model, which suggests that it is not the illness (in our case, dementia) but the changes in personal and social circumstances that are directly responsible for the perceived threat to personal dignity in PwESD. 12 After 1 year, the social indicators have not changed significantly, except that people are living less with their partner and more with others. This may be one reason why people’s sense of dignity has not been affected. We suggest that the reason why cognitive impairment and social activities were not predictors of changes in dignity may be that PwESD were able to continue living in their own homes with their loved ones. This allowed them to maintain their social roles and control over their lives. 6 Home environment, relationships with partners and immediate family members are essential for PwESD. This provides them with the opportunity to perform meaningful daily activities in familiar environments. Thus, the meaning of a house (apartment) goes beyond its basic function as a dwelling and represents a symbol of the identity that the PwESD has built in their life. 6 The opportunity to experience positive aspects of emotional functioning, meaningfulness, social inclusion and life satisfaction are important psychological resources that PwESD develop to cope. 19 This helps prevent the potentially harmful effects of illness on personal dignity. 3 However, PwESD can also maintain their personal dignity by lowering their expectations, focusing on being present and enjoying small pleasures in their home environment. 6 It is important for PwESD to remain socially active and experience personal dignity, based on being valued by those around them. 22 This is consistent with our findings, which showed that PwESD’s participation in social activities and the frequency of visiting relatives/friends did not change significantly after 1 year. Contact with close people who knew them when they were healthy and self-sufficient provides PwESD with a sense that they are still considered ‘complete’ beings, making the presence of cognitive impairment less embarrassing. 6 Thus, our findings suggest that PwESD can remain in their home environments and maintain social contact. However, it is noteworthy that worsened cognitive problems may affect how PwESD cope with identity changes 40 and experience personal dignity. 3
Our findings lead us to hypothesise that the association between self-sufficiency in ADLs and autonomy and meaning in life may be related to role limitations and questioning of an individual’s identity (e.g. for women, changing roles from family caregiver to care recipient). 17 We also suggest that perceived pain may threaten the identity of PwESDs by reminding them of their diminishing physical strength, which threatens their purpose in life.
In our study, worsened depression was the only predictor of change in perceived personal dignity in both overall and individual domain scores in PDI-CZ. Depression is a neuropsychiatric symptom present in more than half of PwESD living in the community. 41 The relationship between dignity and depression is supported by cross-sectional studies focusing on PwESD living in the community 17 and outpatients of cancer. 42 Depression as a predictor of 1-month change in the PDI-CZ’s purpose of life domain was confirmed in a Czech study of older people who were hospitalised. 43 Depression negatively affects self-esteem. As personal dignity includes self-esteem and self-identity, 44 it is easy to lose the sense of personal dignity, as a result of depression. Consequently, it becomes difficult to engage in meaningful interactions with others, which are essential for maintaining personal dignity. 3 Conversely, social capital (including social participation and emotional and affective supports from loved ones) protects against the development of depression, 45 allowing PwESD to maintain a sense of personal dignity.
Limitations
This study has some limitations that should be considered when interpreting the results. Only older adults living at home and with early stages of dementia were included in this study. Therefore, the results cannot be generalised to the population with dementia. The study included results after 1 year follow-up, which may not be sufficient to confirm causal relationships. The low overall explained variability of the independent variable (0.3 for the best model) is another limitation of the study. There may also have been a selection bias. People with fewer social contacts and depressive symptoms may not have wanted to take part in the study. Nevertheless, this study is novel in that it provides valuable insights into the dynamics of PwESD’s perceptions of personal dignity over a year and highlights the factors that may influence these dynamics.
Conclusions
Our findings suggest that people with early dementia living at home are generally not at risk of loss of dignity as their cognitive, visual and hearing abilities decline over time. Future research should therefore focus on how the social context influences their perception of their personal dignity.
Recommendations for nursing practice
This study contributes to the understanding of the trajectory of perceived dignity of PwESD living in the home environment. Home care nurses should focus on maintaining and enhancing PwESD’s sense of personal dignity, promoting preparation for the future and long-term support for family members, for example, through dignity therapy. This may have the potential to fill an existing gap in providing holistic care to PwESD by home-based nurses.
Footnotes
Acknowledgements
The authors would like to thank the older adults who participated in this study and generously shared their perceptions of dignity. The authors would also like to acknowledge the cooperation and support of the family caregivers and research nurses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Health of the Czech Republic (Grant No NU20-07-00100).
Ethical statement
Trail registeration
This study was conducted as part of the longitudinal study ‘Changes in the perception of personal dignity over the course of dementia’ (registered in Clinical Trials.gov.; No. NCT04443621).
Data availability statement
The datasets supporting the conclusions of this study are available upon reasonable request from the corresponding author.