
Abstract
Background
Nurses provide care to meet the complex needs of patients in the increasing workload in the health system and are at risk of compassion fatigue. The concept of compassion fatigue has begun drawing attention in the last decade, as it negatively affects nurses' physical and mental health, job performance and satisfaction, and therefore patient care quality.
Objectives
This study was to examine compassion fatigue and predictive factors in paediatric surgery nurses.
Participants and research context
The study was cross-sectional, predictive and quantitative. It was conducted with the 135 paediatric surgery nurses. The data were sent to the email addresses of the members via Google Survey. Research data were collected with the Nurse Information Form, Compassion Fatigue Scale, Life Satisfaction Scale and Multidimensional Perceived Social Support Scale.
Ethical considerations
After obtaining the approval of the University’s ethics committee, the study was carried out after obtaining participants’ informed written and verbal consent.
Results
There was a difference between the level of compassion fatigue according to the paediatric surgery unit that worked the longest and the thought of changing their profession. Burn unit nurses and nurses who were considering changing professions have higher compassion fatigue scores. When the predictors of compassion fatigue were examined, the thought of changing the nursing profession and life satisfaction were significant predictors of compassion fatigue. The thought of changing the nursing profession and life satisfaction explained 22% of compassion fatigue. The same variables and the longest working period of the paediatric surgery unit were the estimators of the level of occupational burnout; explaining 29% of occupational burnout.
Conclusions
Compassion fatigue, life satisfaction and perceived social support of paediatric surgery nurses are moderate. Compassion fatigue is affected by working time, the thought of changing the profession, life satisfaction and perceived social support.
Keywords
Introduction
Nurses, the largest and most critical group in healthcare, play a pivotal role in meeting the complex needs of patients within the growing demands of the healthcare system. However, they are also susceptible to compassion fatigue (CF), which manifests as an inability to cope with emotional stress. Prolonged exposure to suffering individuals can result in emotional, physical and mental exhaustion. This concept, which has been around for the past 30 years, has surfaced as a contributor to post-traumatic stress syndrome in caregivers.1–3 Figley, in particular, has developed the concept of CF into a well-defined theory. According to Figley, CF is defined as ‘a state of biological, physiological, and emotional exhaustion and dysfunction because of exposure to long-term compassion stress’.3–5 Figley views CF as the ‘cost of caring’. It arises as a natural consequence of witnessing individuals in suffering or pain. Another definition characterises it as the stress that results from trying to assist someone, especially a loved one, who has experienced a traumatic event. 6 Figley (1995) identified two key contributors to CF: empathy and exposure. Without these elements, the risk of an individual developing CF is minimal. Concerning exposure, it is well-known that nurses, due to the nature of their work, are continuously exposed to the emotional states of dependent patients. This work takes a toll on nurses, affecting their psychosocial and physical well-being. Nurses in different specialities are particularly susceptible to work-related stress. Furthermore, healthcare professionals find it particularly difficult to detach themselves from the suffering of others. Neglecting self-care in favour of caring for others can lead to stress, burnout or CF. 6 Compassion satisfaction (CS) and CF can also affect nurses’ overall life satisfaction. 7 Levels of CS are decreasing, while levels of CF are increasing. This trend can negatively affect nurses’ life satisfaction, staff retention, organisational capacity and the provision of holistic care while increasing the risk of adverse events. 8
Although compassion is considered a core aspect of nursing, the literature regarding its characteristics, causes, frequency and effects on nursing practice is scarce. 4 CF has gained attention in the last decade because of its detrimental effects on nurses’ physical and mental health, job performance, job satisfaction, and consequently, the quality of patient care.2,9,10 CF erodes nurses’ innate capacity for compassion and hampers their ability to alleviate suffering. It impacts nurses’ overall well-being, spanning physical, emotional and social dimensions. 5 This gives rise to substantial ethical concerns in the caregiving field, as the well-being of nurses and their ability to provide compassionate care are inherently intertwined. 3
CF in the literature is closely linked to concepts such as burnout, traumatic stress, moral distress, indirect traumatisation, post-traumatic stress disorder, secondary traumatic stress and CS. 2 In a study involving 30 paediatric ICU nurses and 30 paediatric oncology nurses, both groups experienced CF, had low levels of CS and suffered from moderate to high levels of work-related stress. Notably, the paediatric ICU nurses exhibited higher average burnout levels than the paediatric oncology nurses, indicating significant work-related stress among nurses working with paediatric patients, which contributes to CF and subsequent burnout. 11 Another study in China with 44 participants revealed that work-related stress and perceived social support moderately and directly influenced burnout. Job stress also had a direct effect on perceived social support and self-efficacy. 12 Another study examined the relationship between CF, burnout, CS and social support among nurses. The results indicated that CF had a positive effect on burnout, while social support and CS had negative effects on burnout. However, social support and CS did not mitigate the effects of CF on burnout. 13 In a Turkish study of 336 nurses, a negative relationship was observed between CF and the nurses’ attitudes toward life, while work-related stress showed a positive correlation with CF. 14 Additionally, a study involving surgical nurses in Türkiye reported high levels of CF and care satisfaction, revealing a positive and strong relationship between CF and care satisfaction. It is worth noting that paediatric surgical nurses were not included in this study, and CF levels were not assessed by specific units. 15
Paediatric surgical nurses are particularly susceptible to CF due to their exposure to the emotional challenges associated with pre- and postoperative trauma, and the stress, pain and empathy they feel for their patients.16,17 The demanding working conditions and patient-related risk factors, such as rapid patient discharge, high caseloads, exposure to children’s pain and traumatic experiences, interactions with families, workload and time constraints, contribute to CF. In units with fast-changing patient populations, such as day surgery, high ICU patient volumes and limited time for nurses to care for children and families in specialised units (such as burns) can lead to emotional and physical exhaustion among nurses. Paediatric surgical nurses often witness the pain and traumatic experiences of their young patients, triggering empathy and exposure, as noted by Figley. Nurses can become emotionally drained when responding to children’s pain and trauma. Additionally, paediatric surgical nurses are tasked with supporting not only their patients but also their families. Managing the anxiety, stress and expectations of families can further increase the workload of nurses. It can be ethically challenging to balance the wishes and expectations of families with children in care. Beyond medical procedures, paediatric surgical nurses must juggle multiple responsibilities, such as providing psychosocial support, communicating with families and educating them. This workload and time pressure can contribute to their emotional and physical exhaustion. 16
These factors heighten the risk of CF in paediatric surgical nurses. Ensuring that nurses have access to adequate support and resources is critical to maintaining their emotional well-being and improving patient care. In addition, it is important to address the ethical aspects of nursing and patient care, emphasising the need for an ethical review of these factors.
A review of the literature identified studies on CF in neonatal ICU nurses, 16 paediatric nurses, 17 acute care nurses, 18 oncology nurses 19 and ICU nurses, 20 but no study examining CF and predictive factors in paediatric surgical nurses was found. However, in a systematic review, Salmond et al. stated that there are deficiencies in explaining the concept of CF. 21 Our study is the first study in Türkiye to examine CF in paediatric surgical nurses; it is believed that it will contribute to explaining CF and provide valuable insights into the ethical implications for care. 3
This study aimed to examine CF and predictive factors in paediatric surgical nurses.
Research questions: 1. What is the mean level of CF among paediatric surgical nurses? 2. Is there a difference between the mean CF scores of paediatric surgical nurses according to their years of experience? 3. Is there a relationship between CF and life satisfaction in paediatric surgical nurses? 4. Is there a relationship between the CF of paediatric surgical nurses and their perceived levels of social support? 5. What are the factors that predict the CF of paediatric surgical nurses?
Methods
Design
This was a cross-sectional, predictive and quantitative study.
Participants and sample size
This research was conducted with the Association of Paediatric Surgical Nurses. The Association of Paediatric Surgical Nurses was established on 5 May 1998 by the Paediatric Surgical Nurses of Ege University Medical Faculty. The association has approximately 250 members. The sample of the study consisted of paediatric surgical nurses. The aim was to reach all members of the Association of Paediatric Surgical Nurses, and an email was sent to all members. Additionally, members reached by snowball sampling were asked to pass the information on to their colleagues in paediatric surgery. In this way, 135 nurses were included in the sample.
Study inclusion criteria: • Working in one of the paediatric surgical units • Holding a bachelor’s degree • Able to read, write and speak Turkish.
At the end of the research, the sample power was calculated by performing power analysis in G*Power version 3.9.1.2. 22 It was determined that the effect size was 0.89 and the sample day was 0.99. The power analysis was made according to the difference between the mean scores of CF according to the thought of leaving the job.
Data collection
Data were collected between February and October 2022. The data were sent to members’ email addresses via Google Surveys. Research data were collected using the Nurse Information Form, Compassion Fatigue Scale, Life Satisfaction Scale and the Multidimensional Scale of Perceived Social Support.
Nurse information form
There are 14 questions in this form, designed by the researchers. It contains questions on age, gender, marital status, number of children, level of education, unit most worked in, years working in unit and profession, working style, willingness to choose the profession, thoughts on changing profession, the satisfaction of working with the nursing team and the satisfaction of working with other members of the team.
Compassion fatigue-short scale
This scale was developed by Adams, Boscarino and Figley (2006) 23 to measure the level of CF in healthcare workers. The Turkish validity and reliability of the scale were determined by Dinç and Ekinci (2019). 24 The scale is a 10-point Likert-type scale with 13 items, including secondary trauma and burnout sub-dimensions. Items c, e, h, j, l in the scale refer to secondary trauma; a, b, d, f, g, i, k, m items measure occupational burnout. The lowest score that can be obtained from the scale is 13, and the highest score is 130. The scale has no scoring algorithm and no cut-off point. As the score on the scale increases, so does the CF experienced by the participants. The Cronbach’s α coefficient for the Compassion Fatigue-Short Scale is 0.876; 0.748 for the secondary trauma sub-dimension and 0.852 for the occupational burnout sub-dimension. As scores on the scale increase, so does the level of CF experienced by the individual. 24 In this study, the Cronbach’s alpha coefficient for the total scale was 0.87; 0.81 for the secondary trauma sub-dimension and 0.86 for the occupational burnout sub-dimension.
Life satisfaction scale
This scale was first developed by Diener, Emmons, Larsen and Griffin (1985). 25 The scale’s validity and reliability in Türkiye were confirmed by Dağlı and Baysal in 2016. The Cronbach’s alpha coefficient of the scale was 0.88, and the test-retest reliability was 0.97. This scale, which has a single-factor structure, consists of five items and has a five-point Likert (1-strongly disagree‒5-strongly agree) structure. 26 In our study, the Cronbach’s alpha of the scale was 0.87.
The multidimensional scale of perceived social support
The multidimensional scale of perceived social support was developed by Zimmet et al. in 1988, 27 adapted into Turkish by Eker and Arkar (1995) and revised by Eker et al. in 2001. 28 Work has been done on this scale. The multidimensional scale of perceived social support consists of 12 items that subjectively assess the adequacy of perceived social support from three different sources: family, friends and a special person. Each item is rated on a 7-point Likert scale. The subscale score is obtained by adding the scores of the four items in each subscale, and the total scale score is obtained by adding all the subscale scores. A high score indicates a high level of perceived social support. The reliability test of the scale revealed that Cronbach’s alpha values were between 0.80 and 0.85, and the scale and subscales showed acceptable internal consistency. 28 The Cronbach’s alpha of the scale in this research was 0.93.
Ethical considerations
To conduct the research, necessary permissions were obtained from the non-interventional ethics committees of the university, the Paediatric Surgical Nurses Association and the nurses participating in the research.
Data analysis
IBM SPSS (Statistical Package for the Social Sciences) Statistics 25.0 was used to analyse the research. Number and percentage analyses were used for descriptive characteristics. The normal distribution of the data was evaluated using Kolmogorov–Smirnov, Shapiro–Wilk and Kurtosis-Skewness tests. The significance level was determined as p < 0.05. The relationship between the mean scores was evaluated by Pearson correlation analysis; the difference between the mean scores according to the socio-demographic variables was evaluated with two mean or two significance tests of the mean in more than two groups. Multivariate linear regression analysis was used to examine the factors predicting CF in paediatric surgical nurses.
Results
Investigation of compassion fatigue scale and its sub-dimensions according to socio-demographic and clinical variables.
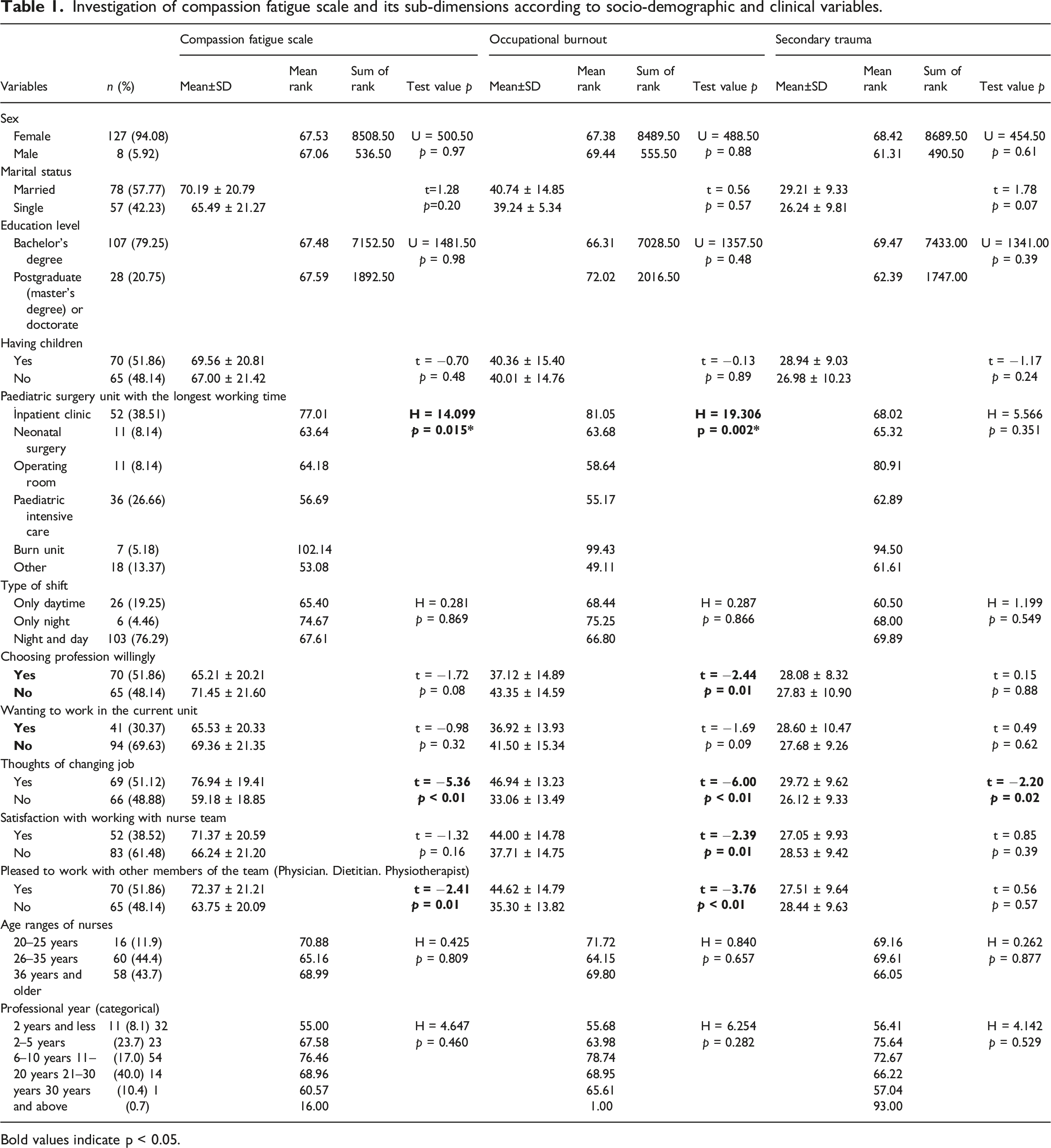
Bold values indicate p < 0.05.
There was no difference in the CF scores according to gender, age, years of experience, marital status, level of education, having a child, working style (shift), choice of profession, thoughts of changing profession and satisfaction with the team they work for. There was a difference in CF points according to the paediatric surgical unit where they had worked the longest and their thoughts on changing their profession. Nurses working in the burn unit and nurses who were considering a career change had higher CF scores (Table 1).
When the sub-dimensions of the CF scale were examined, it was found that there was a difference in the occupational burnout sub-dimension according to the paediatric surgical unit where they had worked the longest, choosing the profession voluntarily, having the idea of changing professions, being satisfied with the nursing team one works with and being satisfied with working with other members of the team (Table 1). Burnout scores were high for nurses working in the burn unit, those who had not chosen their profession voluntarily and those who were thinking of changing their profession. Nurses who were satisfied with their nursing team and with other members of the team also had high professional burnout scores (Table 1).
When the variables in the other sub-dimension of the CF scale were examined according to the secondary trauma sub-dimension, only the mean score of nurses who had thoughts of changing careers was significantly higher (t = −2.20, p = 0.02). There was no difference in the mean scores of the secondary trauma sub-dimension regarding the other variables.
Investigation of the relationship between compassion fatigue scale and its sub-dimensions. Life satisfaction and perceived social support.
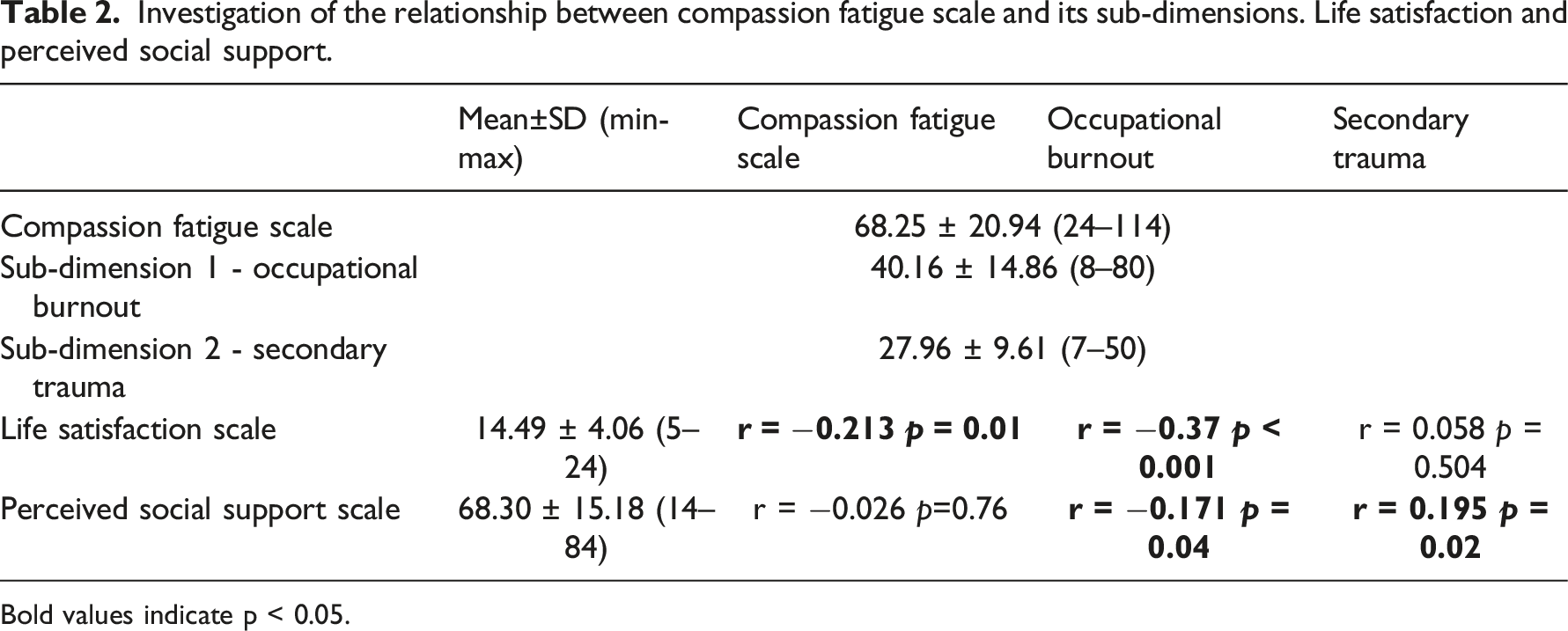
Bold values indicate p < 0.05.
Investigation of the factors predicting compassion fatigue scale, occupational burnout and secondary trauma.
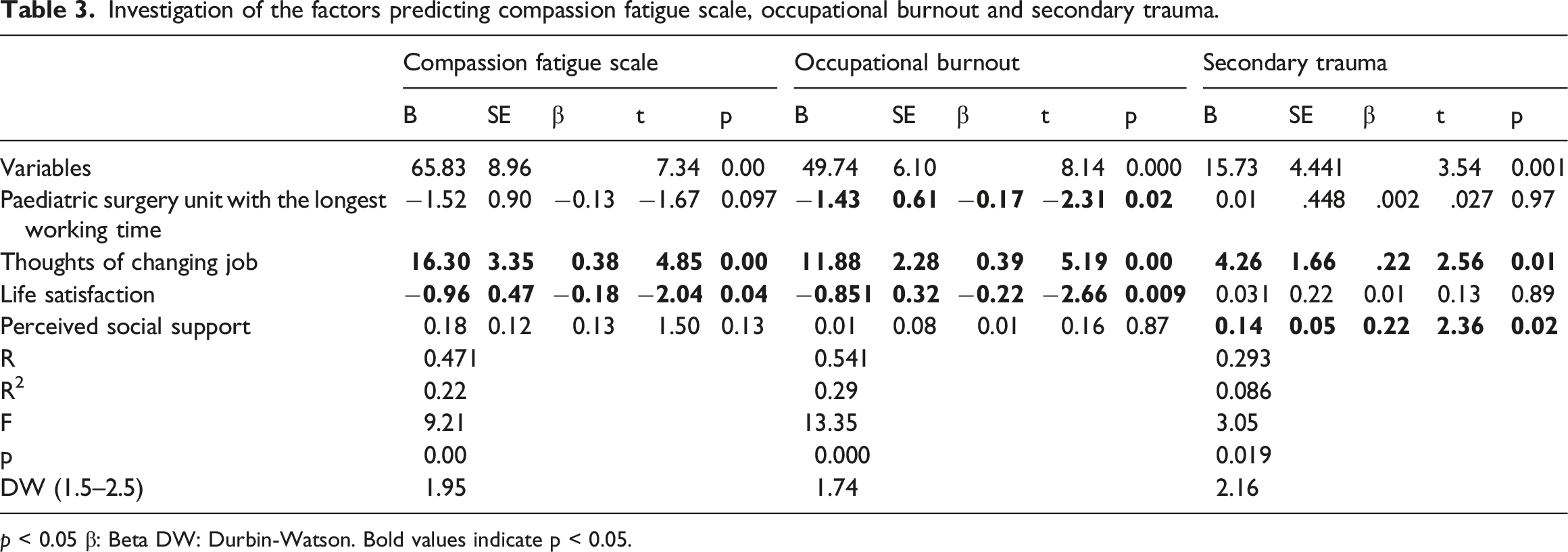
p < 0.05 β: Beta DW: Durbin-Watson. Bold values indicate p < 0.05.
Discussion
This study aimed to investigate CF and its predictive factors among paediatric surgical nurses in Türkiye. The study found no significant differences in CF levels based on gender, age, years of experience, marital status, level of education, having children, shift type, willingness to choose the profession, thoughts of changing profession or satisfaction with their team. In a cross-sectional study of paediatric registered nurses (RNs), contrary to our findings, nurses under 40 years of age, with 6–10 years of experience and/or working in medical-surgical units exhibited significantly lower CS and higher levels of burnout. 17 Another study of nurses (n = 336) in eastern Türkiye revealed that CF levels were significantly higher among women, singles and those working both day and night shifts. 14 In a different study of nurses (n = 207) in surgical units, there were no significant differences in CF levels based on age, gender or level of education. 29 In a cross-sectional study (n = 284) with paediatric nurses in the Turkish Republic of Northern Cyprus, almost all nurses had low to moderate levels of CF, and it was noted that CF levels were influenced by factors such as age, seniority, length of service, marital status and having children. 30 Based on the findings of our study, it is suggested that paediatric surgical nurses demonstrate an unwavering commitment to the cognitive, physical, social, and emotional well-being and development of every child undergoing surgical intervention, showing dedication to their profession regardless of age or years of experience.
In our study, nurses considering a career change and those working in the burn unit had higher scores for CF. Notably, we could not find any studies investigating CF in nurses considering a career change, suggesting that individuals who choose their profession reluctantly for various reasons may be more susceptible to CF. Another significant factor influencing CF is the specific unit in which the nurses work, with nurses in the burn unit demonstrating the highest levels of CF. This finding aligns with the study by Aslan et al., which also reported unit-related differences in CF levels, with the highest CF levels observed among ICU nurses. 15 Moreover, a comprehensive meta-analysis of 79 studies involving 28,509 nurses from 11 countries worldwide found that ICU nurses consistently had the highest levels of CF symptoms compared to nurses in other specialities. 31 However, in contrast to our findings, a study of paediatric nurses found no significant differences in CF scores between different units. 30 It is essential to note that the burn unit is a specialised unit within paediatric surgery, where nurses play a central role in the burn care team. Burn unit nurses are required to have extensive knowledge in areas such as multiple organ failure, diagnostic procedures, critical care techniques, rehabilitation and psychosocial skills. Furthermore, nurses in the burn unit not only focus on the survival of burn-injured children but also help them overcome burn trauma and develop coping skills. 32 Therefore, it is suggested that factors such as empathy and exposure, which according to Figley’s theory contribute to CF, may be more prevalent among paediatric surgical nurses working in the burn unit. In terms of exposure, nurses in the burn unit are constantly exposed to the emotional states of burn-injured children and their parents during their shifts. Consequently, within the socio-psychological context of empathy, characterised by its ‘other-oriented’ nature, the ability to understand and share the emotional experiences of burn-injured children and parents is believed to contribute to higher levels of CF.
When examining the occupational burnout sub-dimension of CF, it was found that nurses working in the burn unit, those who did not choose their profession voluntarily and those contemplating a career change had elevated occupational burnout scores. Consistent with our study, Denk and Koçkar (2018), in their research on CF levels among surgical nurses, reported higher levels of occupational burnout among individuals who did not willingly choose the nursing profession. 29 In a study of paediatric nurses in California (n = 240), differences in burnout scores were observed across different clinical units, including surgical clinics, internal medicine clinics, ICU and haematology/oncology units. Notably, the highest level of burnout was reported in the surgical clinic. 33 Working in the burn unit is characterised by long-term energy depletion, encompassing emotional exhaustion, reduced personal accomplishment, feelings of inadequacy and depersonalisation among nurses. Because nursing involves interdependence and is an act performed for the benefit of others, nurses in the burn unit who did not willingly choose their profession and are considering a career change may have elevated CF scores. This may be attributed to the demanding nature of nursing, which extends beyond self-interest and involves a high level of emotional investment.
When variables related to the secondary trauma sub-dimension of the CF scale were examined, it was found that only nurses contemplating a career change had significantly higher average scores. In contrast to our findings, a study of ICU nurses found differences in burnout and secondary traumatic stress scores based on age group, with nurses aged 40–49 years having significantly higher levels of burnout and secondary traumatic stress than other age groups. 34 CF is the natural consequence of witnessing individuals who are sick or suffering. It results from the stress of attempting to assist someone in distress, being engaged in or witnessing the challenging experiences of individuals undergoing various forms of suffering, and is a combination of burnout and post-traumatic stress disorder. In paediatric surgical nursing, the responsibilities extend beyond promoting the healthy growth and development of children to include pre- and post-surgical care needs. Paediatric surgical nursing is further categorised into neonatal and paediatric surgery, with surgical procedures falling into the categories of urology, abdominal and thoracic surgeries. 35 Given the diversity of units and patient populations, paediatric surgical nurses must be knowledgeable about the unique care requirements of each. The fact that the patients in these units are children places an additional responsibility on the nurse to maintain a warm, compassionate and family-oriented approach to care.
In this study, the nurses’ mean score on the CF scale was 68.25 ± 20.94, and they were found to have moderate CF. In a cross-sectional study conducted in Northern Uganda, 49.11% (n = 194) of the nurses reported that they had high CF, 29.62% (n = 117) had moderate compassion and 21.27% (n = 84) had low levels of CF. 36 In the meta-analysis study by Xie et al., it was emphasised that the Asian region had the highest level of CF symptoms, while America and Europe had the lowest level of CF, and the level of CF in nurses gradually increased from 2010 to 2019, reaching the highest level in 2019. 31 Our research findings are similar to the literature.
In our study, a weak but statistically significant negative correlation was observed between the level of CF in paediatric surgical nurses and their life satisfaction. However, no significant relationship was found between CF and perceived social support. Additionally, a weak negative correlation was found between occupational burnout and life satisfaction. There was also a weak correlation between perceived social support and the sub-dimensions of occupational burnout and secondary trauma. In a study of nurses in Poland (n = 862), higher levels of perceived social support were associated with lower levels of CF, and higher levels of social support were linked to a lower risk of burnout. 37 Similarly, a relational descriptive study in Iran (n = 173) found that increased social support among nurses led to decreased burnout, with family support being a significant predictor of both CF and burnout. 38 The study suggests that as CF levels increase among paediatric surgical nurses, their life satisfaction tends to decrease. Caring for paediatric patients and addressing their needs, along with those of their families, can increase the likelihood of paediatric surgical nurses encountering ethical dilemmas. Balancing professional responsibilities with ethical decisions in these complex situations is crucial, even though ethical decisions may sometimes conflict with moral values. This can be particularly challenging when meeting the needs of paediatric patients and their families, potentially leading to ethical fatigue among paediatric surgical nurses. Moreover, the support nurses receive from their social environment plays a vital role. Such support can help reduce the risk of professional burnout and secondary trauma. However, the absence or reduction of this support may increase the risk of occupational burnout and secondary trauma.
When examining predictors of CF, occupational burnout and secondary trauma among paediatric surgical nurses, several significant factors were identified. The longest tenure in the paediatric surgical unit, thoughts of leaving the nursing profession and life satisfaction were found to be significant predictors of CF (F = 9.21; p < 0.001). Specifically, thinking of leaving the nursing profession and life satisfaction together accounted for 22% of the variance in CF. The same variables were also predictors of occupational burnout, explaining 29% of the variance in burnout. Additionally, contemplating a career change and perceived social support were predictors of secondary trauma, explaining approximately 10% of the variance in secondary trauma (F = 3.05, p = 0.019). Previous studies have found that attitude to life, years of experience in the profession and gender affect CF. 14 In a study of Chinese registered nurses, both work stress and perceived social support were found to moderately and directly affect burnout. 12 Furthermore, CF has been identified in previous research as one of the most important determinants of life satisfaction. 7 Working extensively in a paediatric surgical unit may expose nurses to the continuous traumatic experiences of paediatric patients and their families. This continuous exposure can lead to nurses experiencing CF and professional burnout, as highlighted in Figley’s theory of compassion fatigue. Moreover, the contemplation of changing professions may stem from these traumatic experiences and workload. According to Figley’s theory, individuals experiencing CF may wish to avoid or minimise repeated exposure to traumatic experiences, leading to thoughts of changing their profession. Life satisfaction and perceived social support play pivotal roles in helping nurses cope with these experiences. Higher levels of life satisfaction may enable nurses to cope better with traumatic encounters, while higher levels of perceived social support can create a more supportive environment.4-7 In conclusion, these findings shed light on the impact of traumatic experiences on paediatric surgical nurses, in alignment with Figley’s theory of compassion fatigue. Nurses must consider the possibility of a career change to ensure their emotional and psychological well-being. Strengthening social support networks can also enhance life satisfaction. These insights may contribute to a better understanding of how paediatric surgical nurses provide healthcare services and approach ethical dilemmas.
Limitations
The biggest limitation of this study was the inability to reach all paediatric surgical nurses in Türkiye. Some nurses who are members of the association could not be contacted for the study due to the change of surnames due to marriage, change of hospital where they work and change of email addresses.
Since the number of nurses was limited in this study, all paediatric surgical nurses were included in the study and new nurses were not excluded. However, in the analyses, the years of experience did not make a significant difference.
Conclusion
The study revealed that CF, life satisfaction and perceived social support are moderate among paediatric surgical nurses. CF appears to be influenced by factors such as working hours, contemplation of career change, life satisfaction and perceived social support. Interestingly, no significant differences were observed in CF levels based on gender, age, years of experience, marital status, education level, parenthood status, shift type, voluntary choice of nursing profession, contemplation of changing professions or satisfaction with their team. Caring for child patients and addressing the multifaceted needs of both child patients and their families can potentially contribute to professional burnout among paediatric surgical nurses. These healthcare professionals are tasked with providing comprehensive care, which can be emotionally demanding. Moreover, a decline in social support may further exacerbate their professional burnout and expose them to secondary trauma. Notably, nurses working in the burn unit exhibited the highest levels of CF. Nurses in the burn unit require extensive knowledge of multiple organ failure, diagnostic procedures, critical patient care techniques, as well as rehabilitative and psychosocial skills. They play a crucial role in helping children with burns to not only survive but also overcome the trauma associated with burns and develop coping mechanisms. Consequently, paediatric surgical nurses working in the burn unit may be particularly affected by this complex and demanding process, leading to higher levels of CF. In light of these findings, clinical improvements are strongly recommended to increase nurses’ commitment to the profession and reduce CF, especially among those in specialised units such as paediatric surgery. Ethical considerations regarding the emotional and psychological well-being of healthcare professionals in such roles should be a central focus of these efforts.
Footnotes
Acknowledgements
The authors would like to thank Ayşe İSLAMOĞLU and Birsen EROĞLU for their support during the research process and all the nurses who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.