
Abstract
Background
Moral distress is a far-reaching problem for nurses in different settings as it threatens their health.
Aim
This study examined which situations lead to moral distress in home-care nursing, how and with which consequences home-care nurses experience moral distress, and how they cope with morally stressful situations and the resulting moral distress.
Research design
A qualitative interview study with reflexive thematic analysis was used.
Participants and research context
We conducted semi-structured interviews with 20 home-care nurses in Germany.
Ethical considerations
The study was approved by the Data Protection Office and Ethics Committee of the German Federal Institute for Occupational Safety and Health.
Findings
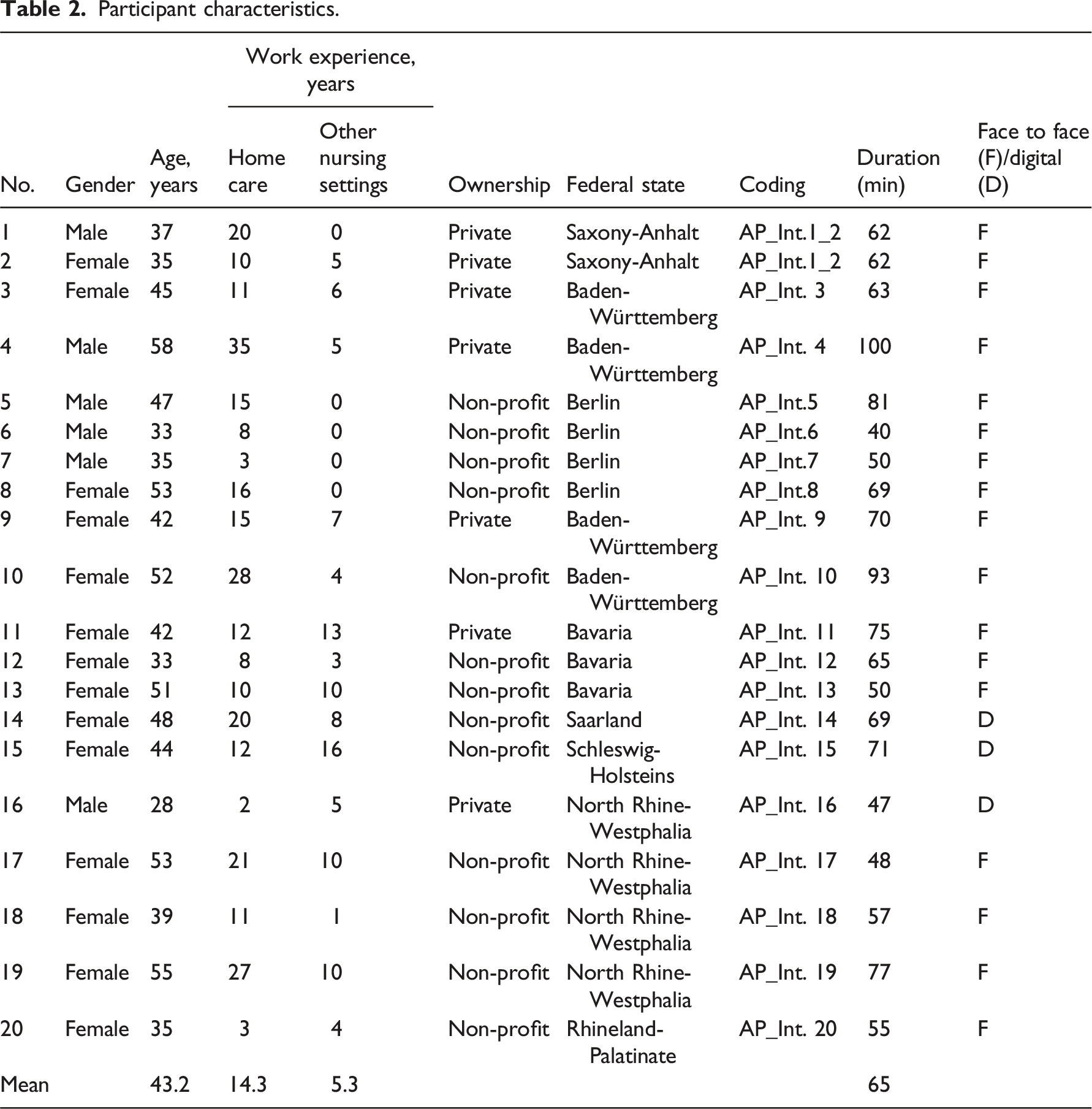
Twenty (14 female and 6 male) home-care nurses were interviewed between April and August 2023 at their chosen location. The situations leading to moral distress were inadequate care of the person in need of care, not being able to protect one’s health, extended responsibility for the entire care arrangement, work–privacy conflicts, and conflicts between the understanding of care or professional ethics and the performance and billing system. The nurses experienced moral distress as they worked alone and provided care in the patient’s territory. Short- and long-term strains with destructive cognitions, negative emotions, physical symptoms, and health consequences were reported. They faced challenges in coping with moral distress on institutional and individual levels.
Conclusions
In cases of tension between the service and billing system and the understanding of these nurses’ care services, moral distress is unavoidable. Alternative forms of organization and billing modalities, such as payment by time and the expansion and refinancing of service, should be implemented. The latter relates to systematic case and ethics meetings. Further, a transfer of medical activities, such as the prescription of wound material to registered nurses, could prevent morally stressful situations and improve patients’ quality of care.
Introduction
Moral distress threatens patient care quality, health professionals’ well-being, and the whole organization, 1 making it a significant problem for health care. 2 Owing to their position in decision-making hierarchies, nurses are particularly affected by moral distress. 3 In 1984, Jameton defined moral distress as “when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action.” 4 This suggests institutional constraints as a necessary condition for moral distress. Other morally relevant events of suffering were overlooked or neglected. Therefore, the definition of moral distress was recently broadened.5,6 Fourie 6 recently proposed moral-uncertainty distress, which is when a nurse is unsure about the morally right action. Morley et al. 7 introduced with empirical evidence a further segmentation in moral tension, uncertainty, constraint, conflict, and dilemmas.7,8 We therefore apply the definition of moral distress as “psychological response to morally challenging situations.” 5
The prevalence of moral distress depends on the care setting, instrument used to measure moral distress, and the country.9,10 The relevant literature mainly focuses on nurses in clinical settings.2,11,12 Although some studies show that home-care nurses also undergo and suffer from moral distress, 13 analyses of home-care-specific situations that lead to moral distress apart from general ethical problems are lacking. 14 Consequences like burnout and intention to leave one’s current position, 13 and the worldwide growth of home-care nursing 15 highlight the need for prevention of moral distress. Therefore, this study examined moral distress specifically in home-care settings.
Home-care (nursing) in Germany
In Germany, home-care services (HCS) support people in need of care and their relatives in all areas of daily living (e.g., nutrition, personal hygiene, exercise). The need for care affects not only older individuals, but also children with disabilities or adults with chronic illnesses. 16 In the German home care system, certain medical-related tasks, such as administering medication or injections, are prescribed by the family doctor and financed by the statutory health insurance, while other services are covered by long-term care insurance. Those in need of care choose a HCS with which they conclude a care contract for the services to be provided. There are private, non-profit, and municipal HCS. Expert raters of the statutory health insurance assess the level of care dependency (low to severe). Depending on this level, a certain budget is available to the person in need of care; if the costs exceed the selected services, they must be paid for themselves. If family members take on care activities, they can receive care money from this budget.
Aim
This study examined (a) which situations lead to moral distress in home-care nursing, (b) how and with which consequences home-care nurses experience moral distress, and (c) how these nurses cope with morally stressful situations and the resulting moral distress.
Methods
Data collection
The first author collected data from April to August 2023. Following Kallio et al. 17 the semi-structured interview process included a peer review of colleagues of the “Designing Service Work” unit of the German Federal Institute of Occupational Safety and Health, an expert review, and a pretest in the target group (Online_Supplement_1).
Sixteen of the 20 interviews were conducted face-to-face at a quiet location of the participant’s choosing such as the HCS or a café. Three interviews were held via videoconference, according to the participants’ wish or for organizational reasons. The interviews began with a reminder of the study aim and a brief definition of moral distress. The situations in which moral distress was experienced were understood as critical events. Based on these situations, accompanying feelings, thoughts, support options, and consequences were elicited to answer the research questions. In the last two interviews, the nurses did not raise new situations of moral distress or other issues, indicating data saturation. 18
Participants and research context
Inclusion criteria for participation were (a) employment in a HCS with social insurance, (b) completion of professional nursing education training (3-years), (c) minimum age of 18 years, and (d) at least one year home-care work experience. Home-care nurses from HCS of different sponsors (non-profit/private/municipal) and different German federal states were interviewed to minimize selection bias due to the structural working conditions of the HCS. Hence, a list of randomly selected HCS per state was compiled, the managers of which were contacted by email for distributing the invitation to employees (Online_Supplement_2). Nurses received €50 in appreciation of their time.
Research design
This descriptive study with thematic analysis used the critical incident technique (CIT) to collect data.19,20 This method originates from the field of air traffic control, making it particularly solutions-oriented. Home-care nurses were asked to describe a critical situation—a real-life experienced situation with a clear beginning and end that is particularly important to them. 17 Participants described the circumstances, including the (a) situation that led to the incident, (b) actions or behaviors of the focal person in the incident, and (c) results or outcomes of the behavioral actions. CIT is particularly appropriate for discussing morally stressful situations in home-care nursing and the manners of coping with them because it is solutions- or option design-oriented 21 and thus, could help in formulating recommendations for work improvement by reducing moral distress. To gain a deeper understanding of the situations, CIT was complemented by the reflective cycle according to Gibbs and Unit. 22 Specifically, questions about emotions, cognitions, and the situation’s appraisal were designed to guide nurses to think more deeply about their experiences. This generated a more precise situation description and insightful information about the nurses’ experience and morally relevant features of the situation. CIT’s application in the health and nursing sciences has proven to be purposeful21,23 and been applied for analyses regarding moral distress. 24
Data analysis
Steps of data analysis.
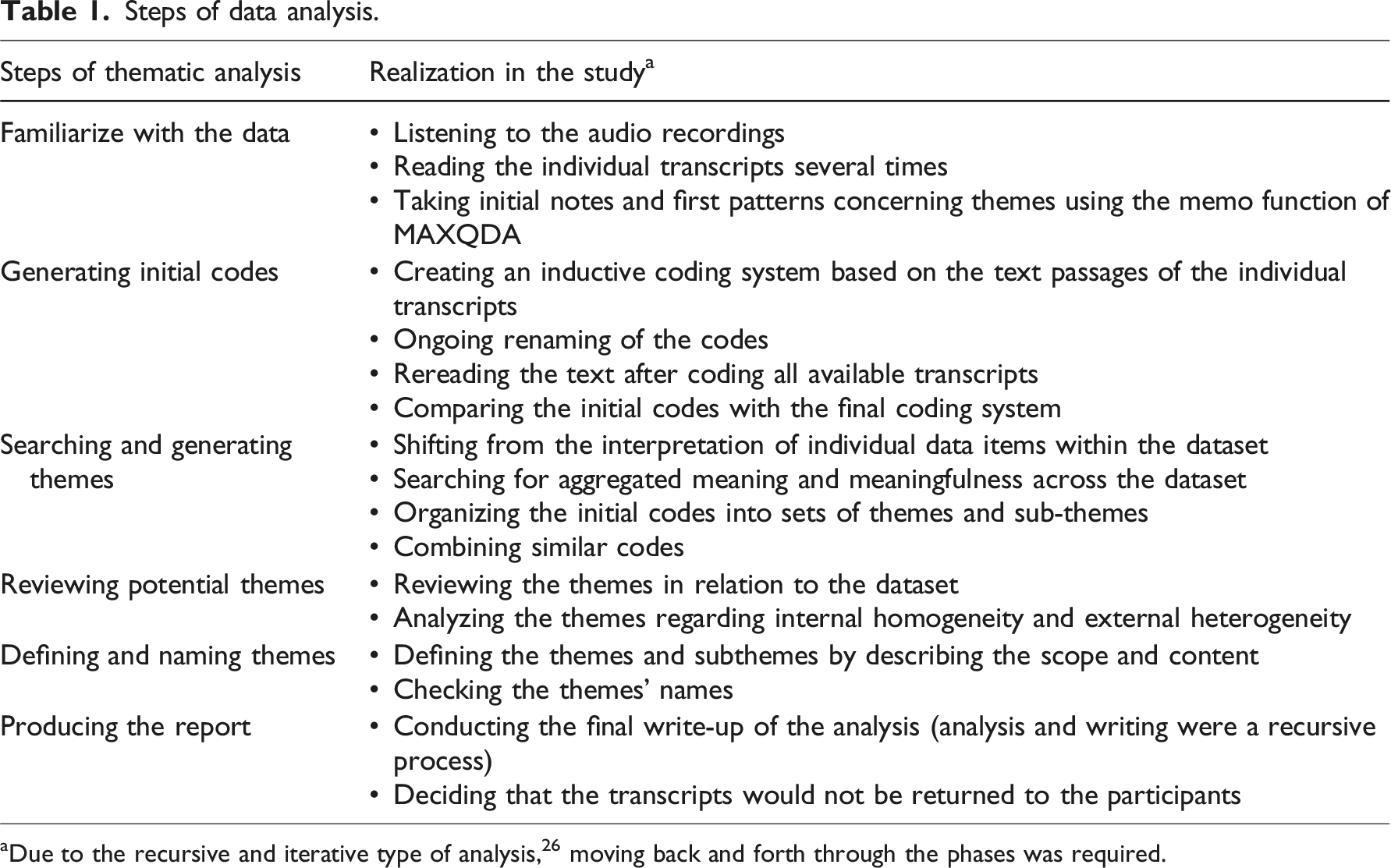
aDue to the recursive and iterative type of analysis, 26 moving back and forth through the phases was required.
Rigor and trustworthiness
For a comprehensible analysis, we applied the quality criteria of confirmability, credibility, dependability, and transferability from Guba and Lincoln. 28 To reach confirmability, two authors discussed the coding and refining process constantly and validated the theme structure with all authors to gain consent.
Credibility was addressed by involving home-care nurses from 15 different HCS in eight federal states. The research process was planned systematically to enhance reliability. Several researchers of the project team also took part in the data analysis and interpretation. To ensure transferability, participant characteristics and the study design were explained in detail.
Ethical considerations
The Data Protection Office and the Ethics Committee of the German Federal Institute for Occupational Safety and Health approved the study design (BAuA: No. 062_2023). The team of authors first informed participants in detail about the study’s aims and procedures, and they voluntarily agreed to participate by signing a written informed consent sheet. According to the data protection concept, participant data were kept confidential such that the interview statements could not be traced to the participant. A psychologist was available for in-depth discussions.
Results
Participant characteristics.
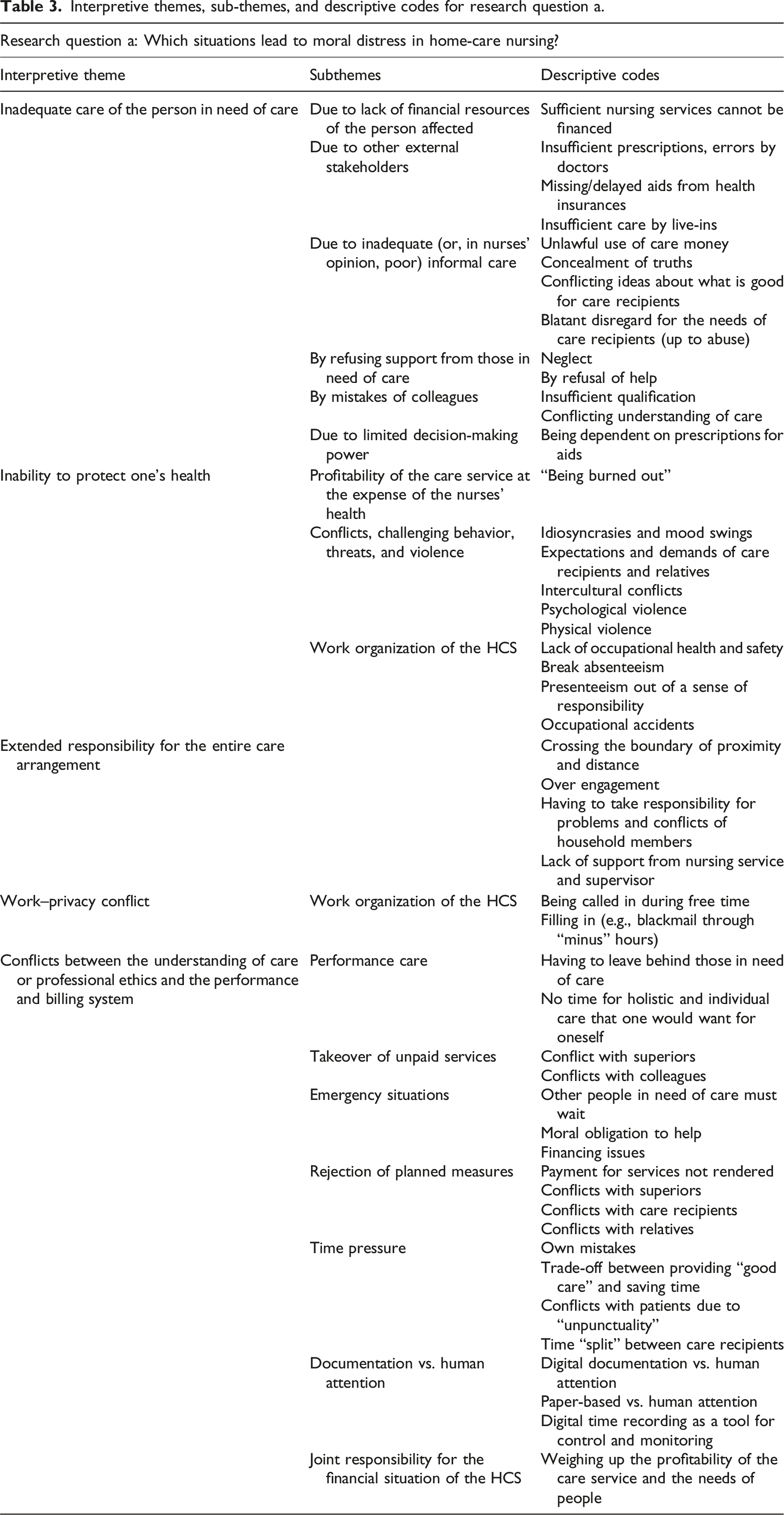
Interpretive themes, sub-themes, and descriptive codes for research question a.
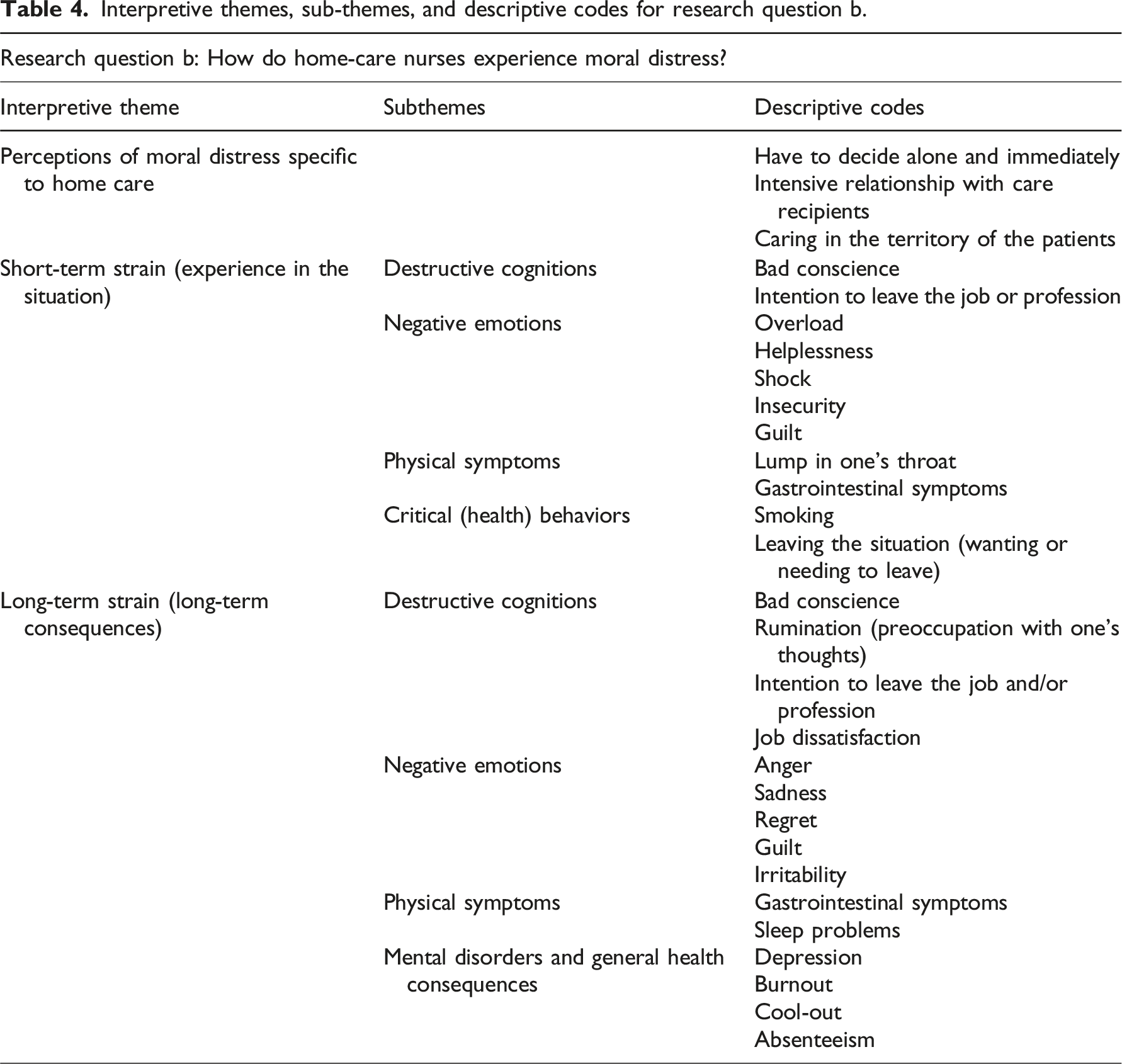
Interpretive themes, sub-themes, and descriptive codes for research question b.
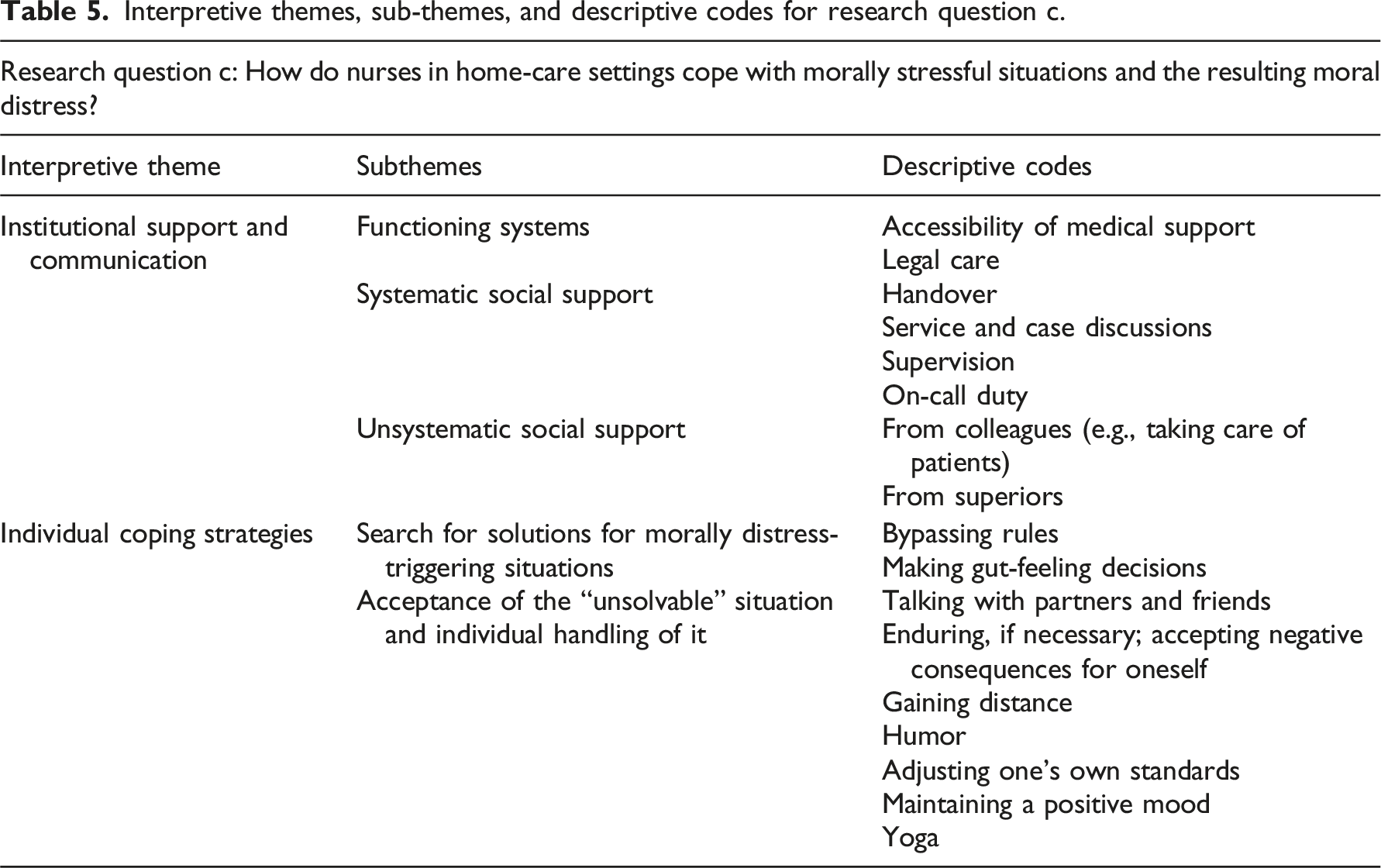
Interpretive themes, sub-themes, and descriptive codes for research question c.
Situations leading to moral distress
Inadequate care of the person in need of care
Theme one, inadequate care of the person in need of care, had several subthemes which specify the causes of the inadequate supply (e.g., lacking financial resources, failure of external stakeholders or informal caregivers, refusion of care). The core issue is that the patient is not being cared for in the manner the nurse envisions, resulting in suffering.
Lack of financial resources
Participants discussed many situations of poor patient care as sources of moral distress, arising from the patients’ or their relatives’ service cost financing difficulties. I see she is simply unwashed, but has booked only medication. Then you leave feeling nauseous and with a little abdominal pain and a bad feeling. Because many older patients cannot afford so much care. (AP_Int.12)
1
External stakeholders
Delayed or inappropriate treatment from external stakeholders (doctors, health insurance providers, or live-ins) also led to poor patient care, with missing prescriptions undermining the patient’s well-being and leaving nurses unable to determine how to improve the situation. The doctor prescribes wound management, which is not suitable at all, where I know from the beginning that the wound will get worse. I find THAT violent, ne? (AP_Int.19)
Informal caregivers
Besides the participants, family members also supported the patients, which caused conflicts and moral distress when the participants disapproved of the care by family. Recognizing that care duties were not fulfilled although family members gained care money was also morally stressful for the participants. Furthermore, some participants reported informal caregivers’ neglect of those in need of care, up to and including physical abuse. I said, “He is in a lot of pain.” […] “I CAN'T move your father in bed anymore without him crying out or making a face.” Say I: “That is a CLEAR sign to me, he is suffering. We can’t work like this anymore.” – “Yes, then you don’t need to come at all.” (.) And then I sat in the car and cried for a while. (AP_Int.12)
Often, the abuse or violence toward the person in need of care cannot be clearly proven, for example, because of dementia, making nurses feel overloaded and helpless. She said that the son would SLAUGHTER her. The son came into the room, he […] said, “I didn’t SLAUGHTER you. That was a slap.” Then it went back and forth. The woman had severe dementia. Then you doubt yourself; is it true, is it NOT? […] Then we are obliged to involve the health department. […] He said: “Well, that’s what you get for that. The health department is coming to get you. You’re going straight to a home,” And then I’m standing there: (breathing in shock) I didn't want that either. I just wanted her to be well. And there one stands, really, one has totally bad conscience, I find, totally. EVERYTHING you do is wrong. (AP_Int.19)
Refusion of care by people in need of care
In some instances, the patient himself refuses certain care activities, necessitating expert advice. You don’t want to leave him in the URINE. (.) On the other hand, he scolds us and gets angry with us and says: “You, always with your shit washing, I don’t want that shit.” So, and the family says, however, he must look good. (AP_Int.15)
By mistakes of colleagues
That their colleagues understood nursing differently or did not provide care according to professional standards (which could endanger the patient) caused a conflict of loyalties, as the interviewees did not want to blame their colleagues but simultaneously felt responsible and ethically committed to the patients’ well-being.
Due to limited decision-making power
In some situations, the participants were unable to provide patients with sufficient care due to their lack of decision-making authority in the healthcare system, for example, in relation to doctors or other stakeholders (e.g., prescribing medical aids).
Inability to protect one’s health
Theme two addressed situations in which the participants could not protect their health and thus experienced conflicts between the principles of self-care and welfare (e.g., Profitability of the care service at the expense of the nurses’ health, conflicts, challenging behavior, threats, and violence)
Profitability of the care service at the expense of the nurses’ health
They felt exploited by their employer, who prioritized economic goals over their health needs (e.g., condensation of tours). This feeling arose from work organization of the HCS such that nurses felt no breaks were possible because of the dense route planning or their supervisors’ inadequate reaction to accidents at work.
Conflicts, challenging behavior, threats, and violence
They also felt their health being threatened by psychological or physical violence. Further, because of patients’ or their family members’ excessive demands, the nurses’ needs were ignored, leading to moral distress. That the bathtub lift should perhaps stand the other way around for bathing, because she gets back pain in this position […] And the son said that it wouldn’t matter to him if the colleague got back pain or not. He would pay for it. And then he, the son also said: “Mother, you don’t have to praise her. If you don’t scold or don’t complain, that’s praise enough.” (AP_Int.17)
Extended responsibility for the entire care arrangement
The third theme, without subthemes, centered around the responsibility, home-care nurses develop for their patients. The boundary between professional closeness and distance is sometimes difficult to maintain, especially when patients suffer from loneliness and make great demands on the nurses. Some participants often felt obliged to solve problems outside their nursing responsibilities in their free time, thereby causing moral pressure.
Regarding the excessive responsibility for the person in need of care, participants felt left alone by the nursing service and superiors, as they could not understand the situation, the need for action in the households, and the emotional pressure resulting from feeling responsible for the person in care, because they have not experienced it directly.
Work–privacy conflict
Theme four, work–privacy conflict with the subtheme work organization, consisted situations in which participants felt torn between family responsibilities and professional obligations.
Work organization
The major aspect in this theme is the work organization. Thus, work–privacy conflicts, which led to moral distress arose when participants were called in during their free time. The participants had to neglect either their family responsibilities, or their colleagues and patients. “Okay, if I don’t step in now, there’s no one there.” So you always feel responsible in the situation, because you don’t want to let the team down; you don’t WANT to let the patients down. […] Yes, to sacrifice your free time or just to say, “Okay, Mama is now WORKING again,” is just difficult. (AP_Int.20)
Company-related minus hours also generated work–privacy conflicts. In some cases, participants were scheduled by roster writers for fewer hours than their contract specified, to allow flexibility. However, hours were often lost because of admittance of patients as inpatients or cancellation of assignments at short notice, thereby causing pressure to make up the hours.
Conflicts between the understanding of care and the performance and billing system
The last theme, conflicts between the understanding of care and the performance and billing system with the resulting sub-themes (e.g., Performance care, takeover of unpaid services, emergency situations, rejection of planned measures, time pressure, documentation vs. human attention, and joint responsibility for the financial situation of the HCS,) dealt with moral distress which occurred if participants did not feel that the existing system enabled them to provide the care, they believed in.
Performance care
Nursing tasks are prearranged by contract with hardly any freedom in the clocked touring plan to react to current needs; this contradicts the moral principles of nursing. They had the feeling that they didn't even have time and space for a banal greeting: That is now with care, with excretion, time for excretion, a wound dressing, that everything is timed to minutes SO ULTRA tight; […] I don’t even have time, [for] this blanket [greeting], “Good MORNING, have you slept well?” I don't even listen. I am already thinking, “Where are the things? (AP_Int.14)
Emergency situations
Specifically, when emergencies occurred, the participants had to balance the needs of all patients in a tour. They felt the moral obligation to help despite knowing that the subsequent patients must wait.
Takeover of unpaid services
Patients requesting tasks or services that they did not pay for also caused conflict for the participants—between the requirements of the HCS, and the handling of colleagues and the patients’ needs.
Rejection of planned measures
Moreover, patients rejecting measures they previously ordered (e.g., taking a shower) are handled by HCS differently. Sometimes, patients must pay for the service anyway or nurses must convince the patients, and sometimes, the patient’s decision is accepted without requiring payment. Hence, the participants experienced contradictory demands from family members, who insisted on the paid service; supervisors, who feared that the visit would not be paid; and the patient, whose needs changed.
Time pressure
The resulting time pressure of the clocked tour plan can lead to mistakes, missed care, and the challenge to “split” the time between care recipients. Participants experienced moral distress in the decision to provide adequate care or save time for the next patient.
Documentation vs. human attention
Participants also described documentation requirements as high and conflicting with their conviction to spend more time with the patient. Paper-based and digital documentation diverted their focus away from the patient’s needs. They found the digital time recording that accompanied digital care documentation as a control and monitoring tool, which increased the time and justification pressure.
Joint responsibility for the financial situation of the HCS
Nurses’ joint responsibility for the HCS’s financial situation likewise resulted from the billing system. They were involved in their supervisor’s struggle to gain profitability for the HCS. Some nurses with additional leadership tasks had to weigh the HCS’s profitability against the patients’ needs, which they found morally stressful. Some participants even reached their limit and found that they no longer wanted to or could not make such decisions. Exactly, so I then decided for myself that this is no longer good for me. And I didn’t want to have to make any more decisions against patients that simply didn’t pay off (AP_Int.12)
Experience of moral distress
Perceptions of moral distress specific to HC
The first theme regarding research question two dealt with how participants perceive moral distress in HC. They perceive morally stressful situations fundamentally different from inpatient settings because they work alone and thus, oftentimes have to decide spontaneously on the right thing to do. Moreover, because of their intensive relationship with the care recipients, they feel especially responsible and involved in the situation. In HC, the nurse enters the patient’s territory and must adapt to the living environment and the value system. This circumstance brings with it moral questions of a different nature, as demonstrated below. We have to adapt to the PATIENTS. And then of course you try to ADVISE and recommend. But if you then, fall on deaf ears, you have to learn to accept, even […] it is WORSE for him. He has the right to DECIDE. [It] is for me PERSONALLY [it is] always a difficult situation. Because I think to myself, “Yes, you could actually do BETTER.” (AP_Int.20)
Short- and long-term strains
Participants experienced moral distress in HC immediately (short-term strain) and afterward (long-term strain). The leading symptom in both was negative cognitions in terms of bad conscience. Many are lonely or isolated. Then COMES the bad conscience. (AP_Int.3)
Participants also reported negative emotions, physical symptoms, and critical health behavior in connection with morally stressful situations. They felt overloaded, shocked, helpless, and insecure about how to react. Sometimes, thoughts of no longer being able to do the job arose.
Even after work or sometimes weeks, month, or years later, the morally stressful situation still affected participants through mental occupation (rumination): And, of course, I take it home with me from time to time. And then I think about the people and think, “Okay, now they are alone.” (.) There is often family, but sometimes NOT. And then I have this feeling that I would like to go back and look. (AP_Int.15)
Feelings of sadness, anger, or guilt accompanied this mental occupation, leading to sleeping problems and illness. Some participants reported depression or burnout as a consequence of morally stressful situations. And when a patient died, who brought us about 1,000 euros a month through insulin, wounds and basic care, and so the first thought flared up: Oh shit, I now have to bring 1,000 euros back in, (.) and NOT, “Man, now a person has died”; it was [then] clear to me, this is no longer possible. (...) Because human beings' need for HELP ranked first with me ALWAYS. That was my greatest difficulty. And that’s what I yes, I actually got sick of.
Nurses’ coping mechanisms
Institutional support and communication
The first theme of research question three contained three subthemes (Functioning systems, systematic and unsystematic social support) and addressed ways of dealing with moral distress related to the HCS as an institution.
Functioning systems
Maintaining cooperation with other stakeholders in patient care was important for the participants, especially in critical care situations or emergencies. Sometimes, the problem in the care situation could be solved without stressing home-care nurses.
Systematic social support
If the morally stressful situation could not be solved in situ, systematic social support, such as meetings or supervision, was considered a helpful coping strategy.
Unsystematic social support
Social support outside the system, such as those from colleagues or supervisors, enabled the participants to talk about the morally stressful situation and accompanying feelings, thereby generating relief as they reflected upon the resulting pressure and strain. That’s when you need a bit of support from the team, when the team says, “Man, you did everything right. You can’t help it; he could have fallen the day after tomorrow. (AP_Int.18)
Individual coping strategies
The second theme addressed individual coping strategies whereas the subthemes: Searching for solutions and Acceptance of the “unsolvable” situation and individual management of it are specified in more detail.
Searching for solutions
Oftentimes, participants decided out of a gut feeling or bypassed rules that evoked a morally stressful situation by organizing prescriptions or drugs in their free time and making less effort for therapies that they could not support, or found extraordinary solutions to help the patient without official medical aid. The neighbors had called me, that the woman is very unkempt and that the man is always drunk. And then I actually just wanted to (.) make a house call to see. (.) And then the woman had FALLEN one night before and had a laceration on the head; it was also all full of blood. […] And the man was drunk. So I just took the woman in the car and brought her to our short-term care. (.) This was a huge STRESS. (Laughter) I took her with me. (.) Uh, it went very quickly with a court order. [It] could have gone wrong, right? But it went well. (AP_Int.19)
Acceptance of the “unsolvable” situation
Regarding missing options for action, the participants tried to cope with morally stressful situations privately by talking with family members about the strain, distancing themselves through free time, or trying to adjust their own standard to reality, especially the duty to endure such situations. And these are also such situations, which you then simply endure somehow, that it is now going badly, but that it is their decision, (.) that they now WANT it that way. (AP_Int.6)
Discussion
Situations leading to moral distress
This study revealed that the home-care situations that evoked nurses’ moral distress were firstly connected with the patient’s well-being, for example, inadequate care due to a lack of financial possibilities to gain adequate nursing service or refusal of support by patients. Owing to their ethos of caring, which is defined in the Code of Ethics, 29 the nurses felt responsible for the human rights of the patients and their relatives, and for social issues. However, in practice, the HCS is the only stakeholder in the home-care arrangement besides the family members, physicians, and insurance companies. The ethical obligations to which home-care nurses are subject therefore go far beyond the specific tasks assigned and paid for by society and the HCS. This contradiction led to morally stressful situations that caused moral distress to the participants when the situation could not be solved. Büscher 30 also articulated that the tension between formal and informal care and the blurred line between social and nursing services cause conflicts in nurses despite not having management responsibilities. Meanwhile, moral stressors in the clinical setting somehow differ. Clinical nurses have reported the provision of futile care for end-of-life patients, team constraints such as professional hierarchy, and organizational constraints such as conflict within hospital policy as causes of moral distress. 31
The findings show the conditions of the German nursing system as possibly a root cause of morally distressing situations for home-care nurses. Instead of providing holistic and individual care that is congruent with the nurses’ ethical principles, the system requires nurses to fulfill single tasks according to the nursing service–patient contract. The participants faced economic pressure because of the demand to stick to the prescribed time slots. The resulting time pressure led to mistakes that made them feel guilt and the need to decide who needs more attention. The situation is similar in clinics when there is a shortage of staff and a lack of time resources.32,33 Furthermore, home-care nurses with leadership duties must constantly balance the nursing service’s profitability and the patients’ needs, which is in line with Büscher and Krebs. 30 This situation also leads to moral distress.
Moreover, home-care nurses are caught between the care for the patient, the expectations of the HCS, and their own needs and family obligations. The latter finding confirms quantitative results, where work–privacy conflicts were identified as predictors for moral distress in HC. 13 Home-care nurses regularly endanger their own health by disregarding their own needs. However, the nurses’ self-care is a prerequisite for the patient’s care, and their neglect is a relevant source of moral distress. 6
In summary, nurses reported situations in which they felt unable to act because of external rules (e.g., non-observance of the patient’s current needs because of contractual regulations) and those in which they did not know how they should act (rejection of nursing activities that are necessary from a professional viewpoint). This supports the distinction between the concepts of moral-constraint distress and moral-uncertainty distress introduced by Fourie. 6
Experience of moral distress
The experience of moral distress in HC is seemingly unique because of the intensive relationship between nurses and patients or the whole family. As they work alone, they are under pressure to make morally distressing decisions, for example, how to react in emergency cases. At several levels, moral distress appears in the situation in situ and in the long run. This is in line with Jameton. 4 This study’s participants described moral distress with destructive cognition (e.g., the intention to leave the job or even profession), negative emotions (helplessness, shock, anger at the situation, and sadness as long-term consequences), physical symptoms (stomach pain), and health consequences (rumination, absenteeism, burnout, and depression). The bad conscience was specifically emphasized, together with guilt and regret, which was a source of rumination. This long-lasting mental and emotional occupation of the experienced situations that bother the conscience indicates violation of the nurse’s moral integrity, which strikes at the heart of a person’s core values. 34 The lingering portion of moral distress, also referred to as moral residue, not only affects an individual at a personal but also at a professional level. 35 Emotional and psychosocial consequences such as grief were also reported by nurses working in care homes, 9 including symptoms such as helplessness, sadness, and sleeping problems. 36
Nurses’ coping mechanisms
At an institutional level, the participants tried to use existing offers such as team meetings to cope with their moral distress. Team cooperation was also found useful for chief nurses. 37 However, colleagues were the first access point to talk about moral distress. This is in line with the findings of Morley et al. 7 but seems only moderately helpful in solving the problem.
Limitations
Owing to the voluntary participation in the study, it is possible that only home-care nurses who are interested in the research topic responded. One interview was conducted with two persons because of the nurses’ wishes. It is possible that topics were presented in a different way than they would have been in a single interview. Three interviews were conducted via videoconferencing for organizational reasons. This method offers opportunities and risks for qualitative social research. 38 Some home-care nurses had additional leadership tasks. Further research is needed to map out the perspective of chief nurses in HCS regarding the experience of moral distress.
Conclusions
The results of this study show that moral distress is a major problem for home-care nurses, threatens their health, and therefore poses a risk for the whole outpatient care situation.
The findings indicate that the service and billing system of HC in Germany, in which every care task is based on minutes, is incompatible with the nurses’ understanding of care and thus, leads to numerous ambiguities and causes moral distress. Nurses find themselves in a quandary between the economic demands of the HCS, bureaucratic requirements of health insurance companies, hierarchical structures of doctors, the demands of relatives, and the human needs of those in need of care. Alternative forms of home-care organization promise positive effects on nurses 39 and should be evaluated in Germany. One possibility is time-based remuneration, which would allow providing situational and individualized care to people with care needs independent of contractually agreed services. Sufficient funding must be provided for the time units for registered nurses, so that deprofessionalization through the increased use of less qualified staff is prevented. A transfer of medical activities, such as prescription of wound material to registered nurses, could prevent some of the morally stressful situations and improve patient care quality.
Home-care nurses often have little support in dealing with morally stressful situations and therefore have to deal with it on their own. According to Tomura 32 this “leaving issues unresolved coping style,” which the interviewees often reported, amplifies the frequency and intensity of moral distress. Thus, organizational ethical structures that are sensitive to possible morally stressful situations and home-care nurses’ moral distress need to be developed and strengthened as a whole to gain moral relief. 40 Targeted support and interventions that take effect directly in or in the aftermath of the morally stressful situation are therefore a priority. 41 Managerial support is important. 2 Up to now, the interviewees have used primarily informal exchange opportunities with colleagues to process their experience of moral distress. The time resources for service and case discussions were—also in view of the COVID-19 pandemic—strongly reduced by HCS. Given the significance of social support, this trend should be reversed quickly. The expansion of these discussion formats to include ethical topics (e.g., introduction of ethics consultations or ethics cafés with corresponding refinancing by health insurers) is necessary. Further research should evaluate interventions to reduce moral distress, considering the conditions in HC. The specific group that experiences moral distress and the practice setting play important roles for the development and implementation of interventions necessary to prevent the harmful consequences of moral distress. 5
Supplemental Material
Supplemental Material - Understanding moral distress in home-care nursing: An interview study
Supplemental Material for Understanding moral distress in home-care nursing: An interview study by Julia Petersen, Ulrike Rösler, Gabriele Meyer, Christiane Luderer in Nursing Ethics
Supplemental Material
Supplemental Material - Understanding moral distress in home-care nursing: An interview study
Supplemental Material for Understanding moral distress in home-care nursing: An interview study by Julia Petersen, Ulrike Rösler, Gabriele Meyer, Christiane Luderer in Nursing Ethics
Supplemental Material
Supplemental Material - Understanding moral distress in home-care nursing: An interview study
Supplemental Material for Understanding moral distress in home-care nursing: An interview study by Julia Petersen, Ulrike Rösler, Gabriele Meyer, Christiane Luderer in Nursing Ethics
Footnotes
Acknowledgements
We are grateful to the 20 home-care nurses who spoke openly about their experiences with moral distress and the participants of the International Graduate Academy of the Institute of Health and Nursing Science at the Martin Luther University Halle-Wittenberg for the collegial support and the exchange of experiences regarding aspects of the research topic and the methodological approach.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The German Federal Institute of Occupational Safety and Health funded the data collection process and ensured the authors’ employment during the study (research project F2521).
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.