
Abstract
Patients with advanced cancer often experience a reduced ability to eat, which may result in tensions between patients and family members. Often with advanced cancer diagnoses, patients’ appetites decline markedly, while family members focus on nutritional intake with the hope that this will postpone death. This hope might cause tensions between the patient and family; the family may expect healthcare professionals to encourage the patient to eat more, whereas the patient needs to be supported in their reduced ability to eat. When these tensions arise, healthcare professionals can experience challenges in providing good palliative care. To address these challenges in the provision of palliative care, healthcare professionals may adopt a care ethics approach. Similar to palliative care’s focus on patient and family members’ relationships, a care ethics approach emphasizes interdependency and social relationships. Using Joan Tronto’s care ethics approach, we conducted a normative analysis of what caring for patients with reduced ability to eat and their family members should look like. Tronto’s approach includes five phases of care: caring about, taking care of, care giving, care-receiving, and caring with. Based on our analysis and empirical studies on patients with advanced cancer and family members, concerns with their lack of appetite, we assert that healthcare professionals must be mindful of the potential of tensions related to appetite and be adept in dealing with these tensions. We urge that education is needed for healthcare professionals regarding the psychosocial impact of reduced ability to eat on both patients and family members and interprofessional collaboration is of the essence.
Keywords
Introduction
A common symptom in patients with advanced cancer is a reduced ability to eat. 1 Patients may experience a loss of appetite, changes in taste, smell, satiety, chewing and swallowing problems, and nausea. Diminished nutritional intake together with abnormal metabolism can result in cachexia, which is characterized by unintended and unwanted weight loss.2,3 In this article, we refer to patients with advanced cancer and a reduced ability to eat when talking about patients with end-stage/terminal cancer and/or cancer cachexia.
Reduced ability to eat can have psychosocial consequences. While patients are less able or unable to eat, family members may insist on increasing nutritional intake with the hope that this will postpone death. Furthermore, preparing and offering food and eating together are meaningful social and cultural activities. For instance, we celebrate special moments and traditional holidays together with special foods.2,4,5 Offering food is often considered an important way to care for a loved one. If this is no longer possible due to a reduced ability to eat, this could provoke negative feelings such as depression and anxiety in both the patient and their family members.2,6,7
An important source for scholars writing on the subject is Deborah Lupton with her work Food, the Body and the Self. 8 She describes how, for a healthy person, food preferences change slowly over time, while for a dying person these changes can emerge fast, resulting in loss of familiarity and shared understanding between patients and family members. Mealtimes become moments of frustration and hopelessness. 8 Also Barbara Karnes stresses that it is normal for people to stop eating in the dying process. In a recent blog building on her work Gone from My Sight: The Dying Experience, she writes ‘When the dying process begins it is normal for eating to gradually stop. […] The goal becomes one of providing comfort. Always offering food but not forcing is the comfort we give now. Don’t force or be disappointed when the food is not eaten’.9,10 However, family members often do not understand that patients are not dying because they are not eating, but that they are not eating because they are dying. The weight loss accompanied with reduced ability to eat is tangible and is considered visible evidence of disease progression that symbolizes the approaching death of their loved one. 4 For patients, eating often becomes a burden and a chore, while family members may try to increase nutritional intake by pressuring patients to eat. 11 Hence, the reduced ability to eat may evolve into a source of tension between patients and family members: whereas family members want patients to eat more, patients feel very uncomfortable or even unable to do so. 12
First and foremost, palliative care is aimed at preserving quality of life rather than survival, and at managing symptoms. For patients with advanced cancer, it is therefore important to adapt dietary advice to existing symptoms; meeting nutritional requirements no longer has priority. Patients experience that eating is no longer pleasurable and might need psychosocial support to deal with this.
Further according to the World Health Organization (WHO), palliative care entails care for both patients and family members. 13 Family members have care needs (i.e. different needs for care that someone has) of their own, such as practical support in their care activities and psychosocial support in the process of dealing with a dying loved one. Furthermore, family members are often involved in care for the patient. They provide direct care to the patient, organize and coordinate formal care services, and assist the patient in daily life activities.14,15 In the case of reduced ability to eat, family members may want healthcare professionals to support them in their need to ensure that the patient eats enough and engages in activities around eating with the patient.
These conflicting needs of patients and family members and the resulting tense situations could pose a challenge for healthcare professionals. How can they support the patient in not eating without ignoring the needs of family members? How can they support the family members in caring for the patient without going along with their focus on nutritional intake? Should they play a role in mediating between them in the case of tensions? What is the best way to address the subject? Research shows that many healthcare professionals experience uncertainty in how to address the psychosocial consequences of and the fear of talking about reduced ability to eat, especially when this leads to tensions within the family.16,17,18,19 How can healthcare professionals provide good care to both patient and family members in a situation in which their care needs (i.e. different needs for care that someone has) seem at odds with each other?
In this article, we explore how healthcare professionals could deal with this issue, while providing good palliative care to both patients with advanced cancer and reduced ability to eat and their family members. First, the dynamics and tensions between patients with cancer with reduced ability to eat and their family members will be examined. Subsequently, experiences and perspectives of healthcare professionals on this issue will be described. Third, we consider what good palliative care would entail from a care ethics approach. We will argue that, considering the deeply relational nature of this issue, as well as the complexity of care needs and responsibilities of those involved, a care ethics approach is most helpful to establish a normative orientation on this issue. Specifically, Joan Tronto’s account of the five phases of caring will be applied to a case example. Finally, we maintain that healthcare professionals could benefit from education on the psychosocial consequences of reduced ability to eat as well as from interprofessional collaboration in order to improve both their competence and attentiveness to this issue.
Caring for persons with reduced ability to eat and their family members
Good palliative care requires attention to physical, psychological, social, and spiritual problems and needs of both patients and their family members. 1 Patients with advanced cancer and their family members can experience problems in all these dimensions. Hence, their care needs for patients’ reduced ability to eat are multidimensional. First of all, patients may experience a variety of physical complaints related to not eating. Due to the tumour or treatment, patients may lose appetite, encounter changes in taste, smell, and early satiety, have chewing and swallowing problems, and experience nausea.3,6 The diminished nutritional intake that follows, together with metabolic disturbances, might eventually result in (refractory) cachexia. 2
Furthermore, patients and their family members both experience psychosocial problems. They often experience negative emotions surrounding eating, such as anger, anxiety disappointment, guilt, grief, powerlessness, shame, and frustration.2,7 For patients, these emotions may emerge directly from changes in the experience of eating or rather indirectly due to loss of control over the body or struggle with eating.1,2,7 For family members, these emotions result from concerns about the patient’s well-being, the patient’s rejection of prepared meals and physical decline, thoughts about the future, and mourning about the loss of shared meals and ‘togetherness’.2,7 In addition, Cooper et al. (2015) described that patients perceive loss of socializing, stigma, and embarrassment because of reduced ability to eat. 6 Family members feel a high sense of responsibility towards the patients’ well-being 7 and experience loss of familiarity and understanding, possibly resulting in disappointment and a sense of helplessness. 4
Lastly, patients and family members may experience existential problems, as they are confronted with death. Weight loss symbolizes disease progression and the approaching death, possibly leading to existential distress. 6 For some patients and family members, eating becomes all that is necessary to stay alive ‘If you don’t eat, you will die’. 20 Also more generally, the awareness of being at the end of life may give rise to existential and spiritual concerns, such as about the meaning of life and the possibility of life after death. 21
Due to these problems, tensions between patients and family members may arise. Research has shown that these tensions can be described under two main denominators, that is, tensions that relate to ‘taking charge’ and ‘protecting each other’. The tensions related to ‘taking charge’ arise from family members wanting to take charge over the patient’s nutritional intake, which is often related to denial of the terminal nature of cancer and non-acceptance of impending death. 22 ‘Taking charge’ can include surveillance of the patients’ nutritional intake and frequently offering (favourite) food. As a result, the patient can feel pressured to eat, resulting in both emotional distress and physical suffering.7,23,24 They may cope by avoiding social events or by isolating themselves. 17 Previous research suggests that family members adopt the dynamic of ‘taking charge’ because of their high sense of responsibility for the patient’s well-being. 7 Cooper et al. (2015) described a common fear among family members that if they are not always present to prepare food and encourage the patient to eat, the patient will die. Family members thus assume responsibility for the declining health status of the patient while this is due to disease progression. 6
The tensions related to ‘protecting each other’ concern patients and family members protecting each other from negative feelings, for instance, by means of avoiding food-related topics.5,25 Also, patients may want to unburden their family members by eating to please them and to ease their concerns, although they feel very uncomfortable by doing so.12,25
Research shows that some healthcare professionals experience difficulties in caring for patients with advanced cancer and their family members. Especially, it is found that dealing with the psychosocial consequences of reduced ability to eat can be difficult. Lize et al. (under review) found that some healthcare professionals did not recognize and assess psychosocial needs regarding the patient’s reduced ability to eat. 26 Moreover, several studies found that healthcare professionals often fear talking about reduced ability to eat because they felt it might take hope away or cause unnecessary distress.8,11,12,19 They often wait until patients or family members raise problems regarding eating themselves, rather than initiating such conversations, or merely address problems in an implicit way.16,19
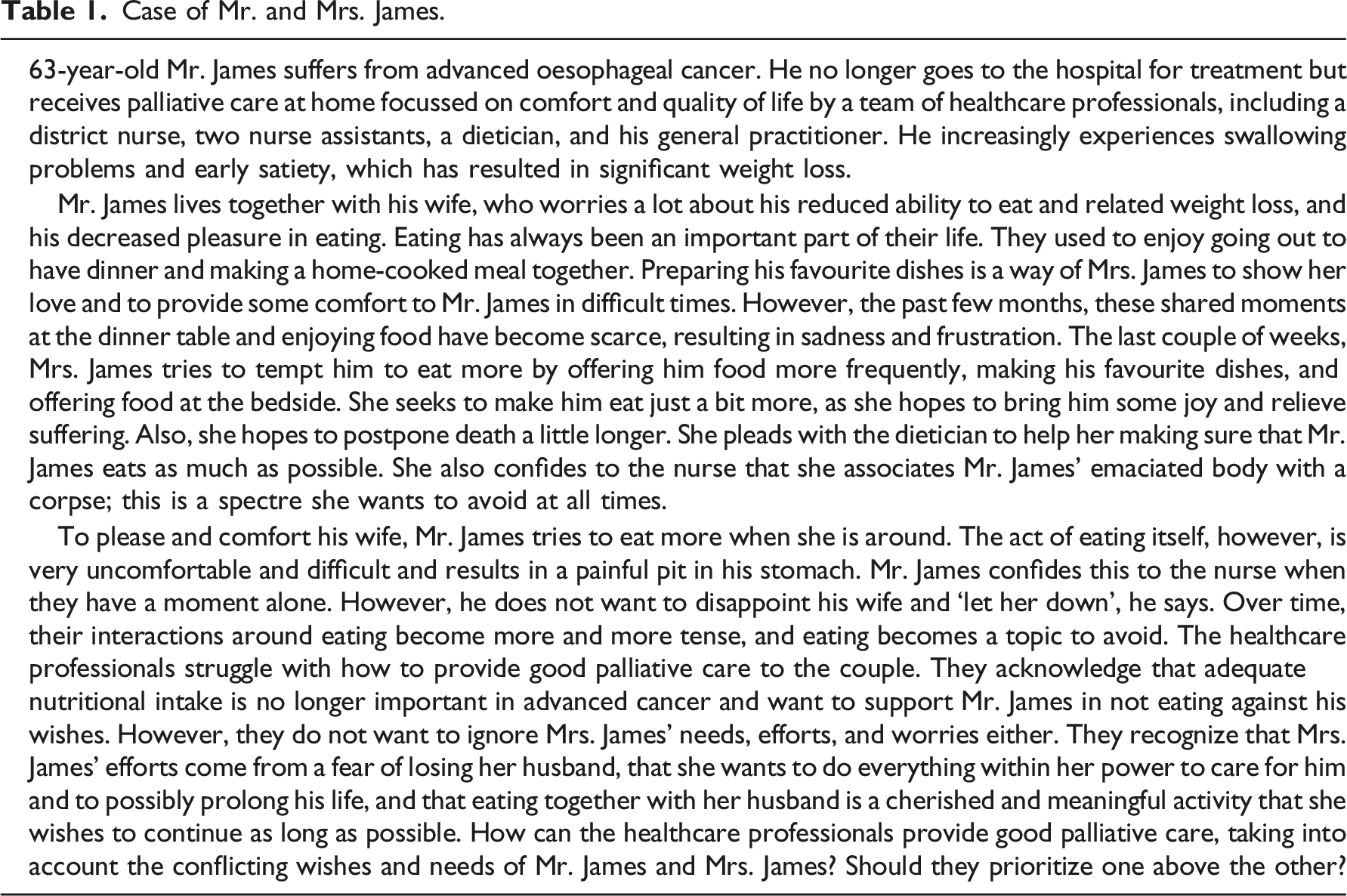
Case of Mr. and Mrs. James.
A care ethics analysis
Care ethics proceeds from an understanding of human life as characterized by interdependency and networks of social relations. Therefore, it assigns great moral significance to concrete relationships, dependencies, and responsibilities. It considers care needs primarily in the context of the concrete identity, biography, and relationships of those involved, rather than relating them to more abstract, a priori principles. 27 Correspondingly, care ethics regards autonomy as relational rather than as individual; someone is autonomous to the extent that (s)he is able to take control of his/her life and realize his/her life goals, while being bound to his/her bodily, mental, spiritual, and social condition, and while being interdependent with others in processes of self-realization. 28 Therefore, in shaping ‘the good life’, also at the end of life, people need each other.
Relational autonomy has been advanced as a foundational notion of palliative care because the individual notion of autonomy fails to encompass interpersonal dimensions central to palliative care, such as possibilities of informal care. 29 This is in line with the recognition that palliative care should deal with the psychosocial aspects of patients and family members; 1 both patients and family members, and the relationships between them, should be considered in the care process. The concept of relational autonomy especially applies to the issue of reduced ability to eat in advanced cancer and the tensions that can arise from this.
Tronto’s Five Phases of Caring.
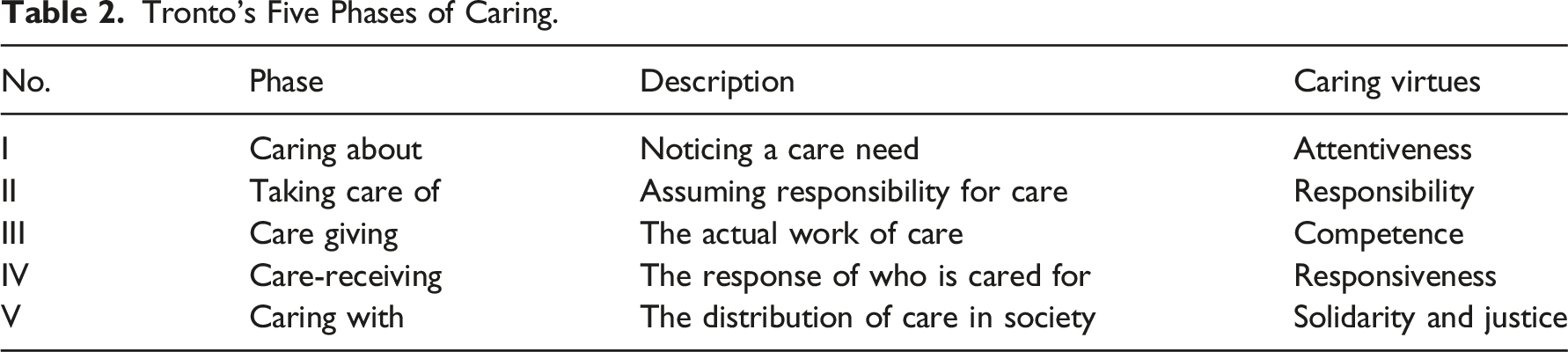
In the following sections, we will explore the issue of Mr. James’ reduced ability to eat using Tronto’s five phases of caring, specifically focussing on obstacles and disruptions in the care process that are known to arise.
Caring about
The first phase of caring, caring about, is about noticing or recognizing care needs. As palliative care is multidimensional by nature and not restricted to physical aspects,1,13 this entails also being attentive to psychological, social, and existential needs and wishes. In addition, it entails not only recognizing the patient’s needs but also those of family members. 1 As mentioned before, some healthcare professionals experience difficulties in recognizing the psychosocial consequences and impact of reduced ability to eat in both patients and family members. Especially since patients and family members often address psychosocial problems indirectly, or express them by means of non-verbal signals. 26
In the case of Mr. and Mrs. James, the professionals involved do recognize the tension between the couple, as well as their unmet psychosocial care needs. However, they struggle with the right way of dealing with them.
Taking care of
The second phase of caring, taking care of, entails that healthcare professionals take upon themselves the responsibility to care and initiate giving care. First, this responsibility touches upon the question to whom healthcare professionals have a caring responsibility. According to the definition of palliative care by the WHO, both patient and family members are central to palliative care. 13 Many healthcare professionals providing palliative care acknowledge that they indeed have a dyadic responsibility to care for both patients and family members and value the involvement of family members in caring for reduced ability to eat. 26
Second, the responsibility to care touches upon the question which healthcare professionals are considered responsible to provide palliative care. Internationally, several models of palliative care delivery are adopted, in which the main distinction can be made between specialist models of palliative care and ‘mixed models’, that is, models that combine generalist with specialist palliative care. For example, in the United Kingdom and United States, a specialist model is adopted in which (hospice and) palliative medicine is a distinct medical specialty.32,33 In contrast, in the Netherlands, palliative care is supposed to be provided by all healthcare professionals. If necessary, they are supported by specialists in palliative care, or to whom the patient is referred when the complexity of the case goes beyond what generalist palliative care can cover (i.e. mixed model). 1
Depending on the model of palliative care delivery, healthcare professionals might have the responsibility to provide generalist palliative care (mixed model) and/or the responsibility to consult or refer to specialist palliative care services (mixed and specialist model). Some healthcare professionals do not see psychosocial support as part of their role. They may recognize these psychosocial needs but do not feel responsible or competent to address them. A UK study by Millar et al. (2013) found that nurses without specialist palliative care expertise often recognized weight loss but not discussed it with patients and their family members because they did not feel equipped to do so. 18 This is not necessarily problematic if these nurses consult or refer to other healthcare professionals in a timely matter. After all, palliative care is an interprofessional endeavour. 13 However, a Dutch study by Lize et al. (under review) suggests that multidisciplinary collaboration is an important facilitator for healthcare professionals to start psychosocial support for a reduced ability to eat. The absence of this collaboration can result in inaction of healthcare professionals and in unmet psychosocial care needs of both the family and the patient. 26 Hence, some healthcare professionals do not take upon themselves the responsibility for providing care, either themselves or through referral. This inaction may result in unmet psychosocial care needs of both the family and patients.
In the case of Mr. and Mrs. James, the responsibility to take action is felt by the team, although they are unsure how to initiate it.
Care giving
The third phase of caring, care giving, is providing the actual care and requires that healthcare professionals possess the competence to do so. As discussed, studies have shown that many healthcare professionals experience to be insufficiently competent due to a lack of knowledge about the multidimensional impact of reduced ability to eat, especially the psychosocial impact.6,17–19,26,34,35 Healthcare professionals express uncertainty about how to help patients and fear talking about reduced ability to eat16–19 because it may take away hope or cause unnecessary distress in patients and family members.16,36 Moreover, healthcare professionals are often found to wait for patients or family members to raise problems regarding eating themselves. However, patients and family members often do not raise problems or merely address them in an implicit way.16-19 In order to give good care to patients with reduced ability to eat and their family members, healthcare professionals should therefore possess the competence to initiate conversations about and address (psychosocial, physical, and existential) problems related to this reduced ability to eat.
Furthermore, in an interview study by Lize et al. (under review), many healthcare professionals explicitly mentioned that they preferred to discuss concerns with the patient and family members together, in a joint conversation. 26 Yet, previous research has identified the dynamics of ‘protecting each other’ between patient and family, through which they might avoid discussing food-related topics in order to prevent hurting each other.4,25 Family members sometimes take the initiative to discuss their concerns openly when the patient is not present. For instance, at the front door, when the healthcare professional is leaving. Patients may take this opportunity as well. For instance, when family members are making coffee in the kitchen. Hence, it is argued that talking to the patient and their family members alone might also be beneficial and sometimes even necessary in order to deal with these problems. 26
In the second phase of caring, taking care of, we discussed that healthcare professionals should take responsibility to refer to other healthcare professionals if necessary. In this third phase of caring, care giving, the focus is on the competence to know when it is necessary and appropriate to consult or refer to other healthcare professionals with the right specialized expertise. Research suggests that this is not always the case. Some healthcare professionals were found to be in doubt whether to refer to other healthcare professionals because they doubted whether their colleagues were sufficiently equipped to provide psychosocial support. 26 In addition, it was reported that healthcare professionals sometimes referred or consulted colleagues too late, especially to dieticians. 26 Late referral to dieticians, with the sole intention to improve nutritional intake, might be inappropriate, even if family members insist on this. Alternatively, previous research assigns dieticians an important role in psychosocial support, in both understanding and accepting the reduced ability to eat. Pinto et al. (2016) suggest that dietetic consultations provide an opportunity for patients to raise problems they were unable to raise with other healthcare professionals. 37
In the case of Mr. and Mrs. James, both confided in their healthcare professionals when alone with them, but protected each other by avoiding food-related topics in each other’s presence. This underscores the importance of creating the opportunity to have conversations separately. Mr. James spoke about his efforts to eat more in order to meet the wishes of his wife, which results in a pit in his stomach, whereas Mrs. James confided about the spectre of her husband’s corpse, which she wants to avoid at all times. These moments alone provide patients with the opportunity to speak openly about their concerns and healthcare professionals with the opportunity to listen, explain, and normalize their worries and struggles regarding reduced ability to eat. In addition to talking with patients or family members separately, the healthcare professionals involved could initiate and facilitate a joint conversation. When the healthcare professionals do not feel equipped, they should consult or refer to colleagues, for instance, a nurse or dietician with specialized expertise in palliative care or, if appropriate, a spiritual care counsellor.
Care receiving
The fourth phase of caring, care receiving, maintains that healthcare professionals should check whether the provided care was indeed coherent with the care needs of the care receiver(s), in this case the patient and family members. Whereas caregivers should be receptive with regard to the care receiver’s response, care receivers should be receptive to the care itself; without this mutual receptivity, good care cannot be established.
Socio-cultural factors play an important role when it comes to (talking about) food in the dying phase, for example, the symbolism and meaning of food differs between cultures but also the topic of death and dying itself concerns different levels of preferred openness.2,4,5,25 A Dutch qualitative study of patients and family members with Turkish and Moroccan origin and their healthcare professionals found that many families preferred not to inform the patient directly about impending death, in order to maintain hope alive and/or to preserve dignity. 38 It is important to be aware and to take this into account when addressing the subject of reduced ability to eat. Lize et al. (under review) found that some healthcare professionals, who deliberately avoided talking about eating, did so because they were afraid of being culturally inappropriate. 26
In the case of Mr. and Mrs. James, healthcare professionals should check whether the psychosocial support that was provided has actually resulted in less tensions between Mr. and Mrs. James. For instance, is Mrs. James able to let Mr. James take control of his food intake instead of offering him food all the time? Does Mr. James eat when he wants to instead of forcing himself to eat? Can Mrs. James come to accept that Mr. James will die soon?
Caring with
The fifth phase of caring, caring with, relates to the question how we ensure that everyone in society who needs care receives care, and how we distribute care as a scarce good across a population with different care needs. Tronto argues that social justice, solidarity, and fairness in the distribution of resources are essential at this phase of caring. 31
Millar et al. (2013) argue that dedicated time with patients and their family members allows for a more effective management of the reduced ability to eat, as it promotes more effective communication. 18 However, previous research shows that a lack of staff 6 and time, especially of physicians, 18 leaves healthcare professionals being limited in finding this dedicated time. Therefore, the responsibility for care may be shifting, at least in part, from formal care to informal care. Informal care is often provided by family, friends, or volunteers. 39
Informal care is an important and valuable complement to formal care. Research shows that informal care is of particular value to patients with cancer and their family in coping with the psychosocial consequences. 39 Yet, an increased reliance on informal caregivers, such as relatives, risks exacerbating social injustices; receiving appropriate and sufficient care will become more dependent on one’s personal social network and their efforts. As a result, those without an active social network may receive much less care than those who do have such a network.
Additionally, some people’s privileged social or financial position gives them access to care that others may not have, for example, to privatized care resources. This access can reduce the burden on informal caregivers and compensate for the lack of time and staff in the public healthcare system. However, people without these resources will not have this access to care.
Here, ‘caring with’ could entail making psychosocial support for tensions related to a reduced ability to eat part of publicly funded healthcare and/or of care for which people are normally insured for. It could also involve a careful assessment of the extent to which patients can rely on informal caregivers and presenting alternatives where this is not the case.
In the case of Mr. and Mrs. James, good care first of all depends on the possibility of the healthcare professionals that are already involved to take the time to have conversations with both of them about (not) eating. Are they able to do so? It is not yet clear whether the couple needs specialized psychosocial support, whether they will have to pay for this themselves, and whether they can afford this. Also, it is not clear whether they have children who can help them with resolving the tensions around eating. Yet, these are important things to assess for the team.
Discussion
Our care ethics analysis highlights several important aspects of caring for patients with advanced cancer experiencing reduced ability to eat and their family members. As we have seen, palliative care for these patients and their family members is holistic care for multidimensional care needs. Healthcare professionals need to be sufficiently competent in recognizing these needs, knowing when to take responsibility to act upon these needs, and in dealing well with these needs. However, healthcare professionals report a lack in these skills, and there is a need for more education and training, especially with regard to the psychosocial impact of the reduced ability to eat on both patients and family members.6,7–19,26,34,35 In the Netherlands, where this study was conducted, it is now agreed upon that every healthcare professional should be able to provide good quality palliative care on a ‘generalist’ level. 1 Accordingly, training should be provided at a basic level of education. This training should include addressing needs related to a reduced ability to eat.
Furthermore, in the case of tensions between patients and family members due to a reduced ability to eat, healthcare professionals have a dyadic responsibility to meet both the needs of the family members and of the patient. Many healthcare professionals are found to acknowledge and value this dyadic responsibility. However, navigating this responsibility when care needs compete has shown to be complex. Education and training could provide healthcare professionals with the tools and confidence to initiate conversations with patients and family members in order to provide adequate (psychosocial) support, especially in the case of tensions.
Palliative care is an interprofessional endeavour. 13 Healthcare professionals are interdependent, especially when it comes to dealing with complex care needs. If healthcare professionals do not feel fully equipped to meet specific care needs, such as psychosocial support, they should consult or refer to healthcare professionals that have the specialized expertise to do so. In such cases, healthcare professionals need to know which healthcare professional to consult or refer to and when and how to contact them. Therefore, healthcare systems need to invest in interprofessional collaboration. Existing structures for interprofessional collaboration in oncology and/or palliative care include consultation of a palliative care consultant within the organization, or, in home care settings, establish multidisciplinary group meetings to discuss patients with complex care needs. 40 By making time available for interprofessional consultation and investing in networks that encourage interprofessional collaboration, healthcare professionals may be better equipped to consult and refer to colleagues with the appropriate expertise.
Different people attribute varying levels of importance to food. We have argued here that healthcare professionals need to be sufficiently competent to manage the tensions and care needs related to a reduced ability to eat in patients with advanced cancer. This includes being able to deal with the fact that patients and family members may have different perspectives than healthcare professionals on good care, for example, because of cultural differences. Socio-cultural factors play an important role when it comes to (talking about) food in the dying phase.2,4,5,25 Food may be an important aspect of a cultural identity, valuing traditional recipes and culinary customs, which makes for added significance of eating for individuals. Also, in some cultures it may be considered inappropriate to talk to patients about their impending death and the resulting changed role of food in the dying process. Sensitivity to (cultural) diversity should be part of healthcare professionals’ caring virtues when caring for patients with a reduced ability to eat and their families in all phases of caring. This sensitivity is not limited to culture but should include all individual differences.
Conclusion
Our care ethics analysis elucidates several important aspects of caring for both patients with advanced cancer with a reduced ability to eat and their family members. We maintain that especially attentiveness and competence are caring virtues that should be fostered among healthcare professionals. Attentiveness particularly applies here to recognizing the psychosocial impact of reduced ability to eat and the tense situations that may arise from this between the patient and family members, whereas competence applies to knowing how to deal well with these tensions, while attending to the care needs of both the patients and the family. Empirical research shows that healthcare professionals experience difficulties in doing so. Therefore, we argue that adequate education and training in (dealing with) the psychosocial impact of reduced ability to eat on both patients and family members and interprofessional collaboration is of the essence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.