
Abstract
Background
Nurses have an essential role in caring for end-of-life patients. Nevertheless, the nurse’s involvement in the passive euthanasia decision-making process is insufficient and lower than expected.
Objectives
To explore factors associated with nurses’ intention to be involved in non-treatment decisions (NTD) regarding passive euthanasia decision-making versus their involvement in the palliative care of patients requesting euthanasia, using the Theory of Planned Behavior (TPB) framework.
Design
A cross-sectional study utilizing a random sample.
Participants and research context
The study was conducted in one of the largest hospitals in Israel among 125 nurses employed in internal and surgical care wards. Data was collected through face-to-face interviews between March and April 2019.
Method
A closed structured questionnaire was developed according to TPB instructions. A paired sample t test and two multiple hierarchical regressions were conducted. Variance explained (R2) and the significance of F change were calculated for each regression. The study used the STROBE statement guideline.
Ethical considerations
The study was approved by the hospital’s Helsinki Committee (#20.11.2017).
Findings
A paired sample t test revealed that nurses’ involvement in the palliative care of patients requesting passive euthanasia was significantly higher than in NTD regarding euthanasia. Regression analyses revealed that nurses’ position and attitudes explain their intention to be involved in decision-making; attitudes and perceived behavioral control explain nurses’ intention to be involved in the care of patients requesting euthanasia.
Conclusions
According to the TPB, nurses’ attitudes explained their intention to participate in decision-making regarding passive euthanasia. It is recommended to enhance open discussion of this complex issue to encourage nurses’ willingness to participate in NTD decision-making regarding euthanasia.
Introduction
Alongside the progress of modern medicine and the increase in life expectancy and in the lifespan in recent decades, the concept of euthanasia has also developed. 1 Patient autonomy to request to end their life under specific medical/health circumstances is central to the concept of euthanasia. 2 Notwithstanding the multiple definitions of euthanasia, most have in common the principle of causing intentional death without pain at the repeated request of a patient with a severe and terminal illness to alleviate his pain and suffering. 2 In most Western countries, the law sanctions a sequence of actions related to euthanasia, beginning from palliative sedation, through passive euthanasia and active euthanasia, to physician-prescribed death. The European Association for Palliative Care 3 defined non-treatment decisions (NTD) as “withholding or withdrawing medical treatment from a person either because of medical futility or at person’s voluntary and competent request” (page 6). The current study used the term NTD as defined by the European Association for Palliative Care for the concept of preventing life-sustaining or life-preserving treatment from patients at the end of life. This definition is consistent with Israeli law in the context of euthanasia. Palliative care is defined by the World Health Organization (WHO) as a patient-oriented approach to improving quality of life, including end-of-life treatment, by relieving suffering and enhancing physical, psychosocial, and spiritual comfort. 3 The current study uses the term palliative care for patients requesting euthanasia in the context of preventing and relieving pain, as well as providing fluids and nutrition, medication and oxygen, and emotional support for the patient and family.
Background
The issue of euthanasia, in its various forms, is described in the literature as one of the most critical and controversial in the current era. 3 Moreover, nursing literature has broadly discussed the complex ethical and moral issues regarding euthanasia and the nurse’s role in euthanasia.4,5 The ethical code of nurses in Israel is directed at facilitating “dignified death,” meaning that nurses must uphold individuals’ right to die with dignity while maintaining their dignity, privacy, and values. 6 This declaration is compatible with nurses’ overall ethical principles of respect for autonomy, beneficence, and justice. 7 Although the authority to approve NTD regarding euthanasia belongs to the physician, there is a consensus that decision-making at the end-of-life is a significant process that requires the involvement of a multi-professional team, including nurses. 8 Nurses, the largest group providing professional care in the health field, are on the frontline of contact with patients and families and encounter requests by patients and families seeking assistance at the end of their life. 9 In many cases, the nurse is also the first professional to whom the patient turns to request euthanasia. 10 These situations are relevant for nurses in a community setting, such as home care and palliative care, nurses in long-term hospital wards, such as care of older persons’ wards and hospices and hospital nurses in intensive care units and general wards. 11 This status gives nurses a significant role at an early stage in the process of euthanasia. 12 Non-treatment decisions (NTD) regarding the euthanasia process may include two phases. The first is decision-making regarding euthanasia, for example, the decision to withhold treatment, which will lead to a hastened death. The second is the treatment phase, for example, palliative care and nursing management of end-of-life patients. 5 Nurses are aware of their essential involvement in the process of patient end-of-life as they are familiar with the patient (and the family), as well as the patient’s values and needs.5,13 The nurse’s role in managing the patients’ end-of-life care is broad, and includes in particular explaining information to the patient and family, mediating between the patient and the physician, and providing physical and emotional support. 14 Nevertheless, studies have shown that nurses’ involvement in the decision-making process is insufficient and lower than expected.13–15 A study conducted among intensive care unit nurses in European countries found that 91.8% were directly involved in the palliative care of patients requesting euthanasia, and 63.6% had a discussion with physicians regarding the patient’s end-of-life. Nonetheless, only 38.2% of the nurses had been asked to participate in decision-making regarding patients’ end-of-life. 16 Similarly, Bloomer et al. found that the discussion between nurses and physicians on this issue involved alerting physicians to the point when medical treatment is futile and end-of-life decisions are needed but nurses were not involved in the decision-making itself. 17
Moreover, countries that legislated euthanasia by law as part of the management of patients’ end-of life mainly determine the physician’s role in the process and lack precise definitions and guidelines for the nurse’s role.18,19 Gallagher et al. indicate the importance of investigating the factors underlying nurses’ willingness to be involved in the euthanasia process, in particular at the decision-making stage. Research on this subject may clarify the strategies required to promote their involvement, help define their role, and allow nurses to lead the process in their country. 20
Euthanasia in Israel
The Dying Patient Act was enacted in Israel in 2006. The law determines who is defined as a “dying patient”: a patient who has an incurable illness, with a life expectancy that does not exceed six months. The law allows physicians to withhold or withdraw medical treatment from a person with a terminal illness but not to stop ongoing treatment. The law forbids withholding palliative treatment, water, and nutrition. Among the Israeli public, this is commonly termed “passive euthanasia.” The Dying Patient Act determines that the patient or his representative can request euthanasia. In 2014 the Israeli parliament discussed a new law that would permit active physician-prescribed euthanasia, but this law has not been enacted to date. 21
The research framework: Theory of planned behavior
The Theory of Planned Behavior (TPB) was developed by Ajzen (1991) 22 and it is one of the most widely implemented theories for understanding individuals’ social behavior. 23 The basis assumption of the TPB is that the essential intention to perform a behavior may predict one’s subjective behavior. Behavioral intention is one’s degree of readiness to act, from which the subjective probability that the person will perform the behavior is derived. 22 The intention to implement a particular behavior is determined by three direct factors: personal attitudes toward the behavior, subjective norms, and perceived behavioral control.
Attitude towards a behavior is the positive or negative assessment of the individual’s behavior performance. Namely, a person who evaluates the performance of a particular behavior positively will hold a favorable position toward that behavior, and vice versa. 24 Subjective norms reflect the social influence on the individual. They are defined as one’s tendency to act according to his perception of the social pressures exerted on him regarding the performance or non-performance of a specific behavior.22,24 Perceived control relates to one’s ability to perform a given behavior. When individuals perceive themselves as having the power to perform a particular behavior, they are more likely to intend to behave thus. According to Ajzen, 22 perceived control may directly predict behavior, and not only through the intention to practice the behavior.
The TPB was found suitable for predicting and understanding the behavior of healthcare professionals, such as physicians and nurses, from various fields of clinical practice. 23 Lee and Kang found that attitudes and perceived control predict nurses’ intention to care for patients with infectious diseases, where perceived control was the strongest predictor. The authors concluded that the TPB is useful for predicting nurses’ intention to perform caring behaviors. 25 A study aimed at predicting hospital nurses’ intention to care for patients with COVID-19 found that attitudes, control beliefs, and perceived behavioral control were significant predictors, where the most robust predictor was perceived behavioral control. The authors concluded that to advance nurses’ intention to provide care, their perceived behavioral control should be bolstered. 26
In light of the literature and the TPB model, the current study aimed to explore factors associated with nurses’ intention to be involved in euthanasia decision-making compared to their involvement in the palliative care of patients requesting euthanasia.
Materials and methods
Research design
A cross-sectional study with a random sample. The study used the STROBE statement guideline.
Participants and research context
The study was conducted in a large hospital (with 1200 beds) in central Israel. From the list of nurses working in internal and surgical care wards, every third nurse was selected and asked to participate in the study, generating a list of 125 nurses. Altogether, 119 nurses agreed, for a response rate of 95.2%. The data was collected through face-to-face interviews during March and April 2019.
The sample size was calculated with G*Power, 27 with the following parameters for hierarchical regression: medium effect size of 0.15, α = 0.05, power = 0.90, two tested steps, and 13 predictors. The minimum calculated sample size was set at 88 participants. For a paired sample t test, the following parameters were inserted into the equation: two tails, medium effect size of 0.30, α = 0.05, and power = 0.90. The minimum calculated sample size for this test was set at 119 participants. Hence, the final sample size, with 119 participants, was satisfactory.
Measurements
A closed structured questionnaire was used. The questionnaire opened with a short explanation of the definition of NTD regarding euthanasia under Israeli law and the definition of palliative care for patients requesting euthanasia. The questionnaire included five sub-questionnaires as follows:
Personal information
Including gender, age, ethnicity (Jewish/Arab), religiosity, length of experience in nursing, level of education (registered nurse/academic BA or MA), internal/surgical ward, and position in the ward (staff nurse/clinical preceptor/management role). Participants were asked three yes/no questions about whether they had been involved in treating patients and families in the passive euthanasia process, involvement in passive euthanasia decision-making, and whether a patient or family had approached them with a request for euthanasia.
Theory of planned behavior questionnaires
These sub-questionnaires were developed according to Ajzen’s instructions 28 and were designated for the study’s aims and the behavior of interest. Two identical questionnaires were designed, one for nurses’ intention to be involved in decision-making regarding euthanasia and the second for nurses’ intention to be involved in the palliative care of patients requesting euthanasia.
Attitudes
This questionnaire included items examining nine attitudes regarding nurses’ involvement in euthanasia decision-making and nine regarding the palliative care of patients requesting euthanasia, both on a 6-point bipolar scale. For example, replies to the item “Your involvement in decision-making regarding euthanasia is” were ranked from unimportant (1) to significant (6) and replies to the item “Your involvement in the palliative care of patients requesting euthanasia is” were ranked from unimportant (1) to significant (6). Participants were asked to note the score that best describes their attitude. Mean scores were calculated, where a higher score reflected a more positive attitude. Cronbach’s alpha for the decision-making questionnaire was 0.9, and for patient care 0.86.
Subjective norm
This questionnaire included seven items regarding subjective norms as conveyed by colleagues and patients, for example, other nurses, physicians, or nurse management, as well as patients and families. The generic question was “To what extent do you tend to behave according to the expectations of the following people regarding your involvement in the decision-making process on euthanasia/the palliative care of patients requesting euthanasia.” Answers were provided on a 6-point Likert scale ranging from 1- “not at all” to 6- “absolutely.” Mean scores were calculated, where a higher score reflected a higher tendency to behave as expected. Cronbach’s alpha for the decision-making questionnaire was 0.9, and for patient care, 0.91.
Perceived behavioral control
Three items measured this dimension. For example, “When you want to, to what extent can you be involved in the decision-making process regarding euthanasia/the palliative care of patients requesting euthanasia.” Answers were provided on a 6-point Likert scale ranging from 1- “not at all” to 6- “absolutely.” Mean scores were calculated, where a higher score reflected higher perceived behavioral control. Cronbach’s alpha for the decision-making questionnaire was 0.93, and for patient care, 0.87.
Intention of behavior
Intention to be involved in the decision-making process regarding euthanasia or in the palliative care of patients requesting euthanasia was measured by three items each. For example, “You intend to take action to be involved in the decision-making process regarding euthanasia/the palliative care of patients requesting euthanasia.” Answers were provided on a 6-point Likert scale ranging from 1- “strongly disagree” to 6- “strongly agree.” Mean scores were calculated, where a higher score reflected higher intention to be involved. Cronbach’s alpha for the decision-making questionnaire was 0.98, and for patient care, 0.96.
The questionnaire underwent validation by a panel of three experts, including a psychologist and two senior practitioners in palliative nursing and public health nursing. Each expert reviewed the questionnaire, followed by a collaborative meeting with the research team. After extensive discussions, revisions were made to the questionnaire items until reaching a unanimous consensus.
Data analysis
Descriptive statistics were used to describe the participants’ characteristics. Normality distribution was examined by skewness and kurtosis parameters suggested normal distribution (skewness = ±1, kurtosis = ±3). The three questions examining participants’ prior experience with euthanasia were recoded through sum command, meaning that each participant could be ranged from 0 = no previous experience with euthanasia to 3 = had previous experience with euthanasia, in all three questions.
A paired sample t test was conducted to assess the differences within the subjects between the TPB’s variables on the nurse’s intention to be involved in the euthanasia decision-making process and the nurse’s intention to be involved in the palliative care of patients requesting euthanasia. Cohen’s d for effect size was calculated for each pairwise variable’s differences. To diminish statistical error I, the Bonferroni correction for pairwise comparisons was calculated. 29 The equation is α/n with n = 5 variables and α = 0.05. Therefore, the statistical significance received for each paired variable was two-tailed, p ≤ .01.
Finally, two-step multiple hierarchical regression were conducted to assess the explanatory variables for the dependent variable: the nurse’s intention to be involved in the euthanasia decision-making process and the nurse’s intention to be involved in the palliative care of patients requesting euthanasia. Personal details, except age and education level, were inserted in the first step. Pearson correlation found a high correlation between age and professional length of experience (r = 0.82, p < .001), suggesting multicollinearity. Hence, only professional length of experience was inserted into the regression. Also, 92.4% of the participants had an academic education. Therefore, this variable was withdrawn from the regression equation. Attitudes, subjective norms (with two dimensions: professional and patient/families), and perceived behavioral control were inserted in the second step. The highest variance inflation factor (VIF) was 1.6, and the highest correlation between the variables was 0.6, suggesting no multicollinearity. Normal probability plots were used indicated no homoscedasticity. The Dubrin–Watson test was calculated to check the independent error, with a value of 2.27 for decision-making regression and 2.23 for patient palliative care regression, suggesting independence between the residual values of the explanatory variables. 29 Variance explained (R2) and the significance of F change were calculated for each regression. Data analysis was performed using the SPSS package software version 28.
Ethical considerations
The study was approved by the hospital’s Helsinki Committee, with the participants’ informed consent exemption (#20.11.2017). Each participant was given a written explanation of the study and an oral explanation by the interviewing researcher. Anonymity was guaranteed, and the participants could withdraw from participation without incurring any harm. Moreover, the participants were assured that the research findings would be used for scientific purposes only, without revealing their identifying details.
Results
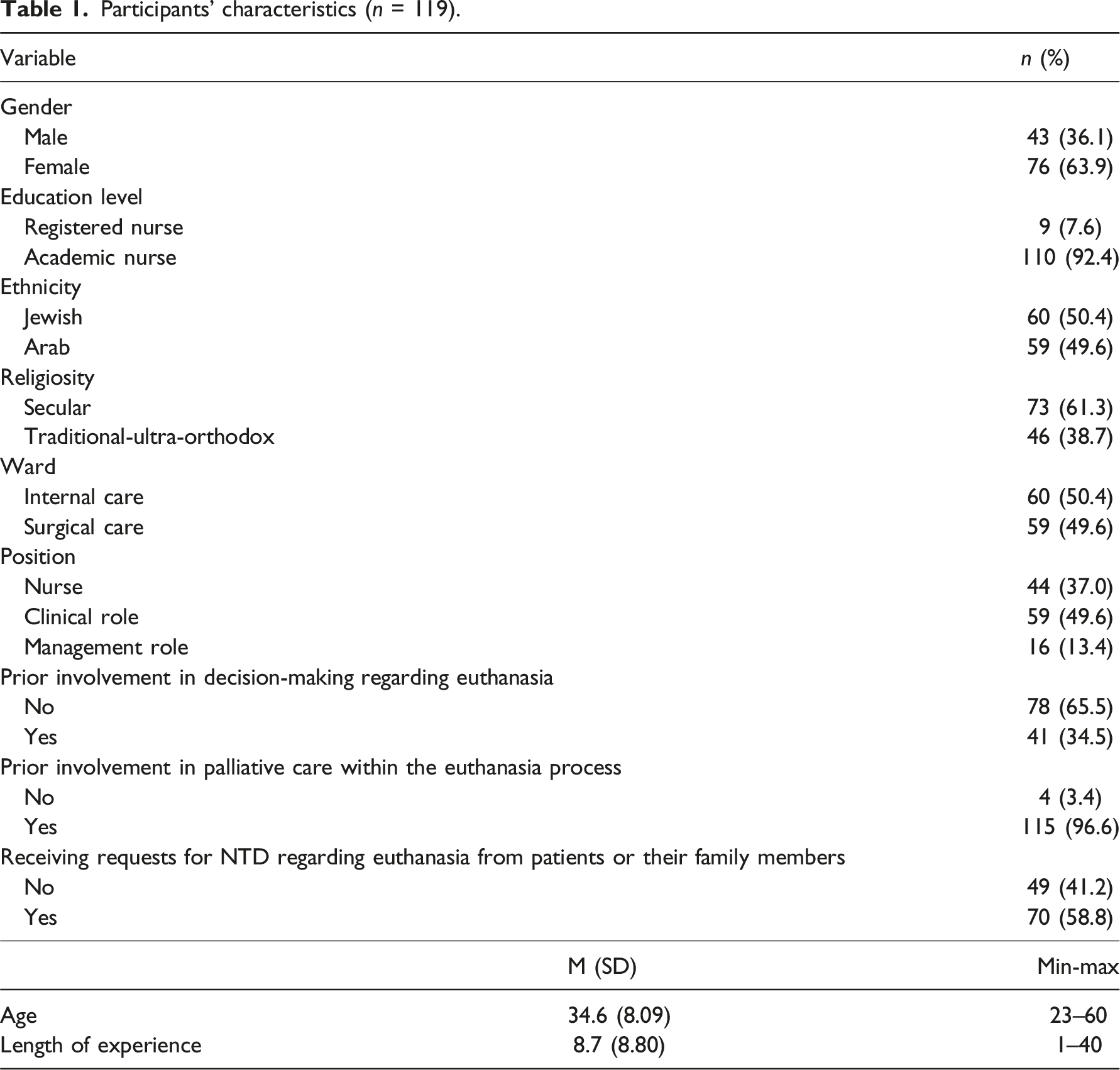
Participants’ characteristics (n = 119).
Comparison of the TPB variables between involvement in patient palliative care and decision-making regarding euthanasia (paired sample t test with Cohen’s d effect size).
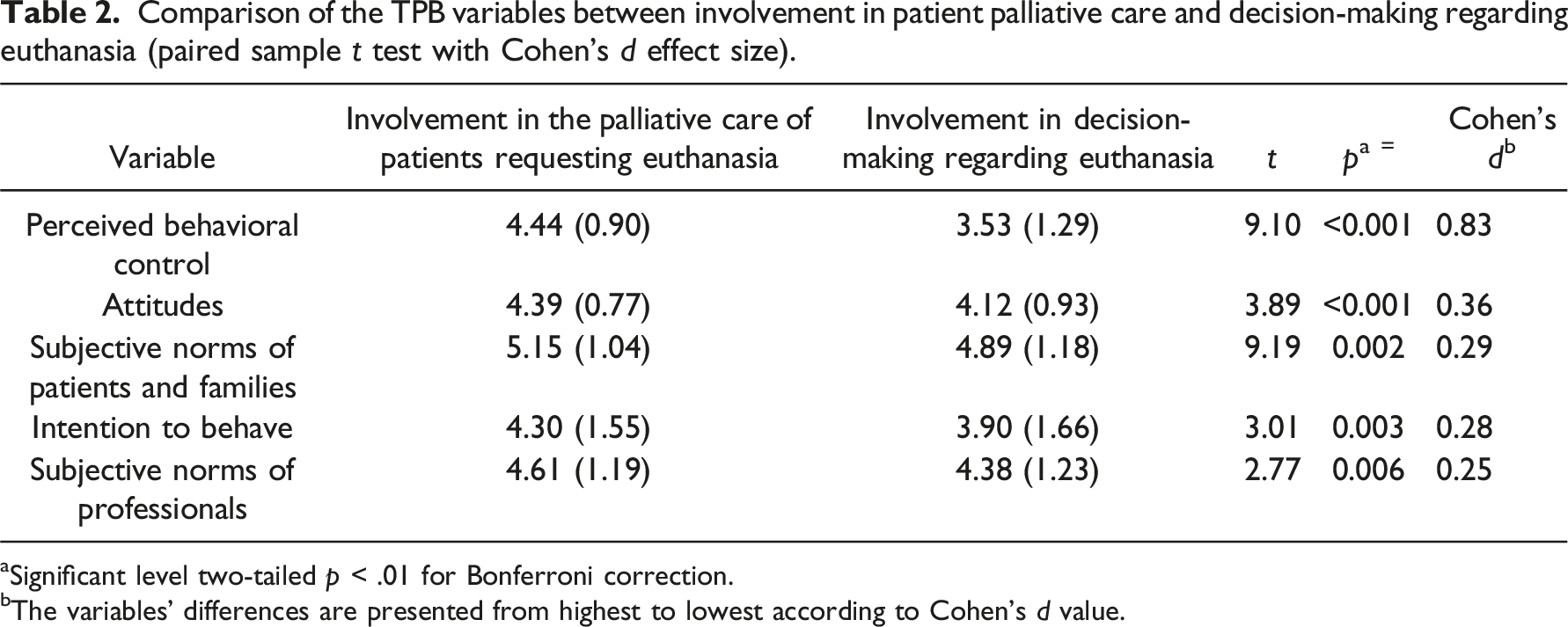
aSignificant level two-tailed p < .01 for Bonferroni correction.
bThe variables’ differences are presented from highest to lowest according to Cohen’s d value.
Linear hierarchical regressions for explaining intention to act regarding nurses’ involvement in decision-making on euthanasia and nurses’ involvement in the palliative care of patients requesting euthanasia.
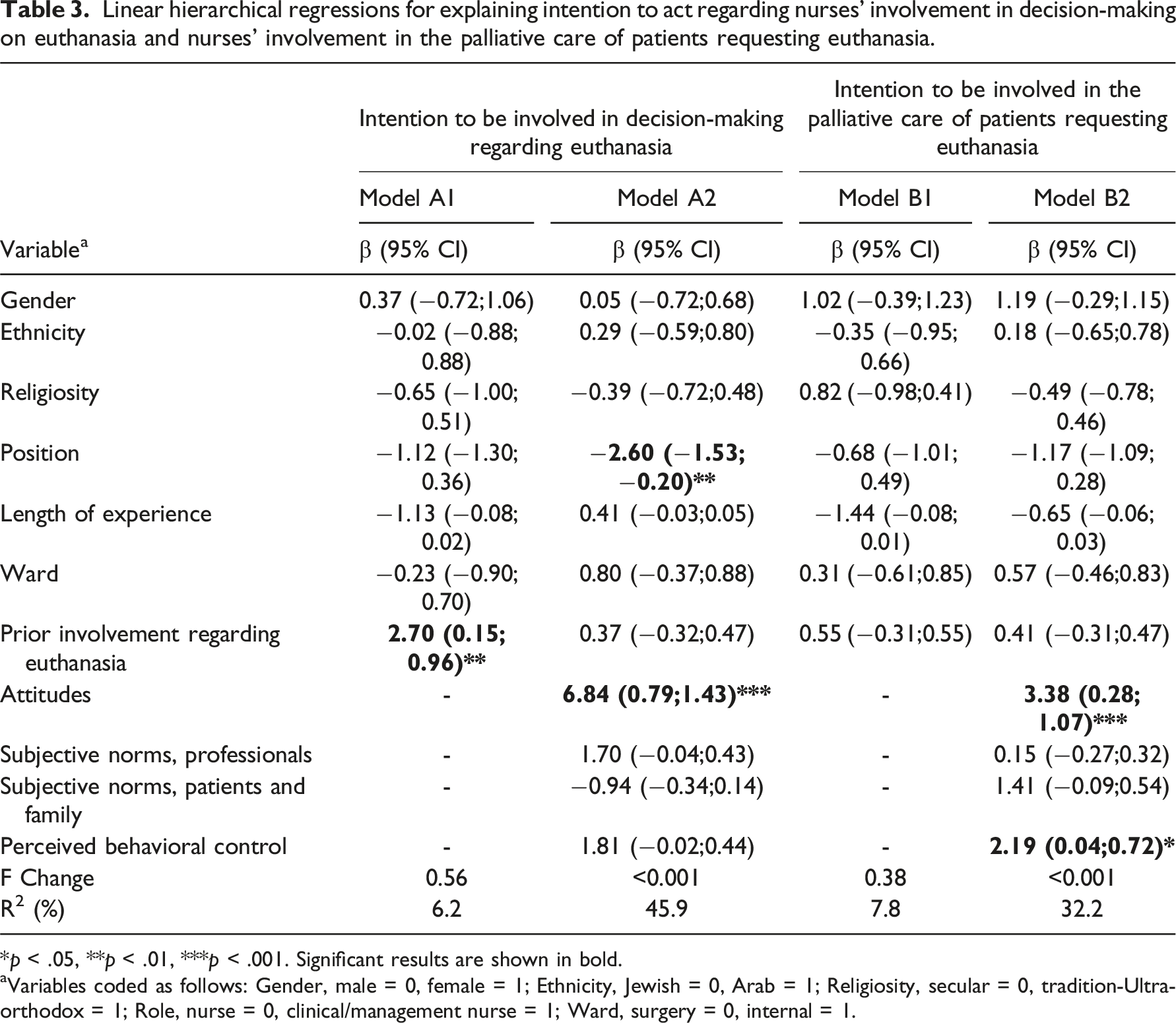
*p < .05, **p < .01, ***p < .001. Significant results are shown in bold.
aVariables coded as follows: Gender, male = 0, female = 1; Ethnicity, Jewish = 0, Arab = 1; Religiosity, secular = 0, tradition-Ultra-orthodox = 1; Role, nurse = 0, clinical/management nurse = 1; Ward, surgery = 0, internal = 1.
The second multiple hierarchal linear regression was conducted to define factors explaining the intention to be involved in the palliative care of patients requesting euthanasia (Table 3, model B1-B2). The regression revealed that only attitudes and perceived behavioral control may explain nurses’ intention to be involved in the palliative care of patients requesting euthanasia (β = 3.38, 95% CI 0.28; 1.07, β = 2.19, 95% CI 0.04; 0.72, respectively). Namely, nurses with more positive attitudes and perceived behavioral control had a greater intention of being involved in the care of patients requesting euthanasia. The model was statistically significant (p < .001), and the R2 was 32.2%.
Discussion
The current study explored factors related to nurses’ intention to be involved in decision-making regarding euthanasia and in the palliative care of patients requesting euthanasia, using the TPB with the variables of attitudes, subjective norms (professional and patient), and perceived behavioral control. The study found that nurses have a higher intention of being involved in the palliative care of patients requesting euthanasia compared to their involvement in decision-making regarding euthanasia. The literature shows an overwhelming consensus regarding the importance of the nurse’s role in the euthanasia process.10,30 Decision-making is a familiar practice among nurses. In nurses’ day-to-day work, they are obliged to reach decisions related to the clinical and psychological needs of patients and their families. The decision-making process is complex and multilateral. Two types of decision-making have been defined: analytical decision-making and intuitive decision-making. 31 The analytical decision-making process is based on integration between evidence-based knowledge and practice. Nevertheless, decision-making based on the nurse’s intuition and experience was found to be more easily and frequently used by nurses although it does not improve the accuracy of the decision-making. 31 Accordingly, decision-making regarding euthanasia is analytical decision-making requiring extensive evidence-based professional knowledge, a deep understanding of the patient and family, 32 and moral competence. 7
Nurse leaders have called upon nurses to be more active in clinical decision-making, rather than focused on caring for patients in silence, 33 particularly in times of health crises and complex moral and social situations. 34 Haahr et al. found that nurses feel inferior to physicians in ethical or moral dilemmas due to the physician’s formal legislative backing. Therefore, nurses are compelled to be less involved in the decision-making process, although they wish to be seen as equal collaborators with physicians. 7 There is a variance in the level of nurses’ involvement in the euthanasia process between different countries according to the laws and regulations in each country, and there is a variance within each country depending on the work environment, the relationship with the physicians, the range of treatment protocols, and the nurse’s involvement in the day-to-day life of the patient requesting euthanasia. 32 A study in the Netherlands found that 24% of general nurses reported being involved in euthanasia decisions with physicians but 69% thought that they should be involved. Moreover, being employed in an academic or general hospital or in a nursing home, having experience in provided care to terminally ill patients, and working within a specialized palliative care team were correlated with active participation in decisions related to euthanasia. 35 In a recent meta-synthesis article, the authors found that nurses used moral explanations for their participation or inability to participate both in decision-making and in assisting dying, such as cultural background and their own beliefs and doctrines. 36 A recent scoping review reported that nurses perceived their role as ensuring a high quality of care to patients receiving euthanasia. 32 Accordingly, the findings in the current study indicate that nurses perceive the palliative care of patients requesting euthanasia as part of their professional role, where they can provide high quality care, support, and advocate for patients and families during the end-of-life process.
The current study found that nurses’ position and attitudes may explain their intention to be involved in decision-making. Accordingly, nurses with no clinical or management position and nurses with more positive attitudes regarding involvement in euthanasia have a higher intention of being involved in decision-making regarding euthanasia. Attitudes were also positively associated with nurses’ intention to be involved in the palliative care of patients requesting euthanasia. An integrative literature review found that nurses’ experience contributed to their professional confidence, which may impact their decision-making process when caring for acute care patients. 31 A study in Spain found that the newer the nurse, the more positive their attitudes toward euthanasia. 37 Nonetheless, this study did not examine the position of the nurses or their attitudes to involvement in euthanasia. In general, it may be assumed that nurses who hold a clinical or management position have more experience and confidence in patient management. Ortega-Galan et al. described the “paradoxical position of nurses,” 37 whereby the new generation of nurses is giving more weight to patient autonomy and freedom from pain and suffering than to merely preserving life.19,37 Bellon et al. reported that nurses with higher levels of education and less experience generally held more positive views towards participating in the euthanasia process. 32 Nursing managers with more experience may be more careful and realize the complex demands involved in decision-making, nurses’ work overload, the organizational culture regarding euthanasia, 31 and that it involves greater responsibility than they are willing to assume. 38 This may result in withdrawal from involvement in decision-making regarding euthanasia.
Ajzen (1991) argued that people tend to be consistent and to behave according to their attitudes. A positive attitude towards a specific behavior will be expressed in a positive intention to perform this behavior. 22 A study performed in six hospitals in Israel examined the association between attitudes and active/NTD regarding euthanasia among neonatal intensive care nurses. The study revealed that strongly positive attitudes regarding euthanasia were correlated with the nurse’s intention to practice this behavior. The attitudes explained 61% of the variance in intention to practice the behavior. 39 This finding was supported by several studies examining the TPB and nurses’ behavior.40,41 The current study is compatible with these previous studies, indicating that the more positive nurses’ attitudes towards involvement in euthanasia, the higher their intention to be involved in decision-making and in caring for patients requesting euthanasia.
The current study found that perceived behavioral control may explain nurses’ intention to be involved in palliative care for patients requesting euthanasia but not in decision-making. Previous studies that examined the TPB in the context of nurses’ intention to display actual behavior found a positive association between perceived behavioral control and intention to behave or actual behavior.42,43 Involvement in the care of patients, including the terminally ill, is a well-defined and recognized part of the nursing practice 14 and is seen by nurses as including the implementation of medical decisions, 44 implementing patients’ wishes, 4 and supporting patients with ending their life in dignity. 19 Generally, nurses have high professional confidence in caring for patients, leading to high perceived control of the situation, of patients’ pain, and of relieving suffering. 19 Moreover, one study suggested that when nurses believe that there is a low need for their involvement, their perceived behavioral control has less of an impact on their behavior. 45 Some nurses felt powerless to be involved in euthanasia 46 as a result of a lack of legal backing for nurses compared to physicians, low ethical competence in euthanasia, and various organizational reasons such as workload, lack of procedures, and others.7,32 Considering the literature, in the context of the current study it may be assumed that nurses feel more confident taking care of patients requesting euthanasia than being involved in decision-making and perceived themselves as less essential for the decision-making process. This may be associated with Israel’s Dying Patient Act, which defines only the physician’s role in decisions regarding euthanasia. 21 These issues are beyond the scope of the current study, and they should be examined in further research.
The current study has several limitations. First, the study was conducted among nurses from a single hospital. Although it is a big hospital, extending the study to other hospitals is recommended. In addition, in complex and moral issues such as euthanasia, there could be a disparity between the intention to behave and actual behavior. Hence, behavioral intention is not necessarily indicative of the final behavior. Finally, other variables that may impact the issue of euthanasia, such as nurses’ autonomy, were not examined in the current study. It is recommended to expand the scope of further studies.
Conclusion
According to the TPB, nurses had higher attitudes, control, and subjective norms in their intention to be involved in the palliative care of patients requesting euthanasia than involvement in decision-making NTD. Nurses’ attitudes and position in the ward may explain their intention to be involved in decision-making regarding euthanasia. Attitudes and perceived behavioral control may explain nurses’ intention to be involved in the care of patients requesting euthanasia.
Nurses have an essential role in caring for end-of-life patients. In the current era, when nurses have extensive professional knowledge, operate sophisticated medical equipment, and deal with complex therapeutic issues, they should also be partners and involved in decision-making processes related to NTD regarding euthanasia. It is necessary to develop their professional confidence to deal with these challenging issues and, first and foremost, to train nurses with clinical and management positions to serve as role models for novice nurses. It is recommended that an open discussion be held with nurses regarding attitudes related to their involvement in reaching decisions about euthanasia and in the care of patients requesting euthanasia. Nurses’ attitudes and desire regarding the extent of their participation in euthanasia must be respected. Encouraging professional discourse on the subject may develop professional skills, strengthen nurses’ professional confidence, and encourage them to take part in reaching decisions regarding euthanasia.
Footnotes
Acknowledgments
The authors thank Professor Yoram Bar Tal for his dedicated and precise guidance.
Author contributions
All authors contributed to the study’s conception and design. Ronit Tsemach and Anat Amit Aharon performed material preparation, data collection, and analysis. Anat Amit Aharon wrote the first draft of the manuscript, and all authors commented on previous versions. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.