
Abstract
Ethics is a foundational competency in healthcare inherent in everyday nursing practice. Therefore, the promotion of qualified nurses’ and nursing students’ moral competence is essential to ensure ethically high-quality and sustainable healthcare. The aim of this integrative literature review is to identify the factors contributing to the promotion of qualified nurses’ and nursing students’ moral competence. The review has been registered in PROSPERO (CRD42023386947) and reported according to the PRISMA guideline. Focusing on qualified nurses’ and nursing students’ moral competence, a literature search was undertaken in January 2023 in six scientific databases: CINAHL, Cochrane Library, PsycINFO, PubMed Medline, Scopus and Web of Science. Empirical studies written in English without time limitation were eligible for inclusion. A total of 29 full texts were retrieved and included out of 5233 citations. Quality appraisal was employed using Joanna Briggs Institute checklists and the Mixed Method Appraisal Tool. Data were analysed using inductive content analysis. Research about the factors contributing to the promotion of qualified nurses’ and nursing students’ moral competence is limited and mainly explored using descriptive research designs. The contributing factors were identified as comprising two main categories: (1) human factors, consisting of four categories: individual, social, managerial and professional factors, and ten sub-categories; and (2) structural factors, consisting of four categories: educational, environmental, organisational and societal factors, and eight sub-categories. This review provides knowledge about the factors contributing to the promotion of qualified nurses’ and nursing students’ moral competence for the use of researchers, nurse educators, managers, organisations and policymakers. More research about the contributing factors is needed using complex intervention, implementation and multiple methods designs to ensure ethically sustainable healthcare.
Introduction
Ethics is a foundational competency in healthcare 1 and is inherent in all nursing practices. 2 Healthcare professionals demonstrate their ethical competence in providing high-quality care to patients. 3 Constantly changing society and healthcare environments with ever-growing demands for ethically sustainable care require nurses’ and nursing students’ moral competence to evolve continuously. This became more evident during the COVID-19 pandemic which required nurses to make difficult ethical decisions,4,5 and with the phenomenon of missed care that requires nurses to prioritise scarce resources. 6 Therefore, it is important to develop a support system to promote and sustain nurses’ and nursing students’ moral competence.
Background
The terms moral competence and ethical competence have been used interchangeably in the literature. 7 Moral competence has been defined as ‘the ability or capacity of persons to recognise their feelings as they influence what is good or bad in particular situations, and then to reflect on these feelings, to make their decision, and to act in ways that bring about the highest level of benefit for patients’. 8 (p. 586). Ethical competence in healthcare, in turn, is defined as ‘a personal capacity including ethical awareness, courage, willingness and skills in decision-making and ethical action’. 9 (p. 410). As moral competence and ethical competence have been used synonymously, in this review, the concept of moral competence is used and defined in terms of perceptions (seeing), knowledge (knowing), reflection, deliberation and acting as a professional caregiver. 10
There is a wealth of literature on what constitutes nurses’ moral competence,3,7,9 as well as the level of their moral competence 11 and the variables associated with it, such as ethics education,12,13 and nurses’ ethical reasoning and behaviour. 14 However, the literature on factors that contribute to the promotion of qualified nurses’ and nursing students’ moral competence is limited. Factors have been considered by the research team in this study context as those elements facilitating, contributing or leading to a specific outcome, as the promotion of moral competence among nurses and nursing students. The pedagogical approaches in teaching or learning ethics in undergraduate nursing education have been found to be limited in terms of what should be taught about ethics, and how and by whom it should be taught. 15 There is also great variation and diversity globally, with some countries offering ethics as stand-alone courses while in others, it is integrated into other subject areas. Similarly, the delivery of ethics education in nursing education varies with practices like clinical and didactic courses including discussions, simulation, case-based learning, problem-based techniques, role play and analysing ethical issues. 16 In view of the increasing complexity of care and the accompanying emergence of new ethical challenges, there is a need to re-examine the content of nursing curricula to enhance the promotion of morally competent nurses as well as teaching practices that are more adaptive to the changing learning needs.
Factors that support and contribute to the promotion of moral competence have been identified not only in education but also in clinical settings. The main aims of support are to improve ethical decision-making and action in the clinical environment, to prevent, mitigate or reduce the ethical burden, supervise policymaking and provide guidelines, education and consultation. 17 The ethical competence of healthcare professionals in undergraduate, continuing and clinical education can be promoted through various interventions, especially educational ones. 18 However, an integrative summary of the factors that may contribute to the promotion of moral competence was not identified from the literature.
The importance of ethics in healthcare and the requirement of moral competence from nursing professionals in providing high-quality care with respect to human and patients’ rights have been acknowledged in the literature.3,4,9 In addition, ethics education in nursing curricula and the best practices varies globally. 16 Therefore, this review was conducted to identify the factors that can contribute to the promotion of moral competence of qualified nurses and nursing students not only in educational institutions but also in healthcare organisations.
Aim
The aim of this review was to identify the factors contributing to the promotion of qualified nurses’ and nursing students’ moral competence.
Methods
An integrative review method was used and its five steps followed according to the methodological model of Whittemore and Knafl, 19 namely, (a) problem-identification, which ensures that both the research question and purpose are appropriately formulated; (b) research strategy and literature search; (c) methodological quality assessment, (d) data analysis; and (e) presentation and synthesis of findings. The review protocol has been registered in the International Prospective Register of Systematic Reviews (CRD42023386947). The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 20 was followed.
Search strategy
A literature search regarding factors contributing to qualified nurses’ and nursing students’ moral competence was carried out to identify relevant scientific research articles. The searches were undertaken on 2nd–4th January 2023 from the earliest content in six scientific databases: CINAHL, Cochrane Library, PsycINFO, PubMed Medline, Scopus and Web of Science. The search terms and strategies were developed in collaboration with a health and medical science library informatics expert. The following terms were used with the Boolean operators AND or OR: (nurse OR nursing OR nursing student OR student nurse) AND (moral competence OR ethical competence OR ethical sensitivity OR ethical decision-making OR ethical knowledge OR ethical behaviour OR ethical behaviour OR ethical reflection OR ethical reasoning OR moral courage OR moral care). The keywords were applied in all databases and MeSH terms were also used when appropriate. In addition, the reference lists of the included articles and relevant reviews were screened; however, this did not produce any new articles to the review. The Zotero software was used to manage references. 21
Inclusion and exclusion criteria
The studies were included if they focused on (1) the moral competence of (2) qualified nurses (registered nurses, practical nurses, Advanced Practice Nurses) or nursing students, including articles that also covered other healthcare professionals in addition to them, (3) identify the factors contributing to the promotion of moral competence, (4) peer-reviewed empirical articles (including all research methods), written in (5) English language and with (6) abstract available. The studies were excluded if they dealt with (1) the moral competence of manager-level nurses, nurse aids, nurse assistants, or solely of other healthcare professionals, and if the articles were (2) theoretical articles, literature reviews, books, dissertations, reports, editorials, opinions, discussion papers or grey literature.
Quality appraisal
Quality appraisal was employed using the Joanna Briggs Institute Critical Appraisal Checklists for Qualitative Research in twelve studies, for Analytical Cross-Sectional Studies in eleven studies, and for Quasi-Experimental Studies in five studies. 22 However, for one mixed-method study the Mixed Method Appraisal Tool (MMAT) 23 was used instead, as no Joanna Briggs Institute (JBI) checklist existed for this purpose. The ranking of the JBI checklist items included Yes, No, Unclear and Not applicable. The quality of the included articles was rated as moderate (n = 10) or high quality (n = 18). The mixed-method article was rated as low quality. However, as suggested in the literature, none of them were excluded based on quality appraisal. 23 The quality appraisal of each article was carried out by two researchers. A total of eight researchers (JW, MS, SC, CG, BK, EM, EP, RS) participated and discrepancies were resolved among three researchers (JW, MS, RS).
Data analysis
Example of data analysis.
Findings
Studies retrieved
The studies were retrieved according to the four stages of the PRISMA
20
flowchart (Figure 1). At the first stage, 5233 records were identified from six databases; 2949 duplicates were removed. The remaining 2284 records were then screened by their titles and abstracts. Following this, 50 full text reports remained, which were screened for eligibility. Twenty-one reports were excluded. In the last stage, 29 studies were included in the review. The PRISMA flow diagram, 2020 statement: An updated guideline for reporting systematic reviews.
20
Characteristics of the studies
Studies (n = 29) about moral competence included in the review according to study design.
aJoanna Briggs Institute’s checklists and Mixed Method Appraisal Tool.
The designs of the studies were mainly qualitative26,30–36,41,45,48,51 or quantitative.27–29,37,38,42–44,46,47,53 One study had a mixed-method design, 50 and a quasi-experimental design was used in five studies25,39,40,49,52 three of which had control groups.25,49,52 Data were mainly collected with interviews26,30,31,33–36,41,45,48 or questionnaires,25,27–29,37–40,42–44,46,47,49,52,53 one study used video filming, 51 one used both questionnaire and focus group interview, 50 and one used individual interviews and field notes. 32
The participants were mainly nurses29,32,34,37,38,41–43,50 or nursing students.30,35,40,44–47,49,51,52 In addition, seven studies included a mix of healthcare professionals or students25,26,28,31,39,48,53 such as physicians or medical students; however, the majority of the participants in those studies were nurses or nursing students. Even though, in some studies the participants were nurse teachers 36 or professors 33 or nurse leaders, 27 the articles focused on qualified nurses’ or nursing students’ moral competence and how to support it. The number of participants in qualitative studies ranged between 6 and 30, in quantitative studies between 83 and 3,493, and in quasi-experimental studies between 100 and 333 (Table 2). One mixed-method study included 14 participants. 50
Third of the studies proposed that exploring stakeholder’s experiences,30–32,36,41,45 perceptions34,48,51 or views 26 on competence was meaningful in order to describe and make visible the meaning and existence of competence. One study raised the promotion of moral competence on strategies and spaces as pedagogical teaching solutions. 33 In several studies,25,35,39,40,44,47,49,50,52 the contributing factors were different educational interventions including basic education and continuing education. In addition, the interventions included ethics training programmes including ethics rounds, educational workshops, interactive e-learning interventions, pedagogical experiments and simulations. Six studies focused on the evaluation of the moral competence level of qualified nurses and nursing students.28,37,38,42,43,46 By operationalising moral competence, awareness of the required level becomes apparent, contributing to the promotion of moral competence. Finally, support from a third party, including superiors or organisational support structures such as clinical ethics support, was identified in three studies.27,29,53
Factors contributing to the promotion of moral competence
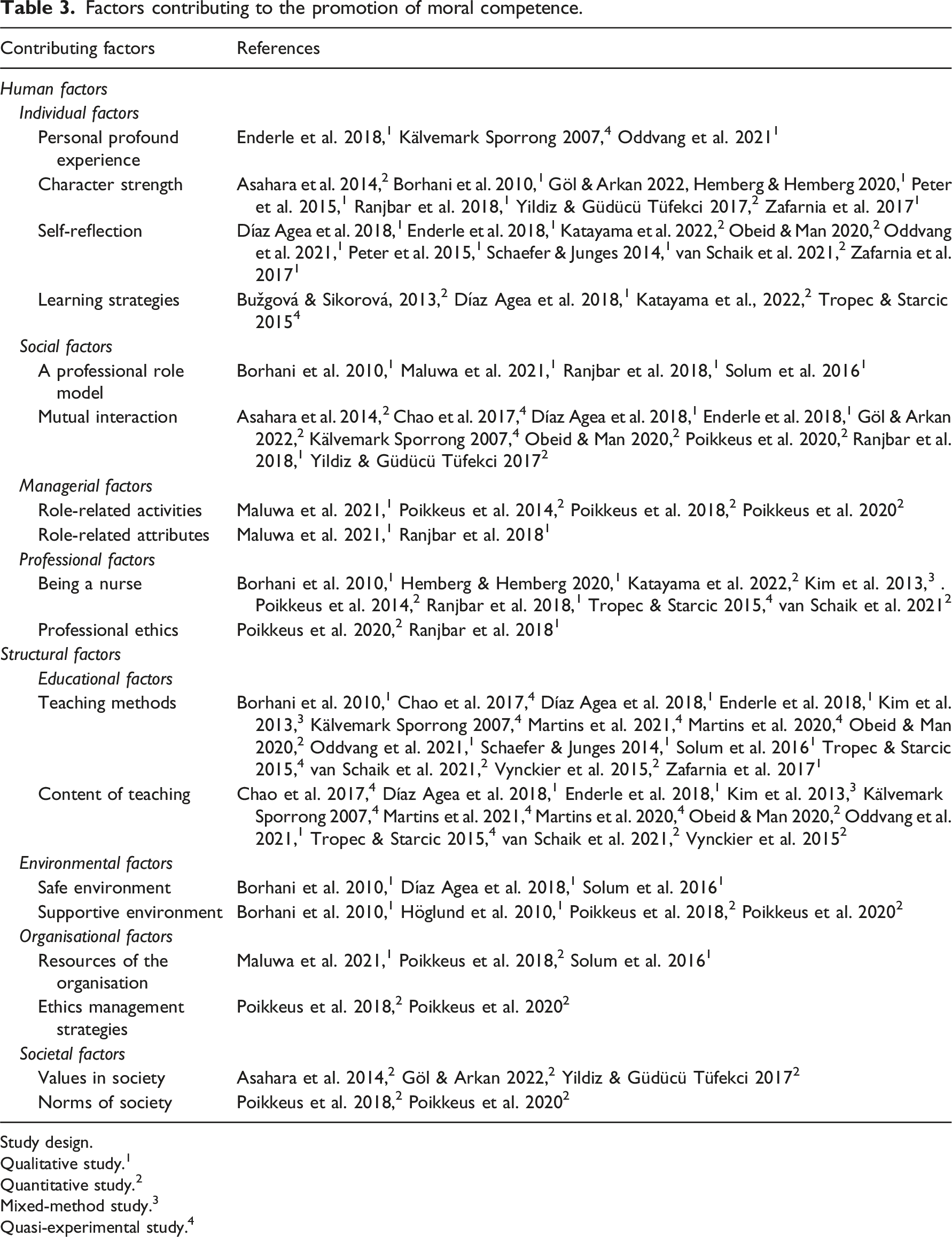
Factors contributing to the promotion of qualified nurses’ and nursing students’ moral competence were identified as comprising two main categories, human factors and structural factors, consisting of eight categories and eighteen sub-categories. Human factors consist of four categories: individual, social, managerial and professional factors, and ten sub-categories. Structural factors consist of four categories: educational, environmental, organisational and societal factors, and eight sub-categories. Human factors relate to the individual oneself, others such as patients, colleagues, managers and teachers and the nursing profession, whereas structural factors relate to the workplace (micro), organisation (meso) and society (macro) level structures (Figure 2, Table 3). Moral competence contributing factors: Main categories, categories and sub-categories. Factors contributing to the promotion of moral competence. Study design. Qualitative study.
1
Quantitative study.
2
Mixed-method study.
3
Quasi-experimental study.
4
Human factors
Individual factors contribute to the promotion of qualified nurses’ moral competence through the individuals themselves. This category comprises four sub-categories:
Social factors contribute to the promotion of qualified nurses’ moral competence through interaction and collaboration in workplace relationships. Two sub-categories were identified as
Two sub-categories of managerial factors were identified:
Two sub-categories of professional factors were also identified as human factors:
Structural factors
Educational factors conducted by educational specialists contribute to the promotion of qualified nurses’ and nursing students’ moral competence through
Two sub-categories of environmental factors were identified:
Two sub-categories of organisational factors were also identified:
Societal factors contribute to the promotion of qualified nurses’ moral competence by
Discussion
This review provides knowledge about the factors contributing to the promotion of qualified nurses’ and nursing students’ moral competence. This knowledge is useful for the development of ethics education interventions and everyday clinical practice. The results indicate that the moral competence can be promoted by various factors at all levels, from the level of an individual nurse or nursing student (micro) to society (macro) level. Given the importance of ethics in healthcare and the required moral competence of professionals, 4 only a limited number of studies about factors contributing to the promotion of moral competence was discovered. However, the number of studies has been increasing during the past decade. Consistent with previous considerations, 3 this indicates a growing interest in exploring nurses’ and nursing students’ moral competence. This can be explained by the increased requirement to prioritise scarce resources 6 and address ethical issues 4 and the need to alleviate the increased moral distress 54 to which moral competence is a potential response.
The nature of the integrative method and the international character of the review allowed combining evidence produced with different study designs, identifying a broad perspective of the factors contributing to the promotion of moral competence. The studies, both qualitative and quantitative were mainly descriptive and based on nurses’ or nursing students’ experiences or their self-assessed level of moral competence, thus providing an insight into the contributing factors. In addition, some educational interventions were identified. However, in order to gain a deeper understanding and to see whether these factors are effective in contributing to the promotion of moral competence, more research is needed using intervention studies, 18 implementation research and multiple methods designs.
Human and structural factors contributing to the promotion of moral competence were identified (Figure 2). Human factors were identified in relation to the individual oneself, others such as patients, colleagues, managers and teachers and the nursing profession, whereas structural factors were related to the workplace (micro), organisation (meso) and society (macro) level structures. Human factors that contribute to the promotion of moral competence relate mainly to informal practices and processes. This is supported by the literature stating that informal practices refer to socialisation processes, human encounters, interaction and professional autonomy. 55 In addition, the findings indicate that structural factors create formal and structured practices, policies, strategies and programmes and enable informal opportunities for the systematic promotion of moral competence. 56
The findings of human factors indicate that it is possible for individuals to promote their moral competence if they are empowered to practice as nurses and use their experiences in a positive way. In addition, it is expected that those who have chosen nursing as a career possess certain characteristics and are usually willing to help and do good to other people. 57 In relation to other people, moral competence does not exist in a vacuum. Hence, the findings suggest that it is important for both nurses and nursing students to have ethical role models, colleagues and managers with whom to reflect critically on ethical issues14,58 in order to provide ethically high-quality care. In addition, it is stated that managers have a key role in promoting nurses’ moral competence by providing support and encouragement, 59 which was also identified in this review.
The findings on structural factors indicate that attention must be paid to the content of teaching and the diversity of teaching methods when designing education and curricula. 12 In addition, according to the findings, it is suggested that healthcare services need to build resilient organisations to support ethics management and enhance ethically sustainable nursing practices. Moral competence should also be given thorough consideration when making health policy decisions on a societal level. These may remove the impediments to nurses’ integrity and build psychological safety and a moral community where moral competence is effectively promoted. 4 In addition, considering moral competence and the multiple levels of contributing factors, 10 a complex intervention engaging stakeholders from the micro (patients, nurses, nursing students, managers and teachers) to the macro (policymakers) level is needed to effectively promote the moral competence of nurses and nursing students. Therefore, it is necessary to discuss whether the moral competence of individuals will broaden into ethical competence of the profession and the organisation. It is not enough to have morally competent individuals; highlighting professional ethics and supporting collective ethical competence as well as advancing value-based healthcare and care provision for patients is also needed.
Limitations and strengths of the review
There are some limitations and strengths in this review. As a limitation, the literature search was performed by one researcher; however, the review protocol was registered in PROSPERO and followed throughout the process. The search strategy was developed among the research team and the search terms in collaboration with library informatics expert. In addition, preliminary searches were conducted by another person within the research team. Furthermore, reference lists of the included articles and relevant reviews were screened to identify all the relevant literature; however, it did not produce any new results.
A further limitation is that only studies written in English were included, introducing a potential selection bias. It should be noted that these studies originated from various countries, ensuring a multicultural perspective. Moreover, in order to ensure inclusiveness, no studies were excluded due to poor quality; as strengths any discrepancies were resolved among three researchers and according to the literature, excluding studies on the basis of poor quality is not recommended. 23
As the final limitations, studies regarding the moral competence of mixed professionals were not excluded given that the majority of the participants were qualified nurses or nursing students. Furthermore, the data analysis process was performed by researchers from multiple countries, which may have introduced bias since only EU countries were included; however, no pre-defined frameworks were used, and the international perspective, as well as the inductive approach, may have prevented interpretation bias.
Conclusion
Moral competence is a phenomenon that is essential to ensure ethically high-quality and sustainable healthcare. Research about the factors contributing to the promotion of qualified nurses’ and nursing students’ moral competence is limited but seems to be increasing. Human and structural factors were identified as the two main categories contributing to the promotion of moral competence from micro to macro levels. This review provides knowledge for researchers to develop interventions such as ethics education programs and to conduct implementation research. For nurse educators, this review provides knowledge to plan and develop ethics education, nursing education and nursing curricula. Moreover, this review provides knowledge for managers and organisations to create ethics structures that support and promote individuals’ moral competence, and for policymakers to enable the creation of such structures. It is important for both practice and education to pay attention to individuals’ ethical conduct by supporting and encouraging their moral competence and moral development from the beginning of basic nursing education throughout nursing careers and life-long learning. To gain a deeper understanding and to see whether the identified factors are effective in contributing to the promotion of moral competence, more research is needed using complex intervention, implementation and multiple methods designs, which would ensure ethically high-quality and sustainable healthcare.
Footnotes
Author’s note
On behalf of the PROMOCON consortium: Stefania Chiappinotto, University of Udine, Department of Medicine; Maria Dimitriadou, (1) Cyprus University of Technology, School of Health Sciences, Department of Nursing, (2) Cyprus Nurses and Midwifes Association; Georgios Efstathiou, Melina Evripidou & Paraskevi Charitou, Cyprus Nurses and Midwives Association; Alessandro Galazzi, University of Udine, Department of Medicine; Chris Gastmans, Department of Public Health and Primary Care, Centre for Biomedical Ethics and Law; Michael Igoumenidis, University of Patras, Department of Nursing; Brian Keogh, Trinity College Dublin, School of Nursing & Midwifery; Jessica Longhini, 1 University of Verona, Department of Diagnostics and Public Health, 2 University of Udine, Department of Medicine; Catherine Mc Cabe, Trinity College Dublin, School of Nursing & Midwifery; Evelyne Mertens, KU Leuven, Department of Public Health and Primary Care, Centre for Biomedical Ethics and Law; Alvisa Palese, University of Udine, Department of Medicine; Evridiki Papastavrou, (1) Cyprus University of Technology, School of Health Sciences, Department of Nursing, (2) Cyprus Nurses and Midwifes Association; Nikos Stefanopoulos University of Patras, Department of Nursing; Minna Stolt, (1) Department of Nursing Science, University of Turku, and (2) Wellbeing Services County of Satakunta; Riitta Suhonen, (1) Department of Nursing Science, University of Turku, 2) Turku University Hospital, Wellbeing Services County of Southwest Finland; Johanna Wiisak, Department of Nursing Science, University of Turku; Maria Zafiropoulou, Non-Governmental Organization ‘Co2gether’.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was Co-funded by the Erasmus + programme of the European Union (agreement nr. 2022-1-IT02-KA220-HED-000087544). The European Commission’s support for the production of this publication does not constitute an endorsement of the contents, which reflect the views only of the authors, and the Commission cannot be held responsible for any use which may be made of the information contained therein.