
Abstract
Background
Individuals living with multimorbidity and/or mental health issues, low education, socioeconomic status, and polypharmacy are often called complex patients. The complexity of their health and social care needs can make them prone to disease burden and suffering. Therefore, they frequently access health care services to seek guidance for managing their illness and suffering.
Aims
The aim of this research was to describe the approaches used by nurses to alleviate the suffering of individuals with multimorbidity and complex needs in acute care settings.
Research Design
A qualitative descriptive approach.
Participants and Research Context
Semi-structured interviews were conducted with 19 nurses working in general, medical-surgical, specialized, and intensive care settings across five hospitals in Pakistan. Reflexive thematic analysis was used for analysis.
Ethical Considerations
Ethical approval was obtained from the Ethical Committee of Al-Nafees Medical College Islamabad, Pakistan.
Findings
Four themes were generated: Deeper Exploration of Patients’ Health-Illness Situation and Complexity, Prioritizing Patient Psychosocial and Emotional Needs, Instilling Hope and Encouragement in Patients, and Creating a Comforting Environment to Foster Sharing of felt needs.
Discussion
Nurses emphasized the need of deeper inquiry into patients illness situation and complexity to discern the impact of determinants on their well-being and develop care plans that are tailored to address psychosocial, emotional, and physical suffering of this patient population.
Conclusions
Alleviation of patient suffering is integral to compassionate nursing care. Nurses use a multifaceted approach entailing sensitive understanding, recognizing sociocultural and structural determinants impact on patient situation, and individual and interdisciplinary altruistic actions to alleviate patient suffering.
Introduction
Complex patients have multimorbidity (coexistence of two or more chronic conditions), polypharmacy, and/or mental health issues, and/or low education and low socioeconomic status.1,2 Martello et al. 3 described that individuals with multimorbidity and complex needs often have “mental health issues, medication-related problems, and social vulnerability” (p. 1). These individuals are prone to experiencing physical, emotional, and psychological suffering due to disease burden, ongoing and emerging symptoms, and lack of personal and health system resources.4–7 Suffering refers to “an unpleasant or even anguishing experience, severely affecting a person at a psychophysical and existential level,” 8 p. 1 and it affects the general well-being and quality of life of these individuals.6,7 Suffering is also theorized as dissatisfaction for individuals and abstracted in terms of their, “struggle, despair, longing, and being cut off from a relation,” 8 p. 1356. The complexity of these individuals’ health and social care needs can make them prone to ongoing disease burden and suffering. Therefore, they frequently access health care services and are readmitted to hospitals to seek guidance for managing their multiple illnesses and suffering.9–11 Based on the data of 38,156 adults on hospital readmissions, it was estimated that 35.3% of individuals with multimorbidity and complex needs that were readmitted, particularly greater risk of readmission was for those with socioeconomic disadvantages (most vs least quintile, adjusted Odd Ratio (aOR) = 1.32, 95% CI 1.08–1.61) and those with no insurance (aOR=1.28, 95% CI 1.21–1.36). 12
Caring for and alleviating varied suffering of individuals with multimorbidity and complex needs is essential yet can be challenging for nurses.4,13 Nevertheless, it is their ethical and moral responsibility to ensure alleviation of these individuals’ suffering.4,14 Previous research explored experiences and perspectives of health care professionals about caring for and barriers and facilitators to care for individuals with multimorbidity and complex needs in primary care settings.13,15–17 However, to date no studies have explored nurses’ experiences of alleviating the suffering of these individuals during their readmission in acute care settings. Alleviation of suffering is one of element of providing compassionate care.4,14 Research demonstrated that individuals with multimorbidity and complex health needs expect nurses to be sensitive, non-judgmental, and empathic during care encounters. 4 A comprehensive understanding of how nurses incorporate these as well as additional behaviors in alleviating the suffering of these individuals can be valuable for improving the delivery of quality care to these individuals. Therefore, it is essential to explore how nurses try to alleviate suffering of these individuals and deliver social compassion with careful consideration of sociocultural determinants and contexts. Additionally, Manning and Gagnon 2 highlighted a dearth of empirical research on experiences of nurses in caring for patients with multimorbidity and complex needs and how they support and address patient complexity in care and clinical settings. Therefore, this study focused on bridging this research gap by generating an account of nurses’ experiences focusing on alleviating the suffering of this population.
Aim
The aim of this study was to describe the approaches used by nurses to alleviate the suffering of individuals with multimorbidity and complex health needs in acute care settings.
Methodology
Design
A qualitative descriptive design was used because it allows for studying a given phenomenon in a naturalistic context.18,19 In qualitative descriptive studies, a greater emphasis is placed on understanding the subjective views of participants in their natural settings 20 and generating “largely unadorned answers” for informing research and practice, 18 (p. 337).
Setting and sample
All the nurses working in two hospitals in Islamabad, Pakistan, were invited to participate through the hospital management and flyers. These hospitals have both inpatient and outpatient settings, and many complex patients visit these hospitals daily. An estimated number of complex patients visiting these hospitals was 25-30 per week. The purposive sample consisted of nurses working in inpatient care settings. The inclusion criteria were: nurses above 18 years of age, nurses with a degree or diploma in nursing, nurses with at least 6 months of working experience, and nurses who stated that they had cared for patients with multimorbidity and complex health needs.
Data collection
The data collection was completed from October 2020 until January 2021, using a semi-structured interview guide. The guide included questions about demographic information. The interview questions explored nurses’ definitions of individuals with multimorbidity and complex needs (i.e., complex patients) and the nature of their suffering, their challenges, their experiences of caring for individuals with multimorbidity and complex needs and alleviating their suffering, and strategies used to effectively address suffering in these patients. The interview guide was evaluated and revised after interviews with three nurses. After this evaluation, additional questions were added asking nurses to share clinical experiences of caring for individuals with multimorbidity and complex needs, their needs and care approaches, and the effect of social and cultural factors on the care of individuals with multimorbidity and complex needs, their suffering, and nurses approaches to alleviate this suffering.
Two researchers conducted online interviews in both English and Urdu using Zoom (https://zoom.us/). One researcher had a masters’ degree and the second researcher has a doctorate and both have experience in conducting qualitative interviews. During interviews, the participants were respected and listened to attentively. Probing questions (tell me more about this, could you please elaborate, please clarify) were used to explore their perspectives. The researchers noted personal interpretations and observations about the participants’ responses and non-verbal cues of the participants and the settings. In total, 19 interviews lasted for 22 to 61 min, with an average duration of 37 min. After 17 interviews, no new responses emerged as the sample was homogeneous in terms of clinical settings. Two additional interviews were conducted to assess data saturation.
Data analysis
The data were analyzed using reflective thematic analysis.21,22 The interviews were transcribed by two bilingual researchers, and the transcripts were entered into MAXQDA Plus 2020. The verbatim transcripts were read several times to develop a broad understanding of the participants' responses. The initial codes were developed using an inductive approach that allows for data-driven, and in vivo coding21,22 and are consistent with the qualitative descriptive approach. 20 The codes were collated based on their similarities and then refined. The refined codes were collated into preliminary sub-themes, and the sub-themes were refined and collated into final themes based on their significance, content, and meanings. Finally, the final themes were named to capture the abstract meaning of the underlying themes.21,22 During data analysis and interpretation, both the researchers were attentive of personal biases of working as nurses with this patient population and therefore maintained a reflexive stance. Each of the researcher refrained from making presumptive claims about the data.21,22 The researcher worked together to refine codes and generate themes by focusing on making sense of varied representations, intersecting and disconnected meanings, and resolving the disconnected meanings of nurses experiences of caring for this population. Thematic maps were used to develop a visual understanding of these representations and intersecting and disconnected meanings. The provisional themes were continuously refined before finalizing to ensure that they adequately capture the essence of nurses experiences.
Rigor and trustworthiness
We used the methodological bricolage metaphor to establish rigor. 23 It involves using analytical moves to understanding the phenomenon through a flexible use of relevant data collection, analysis, and interpretation methods. This approach enhances the trustworthiness of qualitative research by cobbling multiple methodological decisions and choosing a combination of analytical moves. We used the following analytical moves. The data analysis was conducted collaboratively by two researchers. Reflexivity was used during data analysis and interpretation by keeping reflective journals. During data analysis, the themes were developed by staying close to the data and the processes and decisions noted. The use of software allowed for keeping an audit trail. The transcripts and developed themes were returned to 11 participants for verification and comments (member checking). Thick description of study findings was provided by using relational and interpretive account. 24 These strategies contribute to establishing credibility, transferability, confirmability, and dependability. 25
Ethical considerations
The ethical approval (Approval Number: F, 2/IUIC-ANMC/EC-233/2020) was obtained from the Ethical Review Committee of Al-Nafees Medical College, Islamabad, Pakistan. We reminded the participants of their right to withdraw from the study until the end of data collection, and assured them of the confidentiality of information and non-disclosure of identity. We encrypted the data and the computers, and only the researchers had access to the data.
Findings
In total, 11 male and eight female nurses were interviewed. The age ranged from 25 to 38 years, and the clinical experiences ranged from 2 to 14 years. Most nurses worked in general medical and surgical units, and other nurses worked in cardiac, critical care, emergency, higher dependency, and transplant units. Of 19 nurses, 16 nurses had a bachelor’s degree in nursing. Two nurses had a master's degree, and one nurse had a three-year nursing diploma.
Themes
Codes, sub-themes and themes.
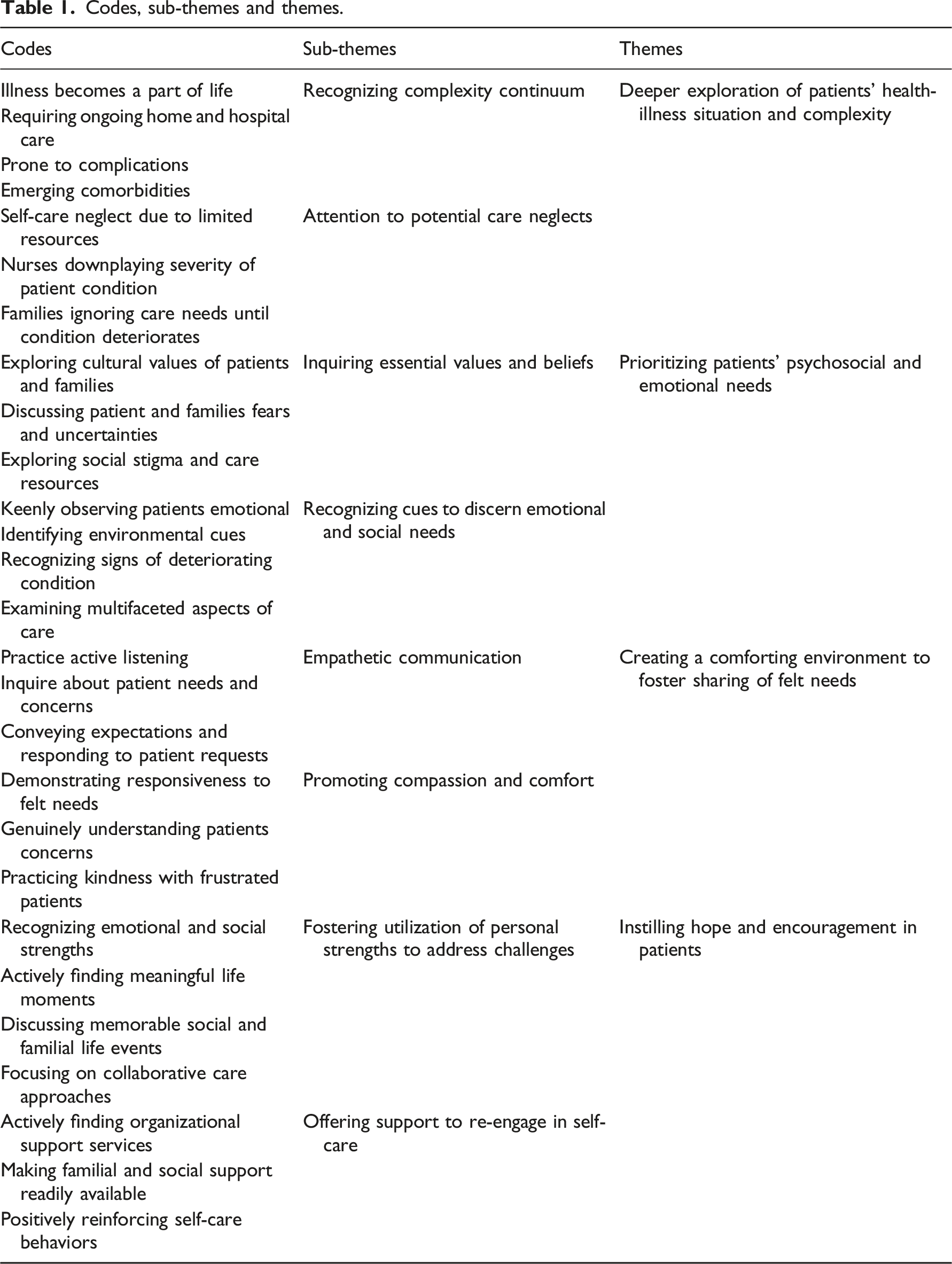
Deeper exploration of patients’ health-illness situation and complexity
Nurses discussed that alleviating the suffering of individuals with multimorbidity and complex needs requires them to fully explore the complexity of patients’ health care problems and illness situations to discern the severity of suffering and level of required care. Nurses noted that individuals with multimorbidity and complex needs have unpredictable health conditions, limited ability to perform activities of daily living, disturbed social, familial, and personal lives, and negative influence of sociocultural and structural determinants on their illness management and suffering. Therefore, the source of the suffering of these patients can be intricate and contingent on the number and nature of health complications, resources for home and social care, psychological ability to accept their illness as a part of their lives, and momentum to self-manage their issues. One of the nurses alluded to the complexity of the health-illness situation and the need to address the ongoing and emerging needs of these individuals. “You work in a ward, and your patient is hemodynamically stable or does not have any physiological problems, but it is possible that he might be facing psychological problems, social problems, and economical problems due to readmission and disturbance in the family process. In my view, caring for patients with multimorbidity and complexity like these, the first thing you do is assess and/or observe their level of complexity in a physical, social, and psychological sense and the negative impact of the complexity on the patient’s well-being” (Nurse, Male, Age 29).
Nurses discussed the deeper exploration of patients’ health illness situation also entails discerning when, why, and how an individual with complex needs could reach an extreme level of complexity. Nurses noted that many personal, social, and family-related factors could lead individuals with multimorbidity and complex needs to reach an extreme level of complexity. The described factors were financial issues, stress and frustration, disease burden, limited home and community care, greater emphasis on cultural and traditional approaches to care, and care neglect. They expressed the need to be aware of these issues and planning care approaches to target these aspects. One of the nurses highlighted the importance of deeper inquiry of patients’ issues and a potential way to alleviate their suffering. “Nurses need to go beyond superficial conversation with the patients. They should explore the health history and personal and social issues which could be leading to deteriorating health and more suffering of these patients. Nurses should be knowledgeable about the complex needs and issues of patients. If they can know more about these patients, their issues of care at homes and communities, and their needs in the hospitals, they can provide care that is effective for alleviating suffering” (Nurse, Female, Age 28).
Prioritizing patients’ psychosocial and emotional needs
Nurses noted that alleviation of suffering requires being attentive and sensitive to the psychosocial and emotional needs and issues of individuals. They expressed that while most of these individuals are readmitted to the hospitals with physical and mental health issues, the more prominent contributing factors to their suffering are their psychosocial and emotional needs and issues. They elaborated that these individuals have three types of needs: (a) physical or hospital-based needs, (b) home and community-based and felt needs conceptualized as psychosocial needs, and (c) emotional needs aggravated by disease and distress or mental health issues. Therefore, addressing their suffering requires nurses to care for physical needs, but also prioritize intricate psychosocial and emotional needs. They discussed the need to discern these needs through inquiries, observations, and assessment of unpredictable patient health issues. The inquiries should explore patients’ cultural and personal values, emotional needs, concerns and fears, socioeconomic issues, and family and care provider-related issues. One of the nurses elaborated on the importance of attending to multiple aspects of care for alleviating suffering. “We need to focus on the psychological, physical, emotional, and social care of the patients. All of these aspects should be attended to while developing a care plan for individuals with multimorbidity and complex needs. So, at each time you need to care for multiple aspects. If you are providing physical care, at the same time you need to offer psychological and emotional care. It is also important to assess the social circle of the patient and identify the kind of social, psychological, and emotional support in the home and community settings. We would have to inquire about the support of family, friends, and social groups and ask about the patient’s satisfaction with the quality of life. So, nurses should identify these needs and provide as much psychological support as they can to improve general well-being” (Nurse, Male, Age 31).
Nurses expressed the need to know about their patients’ lives, needs, and capacities to care for themselves at home and in the community as well as family issues and social issues that can aggravate their psychosocial and emotional suffering. They discussed that when attention is paid to the broader social needs, nurses need to take the initiatives to address social needs. One of the nurses described the interplay of social factors contributing to patient suffering and how nurses can help address patient suffering through comforting acts, but also advocacy, and referral to appropriate agencies. “Many individuals with multimorbidity and complex needs are frustrated with their life and living conditions as they do not have the basic necessities of life. We cannot fully help them with such kinds of issues and can only refer to them for financial support to Bait-ul-Mall and Zakat center. But we can try to improve their experiences of care when they visit health care settings. For emotional care, we often see that those who are poor receive differential treatment in our culture. Rich people do not want to talk to these poor people at all. So as nurses if we are able to share some good moments with these patients, listen to their issues, and support them in simple ways; it could be really comforting to them. This can greatly help in addressing their suffering resulting from social factors” (Nurse, Female, Age 29).
Creating a comforting environment to foster sharing of felt needs
Nurses recognized the need to create comforting environments to foster patient sharing of their issues and felt needs and enhance the development of therapeutic relationships. They noted that nurses’ kindness and empathic communication with patients are two crucial elements of a comforting environment. Nurses noted that practicing kindness is of utmost importance for learning more about patient needs, developing effective relationships, addressing their suffering, and improving their recovery. Nurses discussed kindness is manifest in empathetic communication conceptualized as nurses’ ability to genuinely talk with and listen to patients and interpret their hidden issues. Empathetic communication is conveying personal expectations to patients and responding to their requests. One of the nurses shared how nurses’ need to practice compassion could improve nurse–patient relationships and care. “Individuals with multimorbidity and complex needs expect health care professionals to understand their values and respect them. We as nurses should be truly attentive to the needs of these patients. We should learn about kind behaviors that are useful for dealing with individuals with multimorbidity and complex needs. Our behaviours and communication should be kind so that these patients can develop a trustworthy relationships. Politeness is at the heart of kindness and effective communication. When this happens, these complex patients feel comfortable interacting with the health care professional and willingly allow them to get involved in difficult decisions” (Nurse, Female, Age 37).
Nurses elaborated that creating comforting environments to foster sharing means becoming a part of patients’ social lives and avoiding actions and behaviors that could be threatening to them and are not aligned with their cultural values and beliefs. It is more than just comforting them and entails genuine encounters demonstrating interest in their lives. Nurses noted that during any encounter, patients should get an impression that the nurse is truly invested in exploring their issues and assisting them in overcoming suffering. One of the nurses discussed how practicing kind communication and demonstrating genuine interest in patients can help create a comforting environment, thereby alleviating their suffering. “If I am communicating with kindness to the patient, I have become a part of his social life. Now, when I engage fully with them, they would openly discuss a lot of things about their life. Like a person who is frustrated; until we communicate with kindness, that person would not be willing to share their issues, and would keep the problems to themselves. Patients explore their social connections and think about how and to whom they can trust and share their problems. So, if nurses try to become part of patients’ social life through genuine interest and if the nurses demonstrate kind behaviours, the patients will be comfortable in sharing their issues with them. When patients can share their sensitive issues with nurses, this is a way of alleviating their emotional stress and suffering” (Nurse, Male, Age 30)
Instilling hope and encouragement in patients
Nurses greatly emphasized the need to instill hope and encourage patients to manage their multiple chronic health issues with guidance from nurses. Nurses shared the observations that often when these patients are readmitted, they are frustrated and exhausted with the health care process and bureaucratic system that offer limited support. Therefore, they noted that one of the essential nursing tasks is to identify available external support resources for the patients and facilitate them in effectively using those resources. The necessity to instill hope and encouragement was considered valuable to help patients manage emotional turmoil and develop resilience to alleviate their own suffering originating from sociocultural, familial, and health care system-related challenges and deteriorating multiple chronic illnesses. Nurses emphasized the need to address the emotional issues of patients because these issues can affect nurses ability to care for these patients. One of the nurses offered an account of patients’ frustration and nurses’ role in assisting patients. “These patients are often frustrated with the health care process and system, and you can see that frustration in their behaviours. Many patients are exhausted and frustrated due to longer stays in the hospital than expected and the negative behaviours of health care professionals. Due to this frustration, sometimes, these patients even refuse any sort of medical or nursing care. In these situations, the first step is to support them and offer reassuring words to motivate them to take care of themselves. We should not only inspire them but work with them and be there for them so that they know that we have not left them in limbo” (Nurse, Female, Age 38).
Nurses considered patient encouragement and enhanced hope integral to addressing their suffering. They expressed that working with them and helping them understand their psychosocial, emotional, and physical issues comprehensively without imposing personal interpretations. When patients are supported to address their own issues, they are better able to identify their needs, resources, and competencies, and seek guidance from nurses as the need emerges. Nurses noted that hope and encouragement for patients that they can control their issues contribute towards boosting their confidence and morale in managing complex multiple chronic illnesses. This, in turn, serves as a mediator in enabling them to address their own suffering. One of the nurses illustrated how she was able to instill hope and encouragement. “I cared for a patient with dialysis who also had heart-related issues. His main need was to achieve emotional contentment and alleviate emotional distress. He was frustrated and distressed due to his complex health issues and had talked about giving up his life. To provide effective care, I knew I had to better understand his felt needs. I knew that I had to learn more about his emotional needs and views on his health issues. Some of his emotional needs were connected to unmet physical needs. I used to sit with him during each shift for 15 to 20 minutes, listening to him and offering my knowledge of his illness. I used to tell him ‘you’ve got this’ and ‘let’s keep going’. He stayed with us for 7 days, and I saw marked improvement in his ability and motivation to care for himself. I think I tried my best to manage his physical issues as well as emotional distress so that he could achieve greater contentment. Nurses also need to develop tolerance and patience to meet the felt needs of patients adequately” (Nurse, Male, Age 28).
Discussion
This study aimed to describe nurses experiences of alleviating suffering of individuals with multimorbidity and complex needs in acute care settings during readmission. Nurses shared that these patients have multifaceted health and social care issues and their lives are affected by many sociocultural and structural determinants of health contributing to their psychosocial, emotional, and physical suffering. In order to alleviate these varied forms of suffering, nurses emphasized the need of deeper inquiry into patients illness situation and complexity to discern the impact of determinants on their well-being and developing care plans that are tailored to meet the needs of these patients. Consistently, Webster et al. 13 noted that physicians and nurses moved beyond the narrow view of multimorbidity and complexity and focus on exploration of intertwined sociocultural determinants (living conditions, poverty, and socioeconomic status) on their care. They noted that nurses often have to move beyond their learned skills and competencies to offer quality care to this population. Younas 14 also emphasized the necessity for nurses to deeply inquire patients’ situation and identify interpersonal, intrapersonal, and contextual factors affecting the understanding and alleviation of suffering. Therefore, nurses should be more sensitive and observant of the impact of sociocultural and structural determinants on these patients’ perception and experience of their multimorbidity and complexity, and use this knowledge to design concrete strategies to alleviate patient suffering.
Patients with multimorbidity and complex health needs experience suffering originating from sociocultural factors and encounters and the need to adapt their lives for accommodating multimorbidity.4,7 These patients are also susceptible to experiencing suffering in social aspects of their lives such as balancing autonomy, addressing the needs of their families, and ensuring living a meaningful life. 5 This underscores the importance of attending to their psychological and emotional needs and moving beyond a single disease approach to more integrated care. The nurses in this study highlighted that prioritization of psychosocial and emotional needs over physical needs might be more relevant to alleviating the suffering of this patient population. A recent systematic review 26 also highlighted that providing psychological support to patients with complex needs is instrumental in addressing disease burden and mental health, thereby reducing experiences of inflicted suffering. Therefore, nurses should be aware of the psychosocial and emotional needs and associated suffering and take necessary initiatives to help these patients.
Creating comforting environments to promote patient sharing of their emotional, psychosocial, and physical issues and distress was identified as a useful approach to develop therapeutic relationships, address suffering, and improve their recovery. Younas 14 argued that patient suffering is personalized and variable influenced by hidden factors and vary across sociocultural situations. Therefore, nurses have an ethical responsibility to ensure that their interactions with patients are non-judgmental and genuine for allowing patients to share their lived experiences of suffering. Hueso Montoro et al. 27 also articulated the need to develop a trustworthy relationship with patients to allow them comfortable sharing of their implicit suffering and the influencing determinants. Therefore, nurses should devote extra efforts to establish a therapeutic relationship, and comforting environment to foster sharing. Emphasis should also be placed on adequate training of nurses and nursing students to enhance their skillset and abilities to develop such caring and comforting environments.
Instillation of hope and encouragement are essential aspects of promoting patient empowerment to make an effort to address their own suffering and needs. The nurses elaborated that merely encouraging patients and/or boosting their morale is not enough and nurses should be actively involved with them in their decision making without imposing personal choices and decisions. A systematic review also highlighted the need for greater involvement and empowerment of complex patients in their disease process, management, and care planning. 28 The nurses in this study shared that when patients are offered opportunities and resources to actively participate in their care and alleviation of suffering, it boosts their confidence to better engage in care at home and in the community settings.
This study offers some evidence that alleviating suffering of patients with multimorbidity and complex health needs may be more daunting and challenging for nurses compared to the general patient population. This claim is supported by the finding that there is more focus on the social aspect of suffering in these patients and its threatening consequences to patients general well-being and relationships with their families and health care professionals. The nurses in this study highlighted that owing to the negative impact of sociocultural and structural determinants on health care access, self-management, and empowerment of patients to address their own suffering, patients often become frustrated with nurses which influence the delivery of quality care. Given this, it is critical that nurses are mindful of the impact that multimorbidity and patients’ complex health care needs can have on their ability to alleviate patient suffering compared to when striving to care for those with single disease.
Limitations
The concept of complex patients is often confused with “critically ill” and “difficult” patients. Therefore, nurses’ caring experiences with “complex,” “critically ill,” and “difficult” patients may have influenced their views about complex patients exclusively. Nevertheless, requesting nurses to discuss their assigned meaning of complex patient before exploring their experiences allowed for minimizing the influence of interrelated terms. Our sample comprised of nurses from South Asia and patients’ suffering is often intertwined with sociocultural context and the challenges within a given context. Therefore, Further research in other contexts and may provide different insights into nurses’ experiences of alleviating suffering. Interviews were conducted in Urdu language and then translated; there is a possibility of losing meaning of participants experiences.
Implications for research
Several areas for future research can be generated from this study. First, this study offered some insights about how determinants of health can influence the health experiences of individuals with multimorbidity and complex needs and care delivery. However, future studies should develop a greater understanding of the impact of social determinants of health on patients’ experience within the health system from the patients’ and their families’ perspective. Second, Future research could also explore nurses views about identifying and addressing psychosocial needs, designing care plans, and test nurse-led interventions to alleviate patient suffering. Third, Further research can focus on using mixed methods approaches to develop data collection instruments determining the levels of quality of care, barriers and facilitators to alleviating patient suffering, and more interventions targeting patient suffering through comparative analysis of patients with multimorbidity and complex needs and those with single disease. Finally, future research is warranted to develop a comprehensive understanding of the nature of comforting environments that promotes sharing of suffering from patients as well as nurses perspective.
Conclusions
Alleviation of patient suffering is an integral aspect of compassionate nursing care. Nurses used a multifaceted approach entailing sensitive understanding, deeper exploration of patients’ issues, recognition of sociocultural and structural determinants and their impact on patient situation, and altruistic actions to alleviate patient suffering. Nurses focused on attending to patients’ cultural and social values, identifying support services, and instilling hope and encouragement in them to facilitate them in working collaboratively to alleviate their suffering. Future research should focus on tailoring and operationalizing these approaches to improve the quality of care provided to these individuals with multimorbidity and complex health needs by designing and testing nurse-led interventions to alleviate patient suffering.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.