
Abstract
Background
Nurses play an integral role in the care of children hospitalised with a serious illness. Although information about diagnostics, treatments, and prognosis are generally conveyed to parents and caregivers of seriously ill children by physicians, nurses spend a significant amount of time at the child’s bedside and have an acknowledged role in helping patients and families understand the information that they have been given by a doctor. Hence, the ethical role of the nurse in truth disclosure to children is worth exploring.
Methods
A systematic academic database and grey literature search strategy was conducted using CINAHL, Medline Psych Info, and Google Scholar. Keywords used included truth, children, nurse, disclosure, serious illness, and communication. A total of 17 publications of varying types were included in the final data set.
Ethical Considerations
As this was a review of the literature, there were no direct human participants. Empirical studies included in the review had received ethics approval.
Results
Of the 17 articles included in the review, only one directly reported on the experiences of nurses asked to withhold the truth from patients. Empirical studies were limited to HIV-positive children and children diagnosed with cancer and the dying child.
Conclusion
A paucity of literature exploring the experiences, attitudes, and beliefs of nurses with regard to truth-telling to seriously ill children is evident. Little consideration has been given to the role nurses play in communicating medical information to children in a hospital setting. The 17 articles included in the review focused on cancer, and HIV, diagnosis, and end-of-life care. Further research should be undertaken to explore the experiences and attitudes of nurses to clinical information sharing to children hospitalised with a wide range of serious illnesses and in diverse clinical scenarios.
Keywords
Introduction
Delivering diagnostic and prognostic information to parents and children in the paediatric hospital setting is generally considered to be role of the physician. Disclosure and truth-telling by physicians to seriously ill patients including children has been explored widely in the published literature.1–3 The role of the nurse, when discussed, is typically framed as a support person in the disclosure process,4–7 with the nurse ‘being left to pick up the pieces’ and provide an explanation after the diagnosis and prognosis are received from the physician. 8
Nevertheless, information disclosure and truth-telling in the paediatric setting is an important issue for nurses to reflect upon, given their integral role in the care of hospitalised children. While physicians, physiotherapists, pharmacists, and other members of the health care team see inpatients and their families for parts of a shift, the nurse will spend a significant amount of time at the child’s bedside. Nurses play an important role in supporting the child and parents’ understanding of the hospital communication channels, as well as the information they have been given by a doctor. Nurses can be asked questions about a child’s clinical condition, not only by the parents, but also by the children themselves. The ethics of truth-telling and information sharing in clinical settings and the ethical role of the nurse in truth disclosure to children is an important issue for nurses, in need of deeper exploration.
Background
Telling the truth to children is more ethically contested than telling the truth to adult patients due to the ethical complexities and legalities surrounding consent, autonomy, and cognitive capacity of a minor. 9 Decisions in paediatric health care are made based on the ‘best interests’ principle, that is, deciding what is best for the child.9–11 The reasons typically given for withholding clinical information from children centre on the belief that it is in the best interests of the child. Specific instances and justifications where this has occurred include: the preservation of a safe and healthy relationship between the parents and the child; the child’s inability to emotionally or cognitively process the information; and parents’ desire for their child to maintain a level of hope for recovery or cure.9,11 When communicating medical information, it is important to consider a child’s cognitive capacity which is not always reliant on age rather, on the achievement of their developmental milestones. Children’s diversity in cognitive function and their ability to understand the truth of their medical condition can vary from minimal or some capability to understand to full decision-making capacity and autonomous consent. Younger children or those with diminished cognitive capacity such as an intellectual disability, who do not have capacity to make their own medical decisions independently would generally be represented by a parent or guardian who makes decisions and consents on their behalf. Adolescents or mature minors, however, may have decision-making capacity, and be able to give their own consent to medical treatment. 9 Mature minors can be seen as having a right to autonomy over their own bodies because they have decision-making capacity. Hence, truth-telling to the mature minor is not so contentious, as complete and truthful information is required for informed consent.9–12 The challenge lies in assessing the capacity of children and adolescents when their cognitive, social, and intellectual development is diverse and dependent on their age and lived experience.
For younger children, who do not have decision-making capacity, truth-telling is more contentious, as they do not have a right to information based on a need to give informed consent. 13 It can also simply seem kinder to children not to give them information that will be upsetting to them. However, the principles of biomedical ethics as described by Beauchamp and Childress (2019), establish sound ethical reasons that support honesty in medical information sharing even to younger children, including the provision of some degree of involvement in decision-making, enhancing engagement in the therapeutic relationship, improving the child’s emotional and psychological well-being, and promoting future autonomy. 13 Harrison (2009) and Rosenberg et al (2017) support the view that Western medicine encourages development of a therapeutic relationship with children and their families that is open and honest and hence would support information sharing in a way that children understand.14,15
A paper by Gillam et al (2022) extensively considers the interests and rights of the child with a serious illness to information, when parents give a non-disclosure directive. 16 Both concepts of rights and interests are complex. There are instances when the rights of a seriously ill child to medical information may be in conflict with the right of the parent to protect their child by means of withholding this information. 16 Conversely, paediatric clinical ethics works on the principle that decisions made regarding information, diagnostics and treatment is focussed on the best interests of the child. 16 The subjectivity of what different people believe are in the best interests of the child adds a layer of complexity to decision-making when considering this concept. With these considerations, we look at how the principles of biomedical ethics, specifically autonomy, non-maleficence, and beneficence are applied within a clinical context.17,18
When contemplating these ethical principles, their application to nursing perspectives and bedside experiences of information disclosure and truth-telling to children is not clear. The purpose of this literature review is to establish what is currently known about how nurses see their ethical role in disclosure to children, and what nurses actually do at the bedside when truth-telling becomes an issue. This may guide us in articulating ethical approaches in challenging scenarios in the paediatric healthcare setting if the literature is sufficiently high-quality and comprehensive. If not, the review will identify where further research is needed.
Definitions
For the purpose of the review, the term ‘seriously ill children’ will refer to children who have a medical condition that requires hospitalisation, or a chronic condition has impacts on the child’s life, requiring ongoing treatment and monitoring. Reference to child will indicate children aged 3 to 18; and the nurse is a qualified health professional registered by a professional body as having undertaken an accredited program to register or enrol as a nurse.
Review question
What are the attitudes, experiences, and beliefs of nurses in truth-telling to seriously ill children?
Methods
Search strategy
A systematic approach to the review of the literature was undertaken including a ‘comprehensive plan and search strategy’.
19
The checklist for systematic reviews and the critical and quality appraisal tools on the Joanna Briggs Institute site were used to support systematic approach (see Supplementary Materials).
20
A systematic review is ‘a form of research synthesis that seeks to systematically search for, appraise and synthesize research evidence, using strategies to limit bias often adhering to guidelines on the conduct of a review’.
21
This review was conducted using the workflow of information retrieval tool by Droste et al (2010). This eight step process includes the translation of the research question to a search question which leads to modelling of the search components, identification of synonyms, selection of appropriate articles, designing search strategies, executing the search, saving and documenting the results, and undertaking a quality check.
22
The review question was translated to a modified PIO (population, intervention, outcome) model, as represented below. • Population: Children hospitalised with a serious illness and nurses caring for them • Intervention: Disclosing of medical information to children. • Outcome: The experiences, beliefs, and attitudes of nurses in relation to disclosing the truth to seriously ill children.
The search was undertaken in the period between August and September 2021 and then repeated in November 2022 to ensure any new publications would be identified. With the support of a research librarian, Medline, CINAHL, and Psych Info databases were chosen for use because they are the major databases that hold publications specific to the topic in the fields of nursing, psychology and ethics. In addition to these databases, a grey literature search using Google Scholar was also undertaken.
Key words were identified to ensure the search was specific to the topic. The full search strategy can be found in the Supplementary Materials. The terms ‘truth-telling’ and ‘disclosure’ were used to describe the phenomenon of interest. Nurses of all qualifications were used as part of the search strategy that included ‘enrolled’ and ‘registered’. ‘Infant’ was intentionally excluded from the search strategy as truth-telling is only relevant to children who had some capacity to understand verbal communication. The key terms were then combined with the Boolean operator ‘AND’ resulting in a large number of articles for screening.
Inclusion criteria
All studies that examined and discussed the role of the nurse in truth-telling to seriously ill children were considered. No specific clinical settings or publication time frames were defined. Both theoretical and empirical publications were included in the review as both types could answer the review question. In summary, the articles that were included in the review had to meet all the following criteria: • Be in English • Have abstract available. • Include Truth-telling or non-disclosure. • Include serious illness. • Include Nurses • Include Children over 2 years old.
Exclusion criteria
Publications that did not consider the nurse in the clinical setting were excluded. Empirical studies that did not state ethics approval were also excluded.
Study selection
The search resulted in a total of 4552 articles. All articles were independently screened by title and abstract for relevance to the review question by two of the authors (MEA and LG). The authors used COVIDENCE to support the process and any conflicts in article inclusion that presented were mutually resolved. There were 179 articles that reached full text screening. Any discord in full text article screening was resolved by the second and third author (LG and SL). Finally, full text article reference lists were scrutinised for potentially relevant unidentified articles. A total of 17 publications were analysed for the review. The PRISMA diagram in Figure 1 provides details of the screening process. Prisma diagram. Adapted from: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71.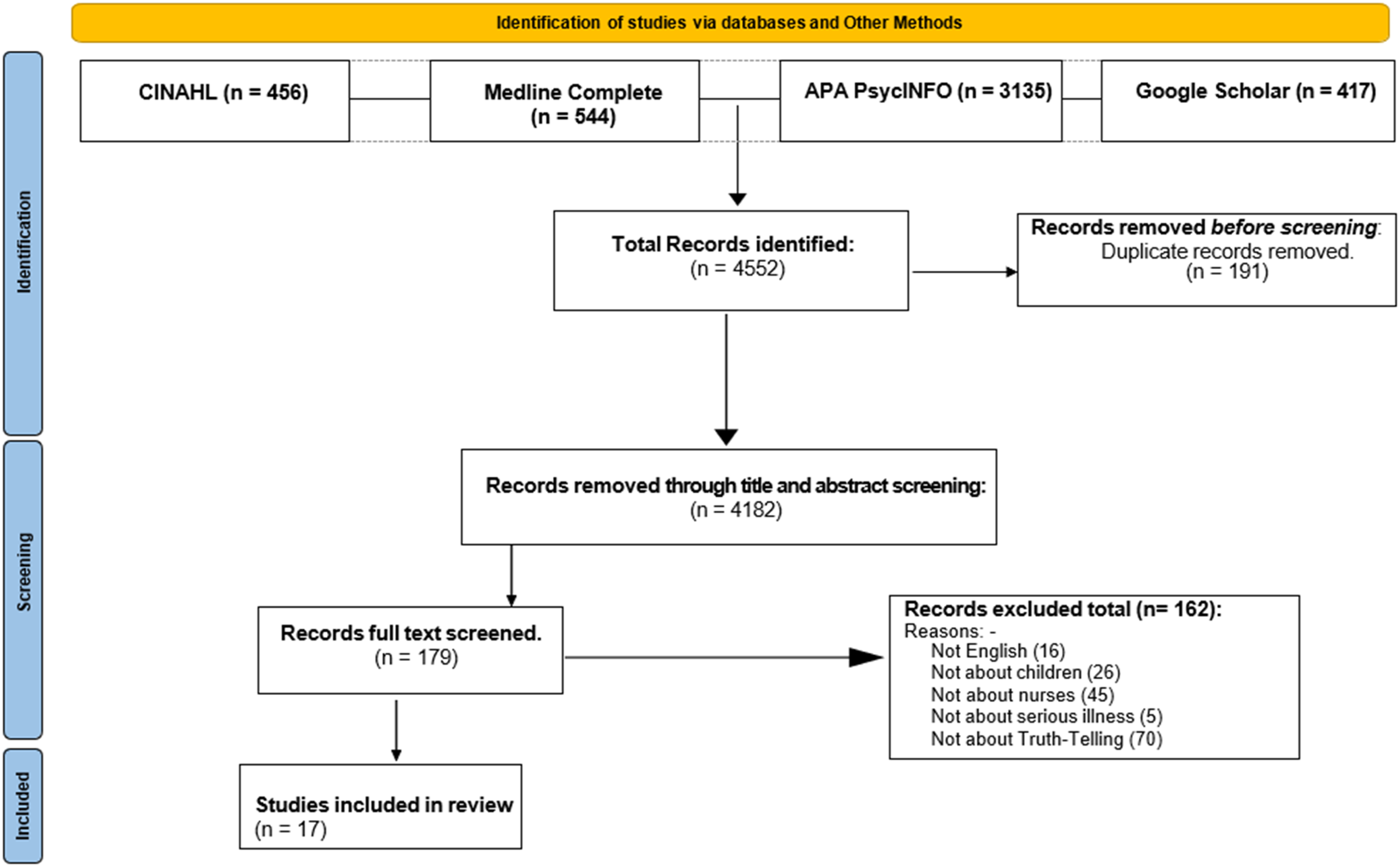
Data extraction
Included studies were analysed with a data extraction template developed by the authors to ensure information was systematically collected which met the pre-determined inclusion criteria. 19 The extraction template supported the identification of the characteristics of the articles including demographic information (country, clinical focus, empirical/nonempirical), and the aims and key findings or key points relevant to the attitudes, experiences, and beliefs of nurses in disclosure of medical information to seriously ill children. The data extraction template supported a critical analysis of each included article with defined parameters that focussed on the research question.
Quality assessment
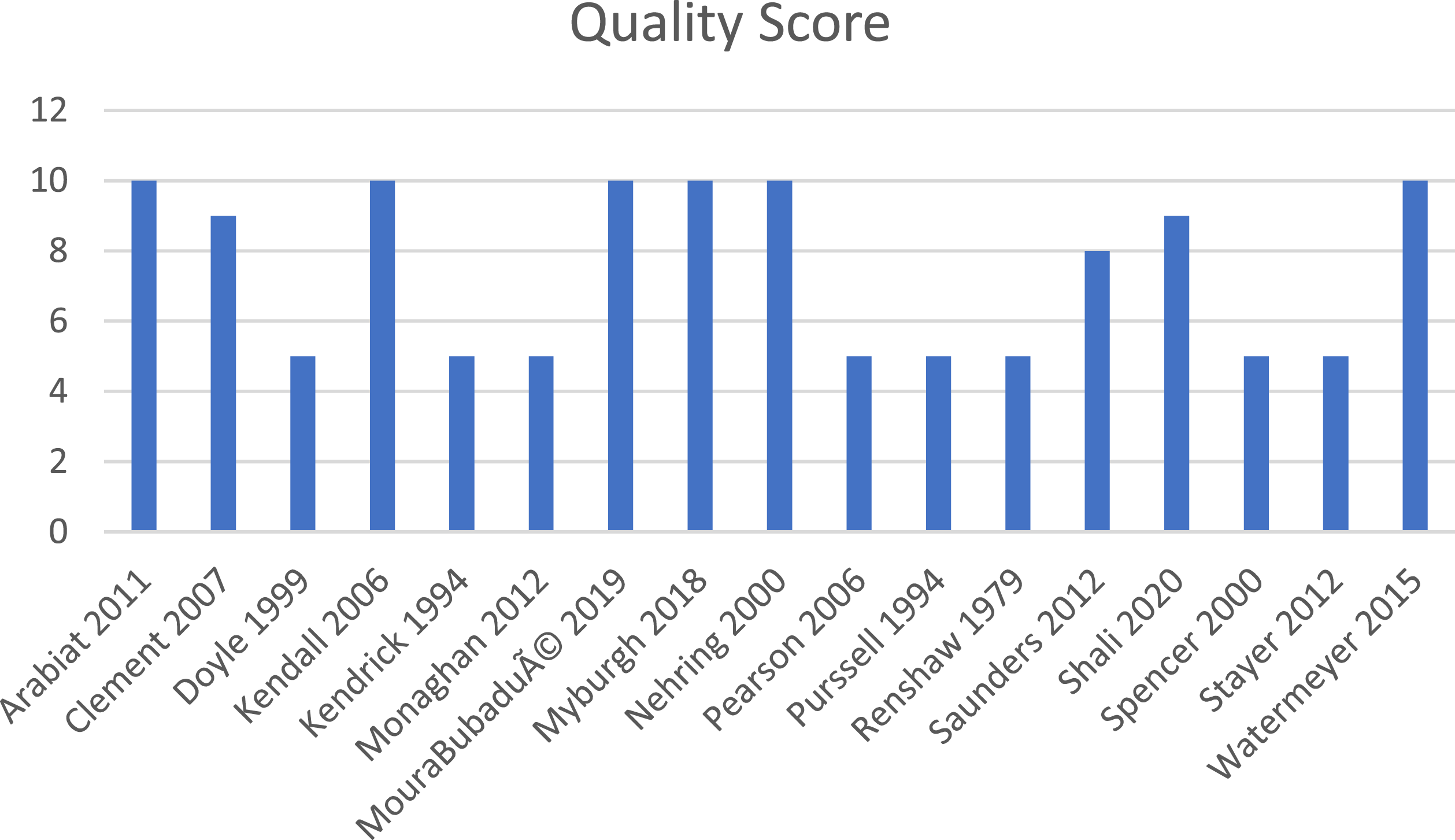
The quality of the included articles was assessed using Joanna Briggs critical appraisal tool for qualitative studies and systematic reviews. 23 Quality was assessed on the clarity and link between aims and findings of the publications. Qualitative studies were assessed on the congruity between the research methodology and philosophical grounds, ethical conduct and approval, specifically asking 'Is the research ethical according to current criteria or, for recent studies, and is there evidence of ethical approval by an appropriate body?’, 24 methods of data collection and links between the aims, findings, and the conclusions drawn. 25 The included studies were diverse in their methodology ranging from qualitative studies, to ethical analyses and discussion papers. The discussion papers scored lower than the empirical studies, as the critical appraisal tool was not designed for this type of paper. This did not diminish their value in terms of addressing the review aims.
Quality Assessment Results using JBI quality appraisal tool.
Results
Overview of included publications
The 17 included articles were published over the period between 1979 and 2020 (see Figure 2) Eight of the 17 included publications were empirical studies, and the other nine were ethical analyses and discussions. Tables 1 and 2 provide full details of all included articles. The review was focused on the attitudes, experiences and beliefs of nurses about truth-telling to seriously ill children. All the included articles therefore referenced the nurse, the child and disclosure practices in a hospital or clinical setting where the child was diagnosed with or being treated for a serious illness. Publication years. Non-empirical data publications in chronological order. Empirical studies in chronological order.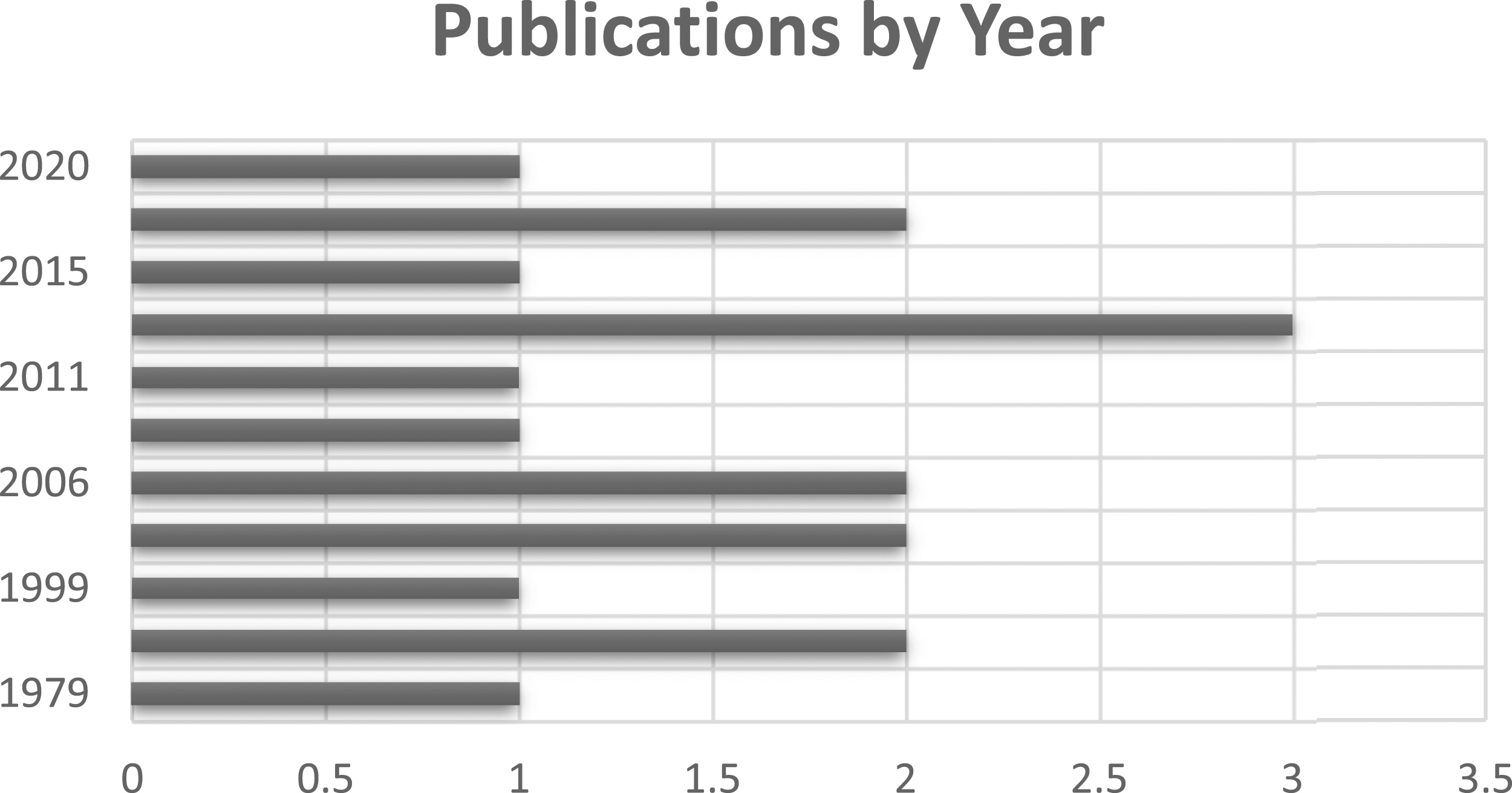
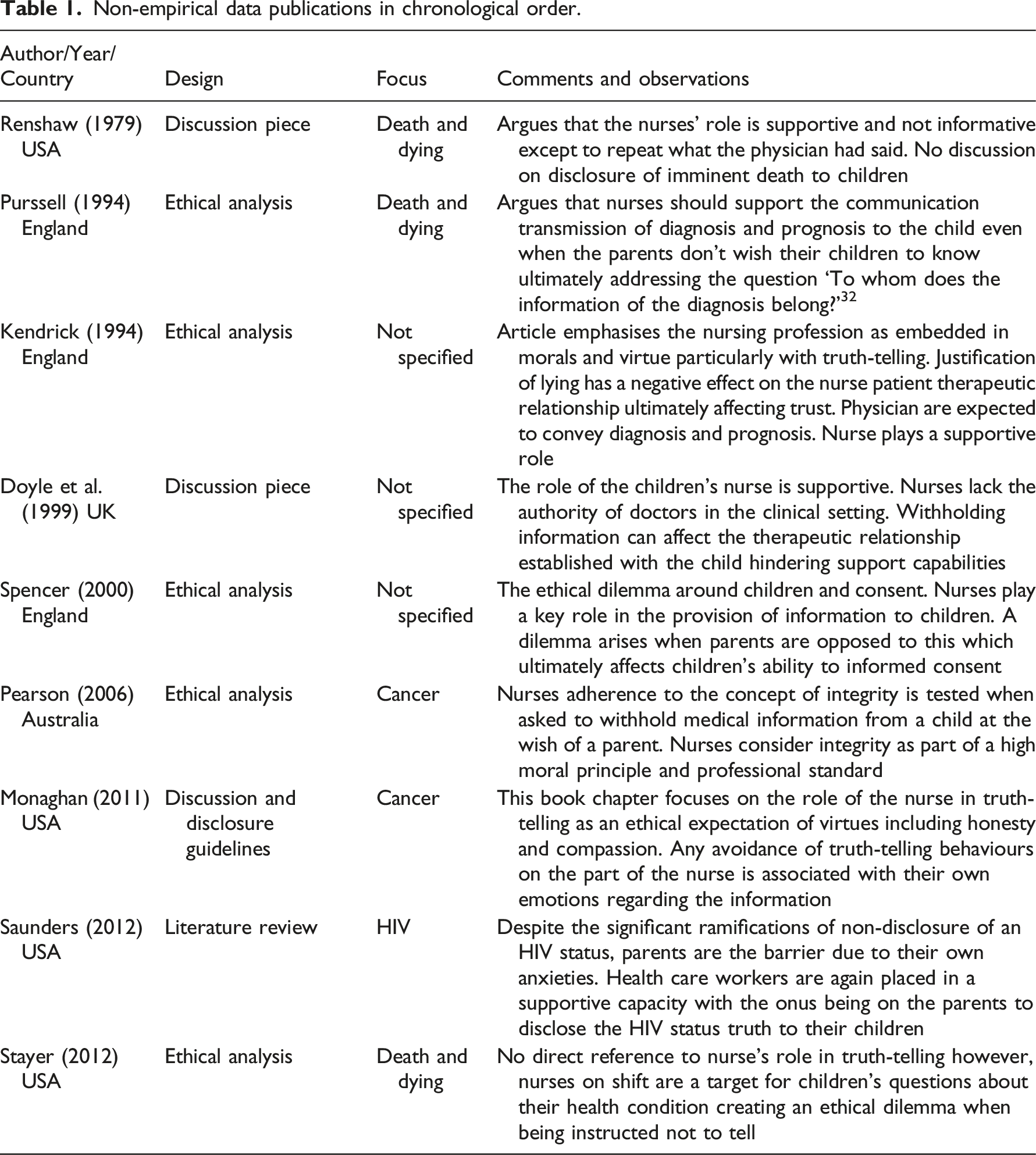
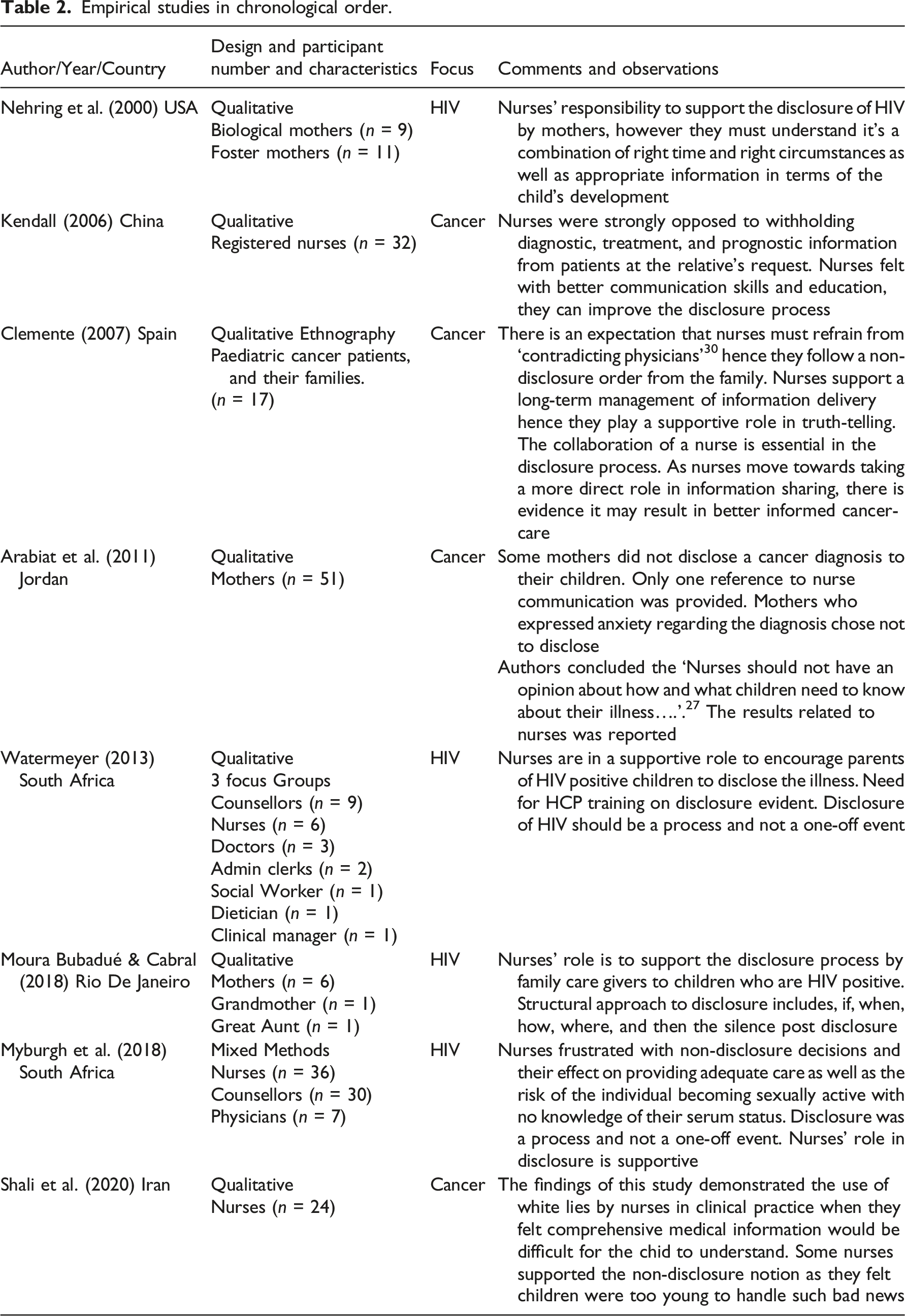
Articles were classified as empirical (8) and non-empirical (9). The research question targeted children with serious illness, which resulted in the majority of articles focussing on the following:
There were three papers which had non-specified or other foci.40–42
Study characteristics
Study type.

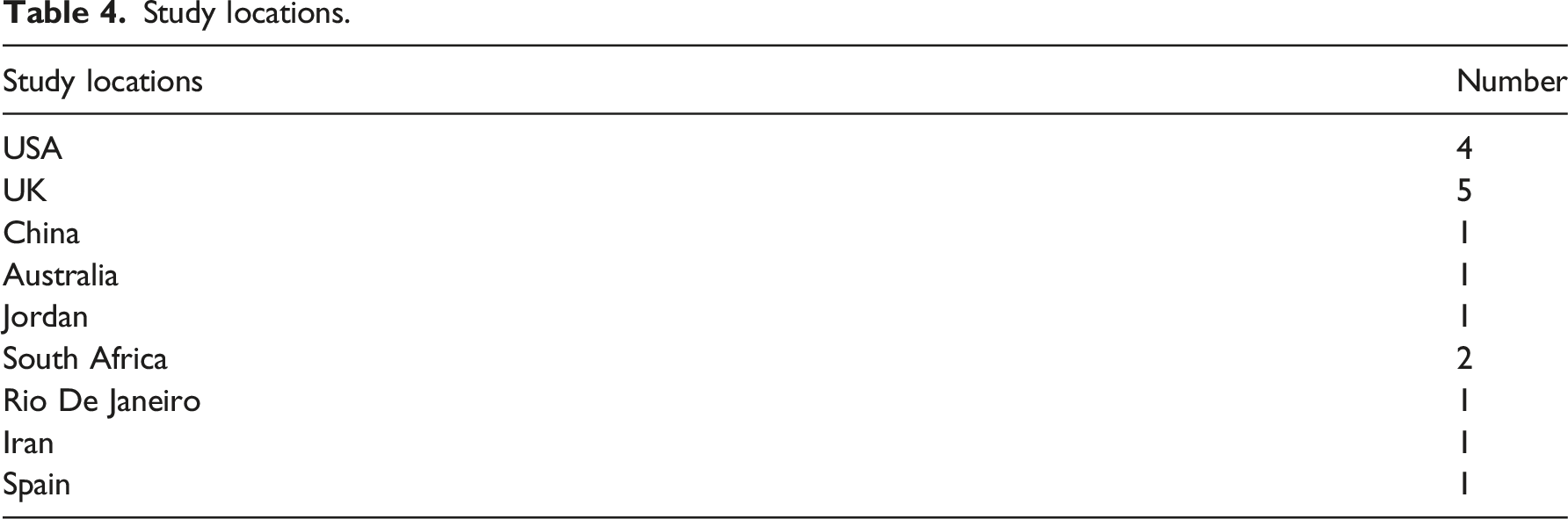
Study locations.
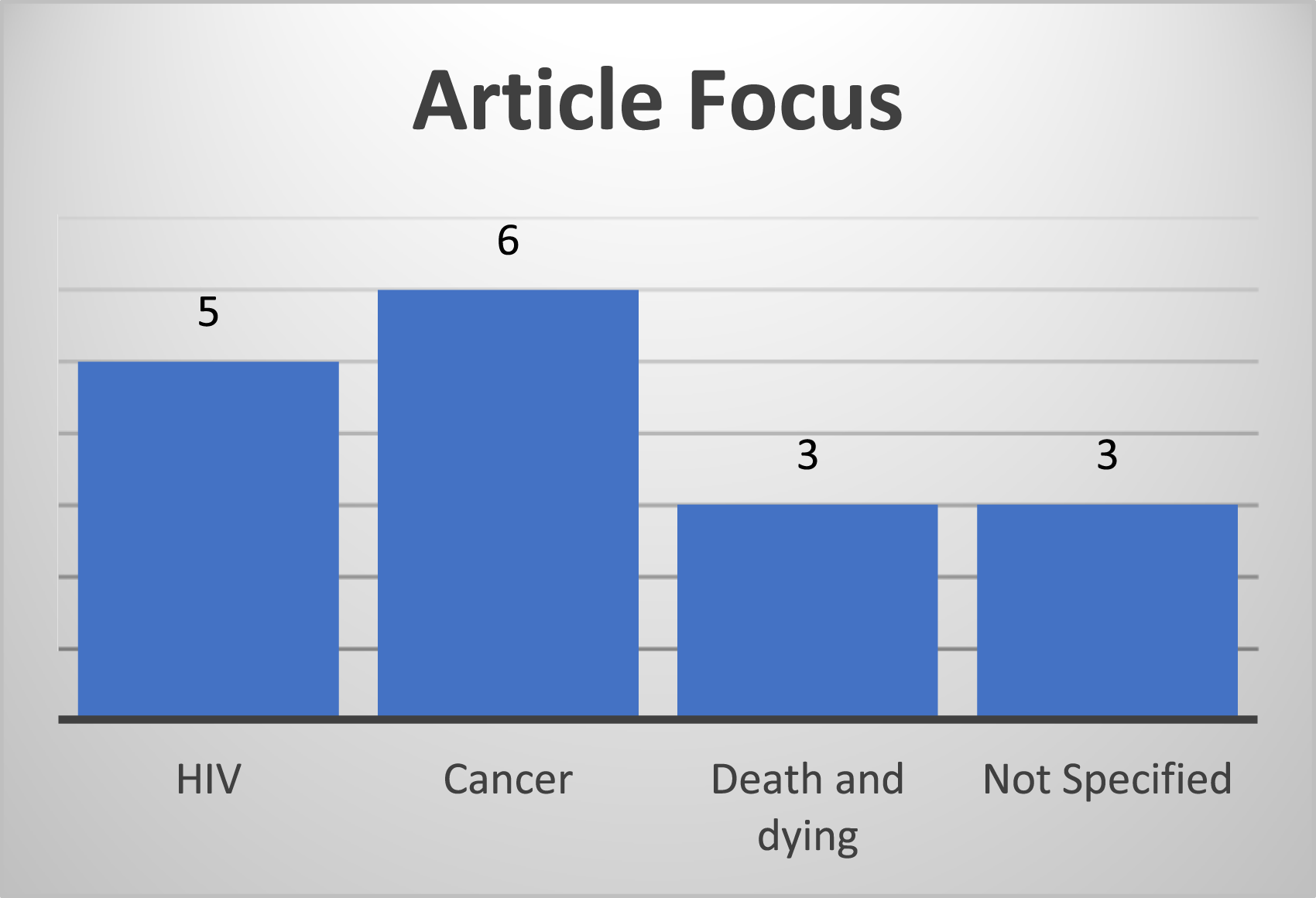
Article focus.
The thematic analysis of the included articles identified commonalities in the presented discussions. The themes identified include beliefs about: the role of the nurse in truth-telling; the nurses’ attitudes and beliefs regarding the ‘“if, when, and how to tell”; nurses’ beliefs about honesty – why children should be told and why children are not told; nurses’ experiences with cultural considerations in truth-telling; and nurses’ beliefs regarding cognitive considerations in truth-telling to children’.
The themes are closely related to each other, together representing the narrative or journey of the process of disclosure. For example, when a child presents to a clinical setting for investigation of a health issue, after a diagnosis is made, the ‘role of the nurse in truth-telling’ is believed by nurses to include support and advocacy for the child during the information sharing process. ‘If, when, where, and how’ the truth is told is influenced by the nurse’s experience, attitude and beliefs about information sharing and further shaped by the ‘nurses’ beliefs about honesty, – why children should be told and why children are not told’. The nurses’ experiences with ‘cultural considerations in truth-telling’ and beliefs regarding ‘cognitive considerations in truth-telling’ to children will then shape the transfer of information to children diagnosed with a serious illness. .
Nurses’ beliefs about their role in truth-telling
Clemente (2007), Myburgh (2018), and Watermeyer (2015) noted that as health care professionals, nurses spend a significant amount of time at the patient bedside, fostering a therapeutic relationship with the child and their family.30,36,39 The included articles interpreted the nurse’s role in truth-telling in the context of this relationship, seeing the nurse a support person for disclosures for information made by others.
The nurse’s role in truth-telling where there is a cancer and end of life care focus was seen as preparing the patient and family for receiving the news, reiterating and explaining the information initially conveyed by the physician and then supporting the child and family after they have received the news. 30 Similarly, there was a strong emphasis on the involvement of the nurse in supporting the truth-telling process to children diagnosed with HIV, but the articles do not describe or support direct participation by the nurse in the disclosure process. There was consensus in the publications focussed on HIV diagnosis that truth-telling to children about their HIV status was the responsibility of the child’s parent or guardian.35–39
The role of the nurse in HIV disclosure
Of the 17 included articles, five publications looked specifically at the role of the nurse in information sharing and truth-telling related to an HIV diagnosis.35–39 The studies, three of which were qualitative, looked at disclosure practices in HIV clinics. Nurses were described in five of the publications as essential in initiating and supporting the disclosure of HIV diagnosis to a child by the caregiver.35–39 Myburgh et al (2018) emphasised that it was routine practice and part of the nursing services in their clinics to support the caregiver with truth-telling practices to the HIV positive child. 36 Moura Bubadué and Cabral (2019) stated that HIV disclosure should be facilitated by parents due to the sensitivity and stigma associated with the method of HIV transmission.
There was a strong emphasis on the nurse’s role as advocate and support person in the disclosure process without the nurse being the person who directly communicated this information.35,37,38 Two studies found that participation by nurses in truth-telling to seriously ill children was not evident and nurses described an unspoken understanding that initial disclosure of new medical information such as a diagnosis or prognosis belongs to the physician as the authority figure; the nurses would be called in to support the parents and the information transfer process when required.37,39
The ethical discussions on HIV disclosure recognised that nurses have a moral responsibility to prepare, advocate, and support parents and caregivers through the disclosure process. 35
This included the preparation of families to disclose to their children, explaining the benefits and risk of disclosure to parents and caregivers, including any potential psychological outcomes and crucially, discussing the timing, method, and location of the discussion.35,37 Nurses were also described as having an instructional role in providing advice to parents and caregivers on how they should deliver the medical information to children without causing harm.
35
In the HIV clinical setting, nurses strongly advocated for HIV diagnosis disclosure to the child. Nurses described this as being a positive directive linked to promoting adherence to treatment and positive psychological support.
39
Nurses believed this knowledge acquisition empowered the child and protected their agency, consequently supporting patient autonomy, participation, and adherence to treatment.35,38 There were minimal ethical analyses within the HIV qualitative studies around parental non-disclosure. Discussions were clinically and practically focussed as opposed to presenting a philosophical argument as to what should be done if parents decided not to tell.36,38 However, Saunders does recognise this situation as an ethical problem stating that when asked to withhold an HIV diagnosis: “The nurse is, therefore, faced with the ethical dilemma of promoting disclosure in the best interests of the child and wider population or respecting the parents’ wishes for delaying disclosure.”
38
The nurse’s role in truth-telling in cancer care, death, and dying
Clemente (2007), Kendall (2006), and Renshaw (1979) described the nurse as a support person in the act of information transfer and truth-telling and in particular as the manager of the information pre, during, and after the child is told.26,30,33 Also evident in these articles was the emphasis on the nurse’s role in advocacy, counselling, and education in cancer care.27,30
In terms of advocacy, nurses were tasked with supporting the physician in the truth-telling process to children, ensuring the children as well as their families were given appropriate and satisfactory information26,27 while balancing the need to not oppose or dispute a physician’s decision on the matters of if, when, and how to disclose. 30 This role of child and family advocate was described as putting a strain on nurses’ interaction with the family. 30 Pursell argued that regardless of parents’ hesitancy to inform their child of their diagnosis, the nurse must find a balance between respecting the rights of the family while still ensuring the rights of the child were upheld. 32
Kendrick (1994) and Kendall (2006) described the fear associated with a cancer diagnosis (particularly in non-western cultures) as having a direct effect on the role of the nurse in truth-telling.26,41 Kendrick’s ethical analysis describes levels of deception within health care environments when difficult news must be conveyed. 41 The majority of deceptions were in the form of information omission. 41 In both cancer and HIV settings, there was an expectation that nurses are honest and forthcoming with information to the child; however, Kenrick noted lying and deception in the delivery of medical information occurred. 41 Kendrick saw this as problematic because trust is essential in the nurse patient therapeutic relationship and the presence of trust is dependent on the veracity of the nurse. 41 The therapeutic relationship itself was essential for the nurse to fulfil their role as support person and advocate in cancer care. 41
Nurses’ attitudes and beliefs about the ‘if, when where and how’ of telling
Clemente and Kendall (2007, 2006) both argued that for chronically ill children, the discussion should no longer focus on whether or not to tell the child, rather, how to tell, what to tell, and who tells.26,30 Due to advances in medical treatments, children with cancer or HIV are living longer with more positive treatment outcomes and can now be seen as having chronic illness, which makes the when, where and how questions about disclosure relevant.36,38
Regardless of the diagnosis, there was consensus that nurses play a significant role in guiding the disclosure process, and it will be specific to the child and the diagnosis. For an HIV diagnosis, and for children who are HIV positive as a result of vertical transmission, Myburgh et al (2018) stated that the disclosure process should be gradual, with information delivered systematically and in consideration of the child’s understanding. For children with cancer, Arabiat et al (2011) similarly argued that children should have the information communicated according to age, seriousness of diagnosis, and treatment types and stages. 27 Myburgh et al (2018) discussed implementation of disclosure guidelines based on the World Health Organization protocols within their health care facility in rural South Africa. The authors noted that these guidelines were not been validated and in many instances, the disclosure process actually implemented by the nurse may be influenced by the nurses’ own values, and belief systems.31,36
Nurses’ beliefs about honesty: Why children should be told and why children are not told
Clemente (2007), Kendall (2006), Kendrick (1994), and Shali et al (2020) discuss potential deceptive strategies such as telling half-truths, and not being forthcoming with information, being used by nurses and other clinicians when they believed the truth would receive a negative reaction.26,30,31,41 In an article published as part of a larger study, one nurse working in Hong Kong described caring for a terminally ill child, whose parents requested a non-disclosure of the child’s cancer diagnosis. 26 In this instance, there was a discussion about how the deception would maintain hope and that it would be better for the child if they did not know. The nurse admitted ‘I learned to tell a lie sometimes’. 26 Monaghan (2012) described the request to withhold diagnostic information from a child as ‘lying’ and ‘deceitful’. 28 Kendrick presented a case where parents refused to allow the truth to be told to their terminally ill daughter and the health care staff participated in withholding this information. Kendrick regarded this as ‘collusion’ (1994, p. 676). The parents in this situation acted with beneficent intent; however, nurses felt this directive went against their moral obligation of veracity. 41 Shali et al (2020) presented a qualitative study where nurses defended their acts of clinical deception by the argument of beneficent intent. Shali et al (2020) concluded that nurses frequently lied to children in their care, depending on the situation presented to them. 31 Some of the reasons for the deception described by the participants in Shali et al’s study were: the technicality of the information presented, reduction of the child’s fear, and the discomfort felt by the nurses in conveying the bad news. 31 Shali et al’s study was undertaken in Iran where cultural influences impacted how and what information was communicated to the seriously ill child. 31 Regardless of the beneficent intent, the authors of all three studies emphasised the importance of honesty in all aspects of clinical communication.28,31,41 Care modelling which is strongly focused on a patient centred approach, adopts honesty in therapeutic communication as best practice.28,41 The domino effect of truth-telling is the building of trust, compliance to treatment, and participation in care. 28
The discussion around deception in communication from the nurses in these publications can be approached from a deontological ethical theory perspective, where, as expressed by Clemente and Shali et al, the nurse has a duty of care to provide the truth to the patient and any act of deception is morally reprehensible.30,31 Kendrick ethically analysed instances where lying can be morally justified, however reiterated that a lie is a lie and should not be regular practice, rather the lie can only be acceptable on rare occasions. 41 Kendrick stated ‘terms such as “to be economical with the truth” are a moral smokescreen and do not negate the moral weight of a lie’. 41 Doyle and Maslin-Prothero et al (1999) took a similar view to Kendrick, saying that lying is synonymous with breakdown of a trusting therapeutic relationship and dissolves the advocacy role of the nurse in ensuring the child’s right to their own medical information.40,41 Honesty is integral to a nurse’s work and supports integrity in nursing practice. 29
The papers about HIV suggested specific reasons why parents and care givers withheld the truth. Despite advances in HIV therapies, the stigma of HIV remains. Dependant on the child’s age, the potential psychological impact of being told the truth can be significant. There is then the parents’ or guardians’ fear the child may unintentionally disclose their HIV status to someone within their community as they do not understand the sensitive nature of the diagnosis and how far the negative impact of the disclosure will extend.36,38 The stigma of HIV was cited by Nehring (2000) as potentially impacting the ‘child’s quality of life’ due to the ‘fear of rejection’ as a consequence of the diagnosis.37–39 Lack of knowledge and tools to facilitate the disclosure process, and the lack of emotional preparation were also discussed as reason for withholding the truth. 39 Parents’ denial about their own HIV status was cited as another reason they chose to withhold the information. 39
A key reason suggested for not disclosing the truth of the cancer diagnosis to the child was that it would cause fear in children. 31 Parent–centred reasons for non-disclosure were also noted, including fear of the impact on family relationships and the lack of tools to deal with the reaction by the patient to the truth, as parents wanted to protect their child but were often fearful of the truth themselves.26,34 Kendall (2006), Clemente (2007), and Arabiat (2011) observed that limited truth-telling is a protective measure and coping mechanism for families of seriously ill children. It offers a maintenance of the status quo by ensuring the diagnosis is not the centre of their family functioning.26,27,30
Other reasons presented for not telling the child the truth were simply that the
The thematic analysis identified publications that discussed some of the reasons why HIV diagnosis should be disclosed to the children. As previously mentioned, the advances in HIV therapies have granted longer and better quality of life to HIV positive patients; however, treatment outcomes are strongly reliant on compliance by the patient. Hence, children need to understand the nature of their illness to comply with treatment.35,36 It was noted that non-disclosure of an HIV positive status can be a risk to public safety as the child enters adolescence and becomes sexually active, hence telling the child the truth could prevent the spread of the infection. 38
Myburgh et al (2018) and Saunders (2012) agreed that the child’s knowledge of their HIV status had positive health outcomes both physically and psychologically.35,36,38 By approaching truth-telling systematically, whilst considering cultural and cognitive factors, learning the truth about their HIV status could have overall positive effects on the child’s health status. 36 These include compliance with treatment, psychological wellbeing, and the development of a trusting relationship with their carers and health professionals.35,36
Psychological impacts were similarly discussed in relation to truth-telling practices in cancer care. 28 Participation in and assent to treatment by the child was noted as a reason to ensure they were afforded the truth about their cancer diagnosis.28,34 Despite diverse cognitive abilities and ages in paediatric care, Monoghan (2012), Clement (2007), and Stayer (2012) argued that children still had a level of understanding and had a right to information about their own health care.28,30,34 According to Kendrick, withholding the truth of a poor prognosis, particularly for pre-adolescents could have significant negative psychological impacts and deny the child the opportunity to prepare for end of life. 41
Nurses’ beliefs that children already know
With all the discussions around whether or not to disclose medical information to children, there was a common suggestion that in many instances nurse believed children were already aware of their illness or impending terminal prognosis.30,32,37,38,40 Doyle and Maslin-Prothero (1999) described how nurses believed children had a sense that something was wrong. In instances where information was not forthcoming, there were potential negative ramifications, specifically on the trust and therapeutic relationship between the child and health care team. 40 Pursell stated that when children were aware of their health status, it was difficult for nurses and doctors to lie to them. 32 Clemente (2007) and Doyle & Maslin-Prothero (1999) explained that nurses believed that the reasons children did not acknowledge their awareness of their illness and prognosis were aligned with the reasons parents did not want their children know. Namely, children understood that their parents found comfort in believing their children were unaware of their own diagnosis and prognosis. In parallel with their parents, children concealed their awareness of their diagnosis as a protective factor for their parents allowing them the continuity of their carer status in the relationship.30,40
Nurses’ experiences with cultural considerations in truth-telling
An outcome of the review was the number of non-western publications describing the limit of truth-telling based on cultural influences and practices. When describing best practice for truth-telling in the paediatric clinical setting, emphasis was placed on ensuring nurses demonstrate cultural safety through the exploration of normal cultural and religious practices for individuals in their care.26–28,31
The review demonstrated a diversity in disclosure practices across developed and developing countries. Clement (2007), in describing disclosure practices to children diagnosed with cancer in Spain, stated that more than two thirds of patients’ relatives are opposed to their loved one knowing the truth. 30 Clement (2007) articulated that patients themselves don’t want to know the truth and this is demonstrated by only a small portion of cancer patients being fully informed. 30 Arabiat (2011) and Shali et al (2020) suggest Middle Eastern truth-telling practices, to children diagnosed with a serious illness and who receive a poor prognosis consisted of withholding information or a distortion of the truth through omissions, deceptions and white lies in paediatric settings.27,31 In Greece, nurses believed that only the relatives should be told about a child’s cancer diagnosis to avoid causing psychological harm, but admitted it was essential for patients to know the truth in order to support a positive therapeutic relationship. 26 It is not unusual, according to Kendall (2006), for patients with a Chinese background to withhold the truth about a child’s diagnosis from the child. 26 Kendall suggested that this is because in China, the good of society and family is prioritised over individual needs.26,27,30 Adding to the challenges were cultural taboos regarding topics involving sex. Watermeyer (2015) stated children with HIV for example who reached adolescence and should have been told about their HIV status due to the risk of safety in sexual practices were not told, as sex talk was considered taboo in some cultures. 39
Nurses’ beliefs regarding cognitive considerations in truth-telling to children
Developmental and cognitive considerations were a common theme. Again, there were many similarities between the two major illnesses discussed – HIV and cancer, but slight variances as to the timing and sensitivities of the disclosure.
All the publications discussing HIV studies agreed that information should be transferred in line with the emotional and cognitive maturity of the child.28,35 Moura Bubadué and Cabral’s (2019) study on disclosure advocacy for children with HIV, stated that in the South African community where the studies were conducted, the recommended age to disclose HIV to affected children is about 10, when they have sufficient cognitive capabilities to comprehend the sensitive topic and in a way that is sensitive to the potential harm that may be inflicted. 35 Kendall, (2006) described the complexities in communicating with children about death and advised communicating medical information in the child’s language. 26 None of the publications in this review identified any validated framework or model that provided guidance on appropriate, ages, methods, or timings of disclosure. There was no exact agreement on the appropriate age for disclosure but most described toddlers and pre-schoolers as not needing a lot of information about their condition.27,37 It was agreed however, that adolescents should be told the truth about their condition.27,37 Two papers noted that waiting to disclose HIV status until adolescence could have a significant negative affect on the adolescent potentially triggering a grieving process, due to the sudden acquisition of knowledge and full understanding of the condition and its implications.37,38 These two papers suggested that a gradual process of information transfer starting in pre-adolescence was more desirable.37,38
Discussion
The focus of this review was to look at the experiences attitudes and beliefs of nurses with regards to truth-telling to seriously ill children. In interpreting the results of the review, the key points that emerged are that: there was consensus across the diverse settings regarding the importance of honesty; nurses play a supportive, rather than an active role in the truth-telling process; nurses have sensitivity to parents reasons in non-disclosure including fear, cultural, and cognitive considerations; nurses experience a moral dilemma when asked not to disclose and that there is an ethical conflict in the concepts of beneficence and non-maleficence when implementing a non-disclosure directive.
The described role of the nurse provides insight into how nurses are involved in truth-telling and the process by which this is undertaken within a health care setting. The included studies indicate that nurses do not play an active role, but rather a supportive one in the disclosure and truth-telling process.30,31,35–37,39 The information nurses are able to convey is limited by the wishes of the parents including what, when, where, and how much they want their child to know.
An important point emerging from the review is the nurse’s sensitivity to parental fear as a reason for non-disclosure. The reasons for fear slightly varied between cancer and HIV studies, but the concept of fear was consistent. For HIV, it was fear of the stigma, fear of a parent’s own HIV status, and fear that the child would disclose to others due to their lack of understanding of their diagnosis.36–38 For a cancer diagnoses, the fear of the child not being able to cope with the information and the parents own self-protective measures were the reasons for parental decisions of non-disclosure.26,31,34 However, there was no discussion of how nurses might help parents to address or alleviate their fears in other ways. Cultural considerations played a significant role across both HIV and Cancer diagnoses with regards to how and if information was conveyed to the child.30,31,35,43 Some cultural beliefs did not support truth-telling to seriously ill children.
There was consensus that telling the truth to children had a positive psychological and physical effect as it supported assent and compliance to treatment across both cancer and HIV diagnoses.35,36,38,44
The most significant of the themes that emerged through the analysis was the nurses beliefs around honesty.31,41,44 A therapeutic relationship between the nurse, patient, and family is born from trust which is based on honesty.
45
Honesty as a virtue is essential in the nurse–patient therapeutic relationship; however, the concept of honesty can be complicated in clinical scenarios when referring to best practice.46,47 While the ethical discussion papers referred to honesty as a key value or virtue, there was a lack of critical analysis of the complexities presented in the clinical setting when factoring in a diagnosis of a serious illness, and the diverse needs of children and families. To understand these complexities, the following questions should be explored. 1. Is withholding of information distinct from lying, 2. What are the nurses’ beliefs about honesty? 3. In what circumstances do parents give a non-disclosure directive 4. What role does fear, stigma, and the desire to protect a child play in withholding the truth? and 5. Is honesty indeed best practice?
47
All these issues need further academic exploration.
A mixed methods study by Newman et al (2019) investigated prognosis related communication in the oncology setting. 48 The qualitative portion of the study found that despite open communication the information relayed to children was not free from deceit or fraud. 48 Nurses conveyed that they were ready to fully participate in disclosure and information sharing; however, the language that the nurse often used to convey medical information to parents, children, and their families was not always direct and concise and was sometimes shrouded in falsities and vagueness, often omitting important aspects of the truth with the intent of giving false hope. 48
A strong message arising from the papers in this review is that the institutional practices of information disclosure in the hospital setting make truth-telling to children a fraught matter for nurses. Nurses play a secondary role in information delivery. What the nurse is allowed to disclose will depend on the primary discussion that is usually held between the physician and the parents. Nurses often prepare the families before this discussion, and frequently provide support afterwards, but they are not involved in making decisions about what information, or how much of the truth, is communicated to the child. The above described ‘disclosure workflow’ sequence is represented in the following figure (Figure 4): Disclosure workflow.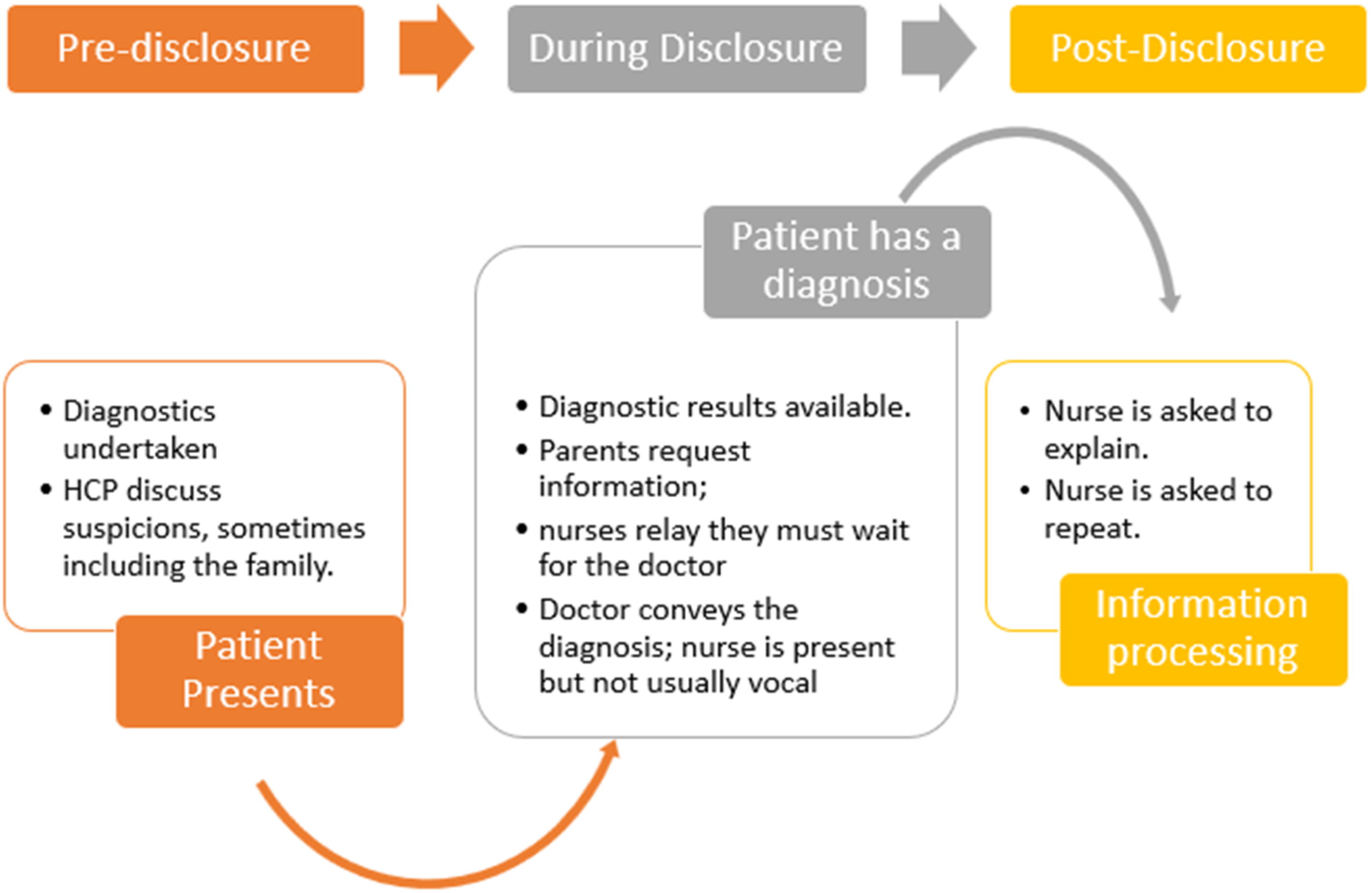
The amount of information shared is at the discretion of the parents and the physician; and nurses typically end up being complicit in whatever decision is made, either full disclosure or withholding of information.
When analysing the application of the principles of biomedical ethics several papers present ethical justifications for acts of both honesty and deception in communication.29,32,41,42 Kendrick (1994) presents a utilitarian and deontological ethical analysis related to the moral justification of lying in the clinical setting. 41 Two hospital-based scenarios are presented, one in which a patient is hospitalised after being physical abused by her partner and the nursing staff lie to the partner about her location when he presents looking for her. 41 The second is in reference to a 16-year-old girl who is dying and whose parents give a non-disclosure directive. In the first scenario, a utilitarian justification is given to support lying to the partner regarding the patient’s location – the end justifies the means, and the lie will protect the patient. 17 In the second scenario, a clear deontological perspective is presented that indicates a lie is a lie and always wrong, so honesty is always best ethical practice. 17 To highlight the ethical complexities of truth-telling, Kendrick asks ‘If telling the truth leads to harm, should we tell a lie to try and promote beneficence?’ 41 Kendrick (1994) then argues that lying can sometimes be morally justified. 41 Pearson (2006), Purssell (1994), and Shali et al (2020) present similar discussions with Shali et al describing the practice of white lies as being common in clinical practice.31,32
Martinez (2021) and van Straaten (2000) ethically justify the withholding of information, the deception, falsities, and white lies which are presented as protective measures to overt fear and to allow for hope. There is a lingering belief that hope and fear are tied to the possession of the knowledge of the illness.9,10 However, when considering the best interest of the child, application of the bioethical principles of beneficence and non-maleficence can be subjective, with different people holding different views, including nurses. While a child’s parents may withhold the truth from the child with the intention of maintaining a level of hope for recovery or cure, or holding the belief that the child is unable to process the information emotionally or cognitively, health care professionals and importantly nurses, may believe the sharing of medical information with the seriously ill child within the realms of their cognitive ability would actually be more beneficial to child. There is evidence that children do better psychosocially when they receive an age-appropriate explanation of what is happening to them and why. 49
One of the more significant reasons for the support of disclosure and honesty in medical information sharing to children hospitalised with a serious illness is assent and compliance to treatment, particularly for patients diagnosed with HIV. The participation of children in their own health care is supported by the principle of respect for the child’s developing autonomy.17,31,50 Participation, decision-making and the level of truth-telling, and honesty is related to a child’s cognitive capabilities.13,16,35,38 The review demonstrated consensus in both cancer and HIV settings that in order to support a child’s participation in their own healthcare, nurses should advocate for honesty. The papers included in the review demonstrated appropriate use of the wider ethics literature to inform their discussion of information disclosure to children; however, the included articles don’t use this to provide ethical guidance for nurses about truth-telling in practice, even in relation to how to manage a non-disclosure directive. The nurses’ experiences, attitudes, and beliefs therefore support advocacy for honesty and disclosure, yet nurses have no validated guidance of how this can ethically be addressed considering the culturally and cognitively diverse paediatric patient population.
According to Pearson (2006), on moral grounds, a nurse can refuse to carry out the instruction to lie to the patient. Despite their position in the medical hierarchy, the physician is not within their rights to make a nurse lie. 29 However, the papers included in this review do not challenge the overall clinical communication hierarchy in the hospital. It was clear through the review that the physician as the authority figure is the conveyer of the diagnosis or other diagnostic and treatment information while the nurse in any disclosure setting is the shadow that supports the practice. Indeed, Arabiat et al (2011) expressed the view that nurses ‘should not have an opinion’ on the child’s access to information but rather should simply facilitate communication between mother and child (p. 443). The disconnect between the nurses’ attitudes and beliefs about truth-telling to seriously ill children, and their actual experiences was a common observation in examined articles, as was variation in their own understanding of their discipline and scope of practice in relation to the role of physicians in information transfer. The lack of specific guidelines or policy warrants further work in nursing ethics to address the differing views on this issue.
Implications for policy and practice
Considering the significant roles nurses play in the care of children and their families, it is reasonable to assume they also play a significant role in communicating information to these families. Hence, it is also reasonable to question why nurses are not active participants in the sharing of medical information to seriously ill children. After all they are well placed to modify information delivery to meet the needs of the child and family. As noted above, a clear message from this review is that the institutional practices of information disclosure in the hospital setting make truth-telling to children a fraught matter for nurses. These practices need to be reviewed, to be more inclusive of nurses at all stages of truth disclosure, and to make it less fraught for nurses to be honest with children. The provision of guidelines on information disclosure and truth-telling for nurses caring for children would be another important step. Guidelines would support nurses who are presented with a non-disclosure directive to acknowledge and respect the diversity among families of hospitalised children, while also promoting the rights and best interests of the child.
Strengths and limitations
The strength of the review is in its rigorous and comprehensive search strategy, aimed at finding all relevant articles, and the rigorous screening process undertaken individually and independently by the authors, to ensure that irrelevant and poor quality articles were not included. The inclusion of non-empirical publications was a deliberate decision, based on content within relevant to the review question. However, this meant that the review did not meet the strict definition of a systematic review. Nevertheless, it demonstrates the same processes for rigour19,51,52 as a systemic review in that: 1. There was a clear research question. 2. The methods and methodology were transparent and replicable. 3. Inclusion and exclusion criteria were stipulated. 4. A comprehensive search strategy was undertaken. 5. A quality assessment of the included articles was undertaken. 6. A systematic analysis of included articles was performed. 7. Findings were presented in detail and synthesised.
A potentially significant limitation to this review was the keywords used to find publications which addressed the question for the literature review. The terms ‘truth-telling’ and ‘disclosure’ may not have captured all relevant papers but adding the broader term ‘communication’ produced an extraordinarily high number of results, completely unmanageable to screen within our resources. The phenomenon we are interested in may not be delineated well by keywords and MesH terms in current use. It is also possible that some papers that contained relevant content were missed because the keyword ‘nurse’ or ‘nursing’ was not nominated by the authors, even though the paper referred to nurses’ experiences attitudes and beliefs.
Conclusion
Despite the length of time nurses spend at the patient’s bedside, little consideration has been given in the literature to the role the paediatric nurse plays in the day to day transfer of information in clinical setting. This is significant because nurses are well placed to be on the receiving end of questions posed by paediatric patients hospitalised with serious illnesses. This review demonstrated a paucity of literature exploring the experiences, attitudes, and beliefs of nurses with regards to truth-telling to seriously ill children. The publications that met the inclusion criteria focused mainly on medical information about cancer, HIV and death and dying as focal discussion points. Other medical conditions were not addressed. This lack of a comprehensive picture of what truth-telling issues arise in practice for nurses across the full range of paediatric nursing fields is problematic. Further to this, no publications explored nurses' practices in telling or hiding the truth about nursing interventions – the focus was only on information seen to belong to doctors, such as diagnosis and prognosis. This means that the current literature gives no solid basis for providing sound ethical guidance for nurses, in their education or their practice settings. The findings of this review highlight a need for further research to be undertaken to explore the experiences, beliefs, and attitudes of nurses to information sharing to children hospitalised with a wide range of serious illnesses and in diverse clinical scenarios.
Supplemental Material
Supplemental Material - Truth-telling to the seriously ill child – Nurses’ experiences, attitudes, and beliefs
Supplemental Material for Truth-telling to the seriously ill child – Nurses’ experiences, attitudes, and beliefs by Mandy El Ali, Sharon Licqurish, Jenny O'Neill, and Lynn Gillam in Nursing Ethics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.