
Abstract
Research question and aim
Clinical Ethics Committees (CECs) aim to support healthcare professionals (HPs) and healthcare organizations to deal with the ethical issues of clinical practice. In 2020, a CEC was established in an Oncology Research Hospital in the North of Italy. This paper describes the development process and the activities performed 20 months from the CEC’s implementation, to increase knowledge about CEC’s implementation strategy.
Research design
We collected quantitative data related to number and characteristics of CEC activities carried out from October 2020 to June 2022 using the CEC internal database. Data were reported descriptively and compared with data from the literature to provide a complete overview of the CEC’s development and implementation process.
Participants and research context
The study has been conducted at the local health authority (LHA) of Reggio Emilia. It is a report of the activities provided by the CEC, where no HPs or patients were involved.
Ethical Considerations
The report is part of a larger study named EVAluating a Clinical Ethics Committee implementation process (EvaCEC), which has been approved by the Local Ethics Committee (AUSLRE Protocollo n° 2022/0026554 of 24/02/2022). EvaCEC is also the first author's PhD project.
Findings
In total, the CEC performed 7 ethics consultations (EC), published three policies related to particular ethical questions of clinical and organizational practice, provided one educational online course on ethics consultation targeting employed HPs, and promoted a specific dissemination process among the different departments of the LHA. According to our results, the CEC widely fulfilled the standard threefold set of clinical ethics support services tasks (namely, ethics consultation, ethics education, and policy development), but further investigations are needed to evaluate the CEC’s impact on clinical practice.
Conclusion
Our findings may increase knowledge regarding the composition, role, and tasks of a CEC in an Italian setting, informing future strategies and efforts to regulate these institutions officially.
Introduction
The shared decision-making process in the healthcare setting is often challenging due to unavoidable uncertainty about consequences of treatments and deep-seated value differences of the person involved. In response to the need of patients, families, and healthcare professionals (HPs) of assistance in addressing the ethical issues of the daily clinical practice, clinical Ethics Consultation (EC) has increasingly been implemented within healthcare organizations over the past 30 years.1,2
EC is defined as “a service provided by a committee, team, or individual to address the ethical issues involved in a specific clinical case.” 3 The EC services are known as Clinical Ethics Support Services (CESSs). CESSs represent a type of ethical intervention that aims to promote a personalized care approach while improving the process and outcome of patient’s care by reducing conflicting situations, promoting the ability of HPs to recognize and manage the personal preferences and values of vulnerable patients, and supporting decision-making in ethically complex situations. 2
Clinical Ethics Committee (CEC), one of the most common forms of CESS,4,5 is a standing, independent body established by a healthcare institution whose task is to consider, discuss, and promote educational initiatives and to provide advice or recommendations to HPs concerning the best course of action in a specific clinical case or discussion that leads to a good decision-making process. 6
Although CEC are quite common worldwide, 7 in Italy, they are mainly slowly growing entities, resulting from voluntary local efforts rather than national impetus. 8 According to the Italian Ministerial Decree of 8 February 2013, 9 EC is an option whose organization is demanded by the Research Ethics Committees (RECs), the independent bodies responsible for ensuring the rights, safety, and well-being of subjects enrolled in clinical studies. EC does not represent the RECs' primary function and might represent an excessively burdensome workload. 10 Despite the Ministerial Decree, some Italian regions established CECs in the last 10 years by regional resolution. 8 It must be noted that in February 2023, a new Ministerial Decree related to the reorganization of RECs entered into force, according to the European regulation, but the tasks related to ethics consultation have not been modified. 11
On 13 July 2020, the Clinical Ethics Committee (CEC) was established by the General Directorate of the Local Health Authority (LHA)–Azienda USL-IRCCS of Reggio Emilia (AUSLRE Deliberation 2020/0224 of the 1307/2020) as a consequence of the Covid-19 pandemic outbreak and its ethical implications.12–14 The first meeting was on 10 October 2020.
This report aims to provide a preliminary description of the CEC’s development process and activities performed after 20 months from its implementation. It is part of a larger research project called “Evaluating a Clinical Ethics Committee (CEC) implementation process in an Oncologic Research Hospital. A process evaluation study using Normalization Process Theory’. It is a mixed-method study aiming to determine the mechanism for the successful implementation of a CEC in a hospital setting by means of normalization process theory. Quantitative and qualitative methods are integrated to collect crucial variables of the implementation process and to get a more accurate appraisal of the work required for the CEC to become a “normal” part of the hospital system. 15
Background and research context
The Clinical Ethics Committee (CEC) was established at the Local Health Authority (LHA) of Reggio Emilia, which is the single public healthcare company in the province of Reggio Emilia, Italy. LHA is a part of the Regional and National Health Service; in Reggio Emilia, the LHA, organized into six healthcare districts, provides health and social care, hospital services, and primary care. The LHA Hospital Service consists of six hospitals (one for each district), which work together to coordinate, develop, and provide high-quality services. Finally, a Scientific Institute for Research, Hospitalization and Healthcare (IRCCS) in Advanced Technologies and Care Models in Oncology is incorporated into the Reggio Emilia hospital. A total of 1500 beds are provided by the LHA, with 180 beds dedicated to oncology patients. The CEC intervention targeted all the HPs employed by the LHA of Reggio Emilia.
As part of the research activity on the care models in oncology, in 2016 a Bioethics Unit (BU) was implemented with the aim to assess and promote quality of care for patients, family caregivers, and HPs throughout empirical bioethics research projects, educational and training programs, and EC activities.
The projects are focused on developing, implementing, and evaluating new and innovative bioethical interventions at the hospital and community level. These interventions are dealing with ethical issues (i.e., informed consent, shared decision-making, end-of-life issues, pediatric issues, patient engagement, truth telling, decision-making capacity, and healthcare costs) in clinical practice and they integrate empirical analysis into ethical theorizing.
The CEC is one of the experimental bioethical interventions promoted since 2020.
Structure and working of committee
The composition and tasks of the CEC were delineated in line with data from the scientific literature, 16 and the recommendations of the Italian Committee for Bioethic’s Opinion. 10
Composition
CEC’s components characteristics.
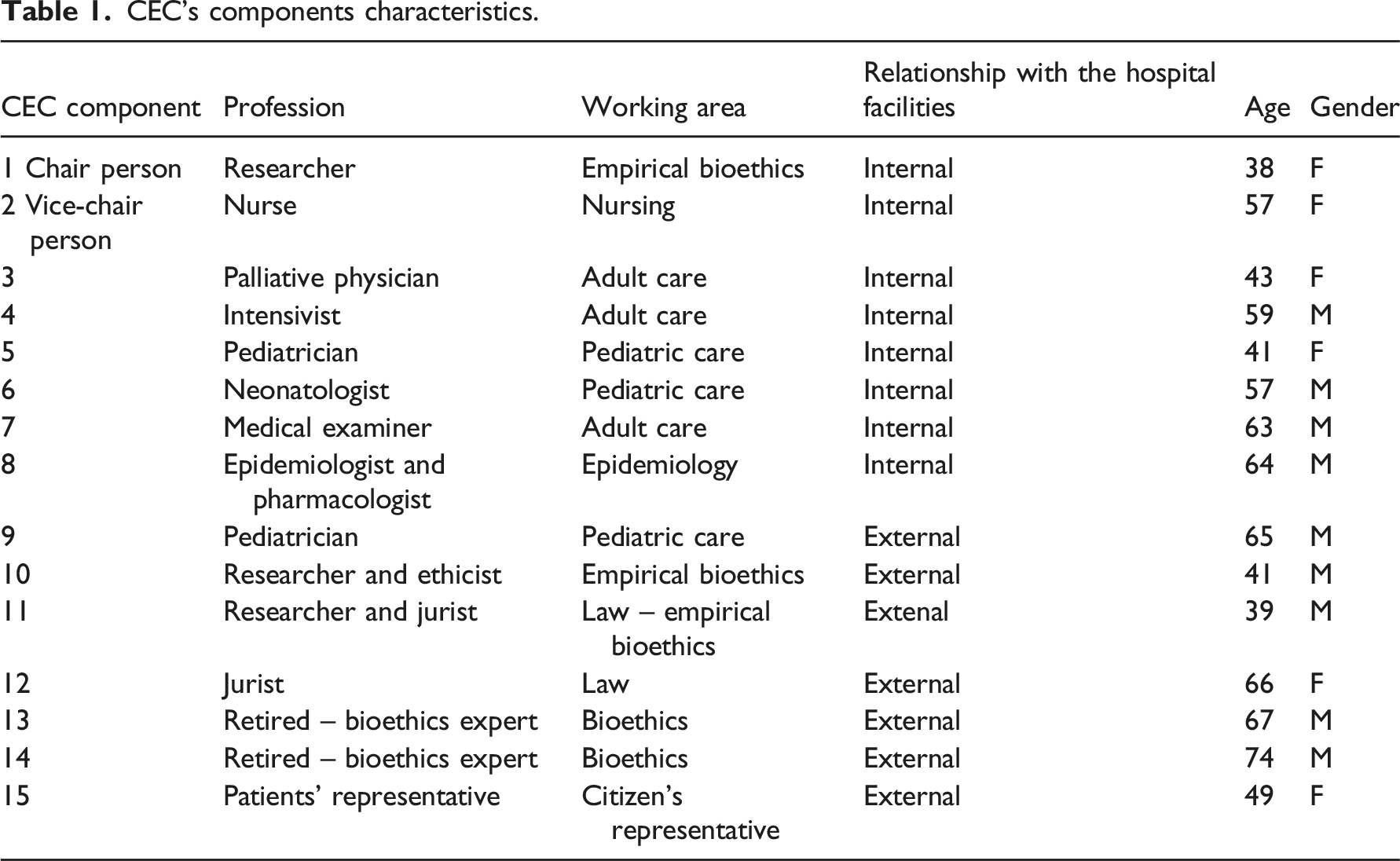
According to the CEC Regulation, the Chairperson can occasionally allow other HPs to participate in EC deliberation, but only in decisions where their presence appears necessary according to the patient’s needs (e.g., religious, cultural mediators, psychologists, and social workers). Due to experimental nature of the CEC, the components were selected personally by the Head of the BU according to their competencies and expertise in their field.
CEC is also provided by a administrative office, responsible for the back-office activities.
Role, tasks, and procedures
The CEC Regulation established the nature, aims, functions, and procedures of the CEC. It has been discussed and approved by all the members of the CEC during the first meeting. The Regulation has been deliberated on 11 November 2020 (AUSLRE Deliberation 2020/0391 of the 17/11/2020).
CEC is responsible for: a) evaluating clinical cases that are not part of the clinical and pharmacological experimentation, both retrospectively and prospectively (ethics consultation); b) analyzing the moral problems related to clinical practice (e.g., ethical aspect of allocation resourrces criteria, Withdrawing and withholding treatments, request for medically assisted suicide, minors and consent, substitute decision-makers, the ethical aspect of communication, and immigration issues) and the development of policies on specific moral issues (policy development); c) supporting HPs in their clinical practice when particular ethical issues emerge, also in urgent/critical situations; d) proposing public initiatives to develop the bioethical awareness among citizenship; and e) proposing and conducting institutional ethics training program targeting HPs (ethics education).
Guide for the formulation of Ethics consultation request.

EC requests are discussed during regular meetings by all CEC members or, in specific cases, by a subgroup identified by the CEC President based on the competencies and appropriateness requested. If necessary, the President can specifically recommend that external experts attend the CEC meetings to provide their qualified advice.
Methods
Quantitative data on the CEC’s activities from October 2020 to June 2022 were collected in relation to: i) Characteristics of the activities provided, in terms of: a) meetings performed, b) EC’s provided, c) ethical policies development, d) educational courses in ethics promoted, and e) dissemination. ii) Hours spent by the services for each activity. iii) Resource employed by the service.
Data were collected from the internal database of the CEC’s administrative office and have been analyzed by descriptive statistics. Data are presented descriptively, and compared with data from the literature, to provide a complete overview of the CEC’s development and implementation process.
Ethical considerations
This article is part of a larger research project called “Evaluating a Clinical Ethics Committee (CEC) implementation process in an Oncologic Research Hospital. A process evaluation study using Normalization Process Theory’’ regarding the implementation and evaluation of a CEC in an Oncological Research Hospital in the North of Italy (Protocol approval: 1085/2021/OSS/IRCCSRE). Since it is a report of quantitative data, no human subject was involved in this study and any informed consent was required.
Findings
Meetings
From October 2020 to June 2022, the CEC performed 16 meetings, with an average duration of 1 h and 50’ (range 1h–2h40′), for a total of 25 hours. All the meetings were conducted online. Four meetings were not performed due to the lack of quorum and lack of EC requests. Two members (the citizens' representative and one expert in bioethics) retired for personal reasons and only the Citizens’ representative was replaced.
During the sessions, the main topics were as follows: a) discussions of the EC requests; b) discussions and revisions of policy or recommendations on particular ethical questions arising from clinical practice; c) setting up of a training course in clinical ethics and EC targeting HPs; and d) relationship with other CECs to create further collaboration and national network.
All the meetings were audio-recorded, also for research goals. After each session, the administrative office elaborated a report and shared it with all the members to further check.
Ethics consultation
CEC’s activities – Ethics Consultation.
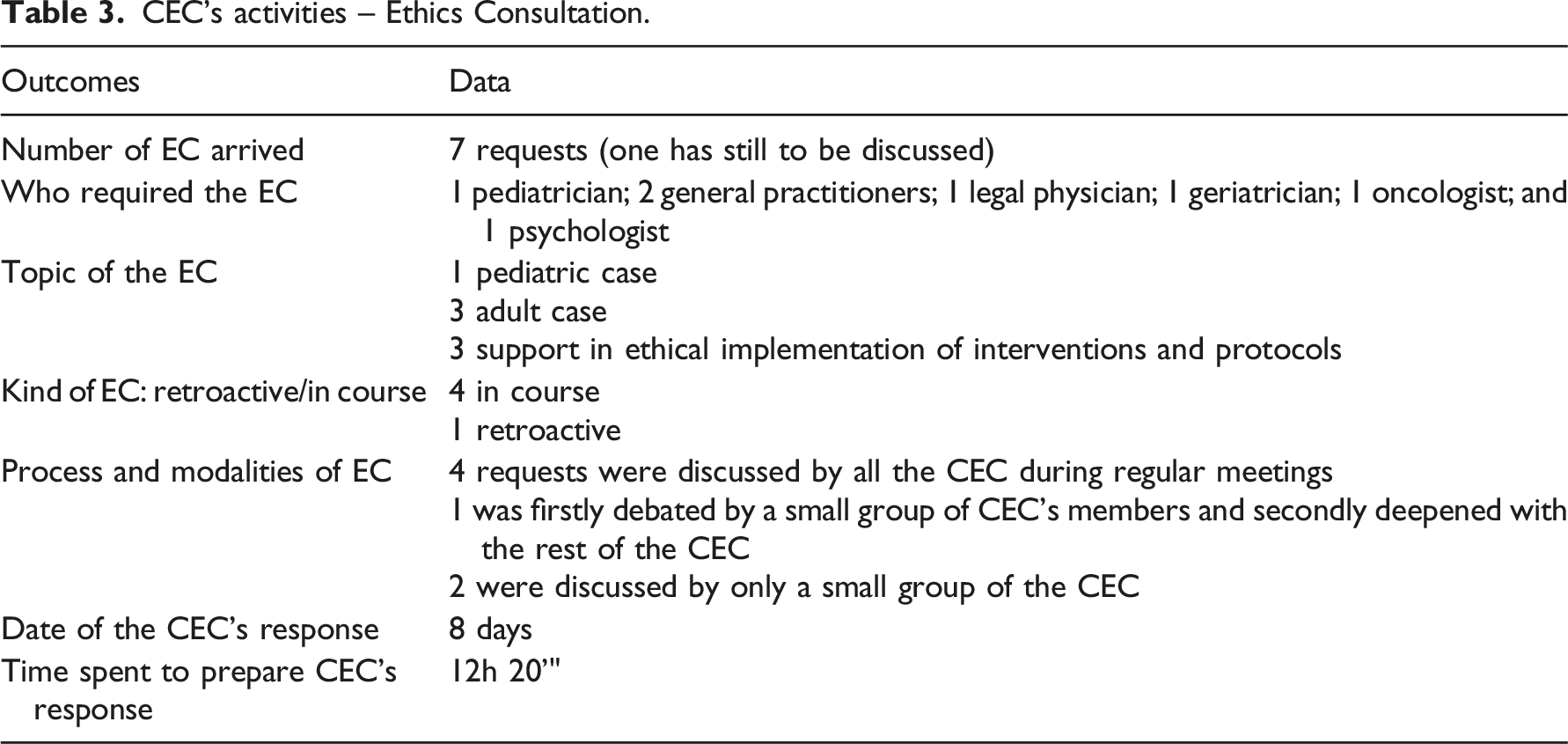
A total of 10 hours have been spent for EC. Examples of EC request are presented as follows: 1. The disagreement between two pediatric teams care regarding the children’s care goals and the options available to the family. 2. A family disagreement regarding the Covid-19 vaccination for a person with dementia. 3. A conflicts between physician, patients, and familiars related to the administration of unconventional therapy. 4. The involvement of patients with dementia in a research project. The request was declined and the CEC agreed that the RCE should discuss the case. 5. The concerns regarding the activation of a project of Art-therapy with patients recovered in a hospice. 6. The ethical questions related to the management of deep palliative sedation and existential distress. 7. The ethical aspect of screening for artificial nutrition in patients with dementia.
Before the official submission of the EC request, an informal discussion between the HP and the CEC’s President took place to let the President assess the appropriateness of the case for the CEC. Then, the HP submitted the request through the online format. The submission process consists of a brief description of the issue and the formulation of the ethical problem perceived.
During the meeting, the President introduced the ethical case with a brief description of the circumstances. Opinions, comments, and suggestions were collected and subsequently elaborated into a first-draft response. Then, the draft is sent to the rest of the components to collect further suggestions. If all the members agreed on the answer, it was finally submitted to the requiring HP. Generally, the HP was invited to participate at the next meeting. The average response time is 8 days (min.2 and -max.14 days).
Policy development
The CEC developed and published three policies related to particular ethical questions of clinical and organizational practice. They all concerned the moral aspect of care in the light of the Covid-19 pandemic.
The first document was related to the ethical problem of triage, the second one concerned the ethics of vaccination during the Covid-19 pandemic, and the last one dealt with the loneliness of patients during the Covid-19 pandemic.
The documents topics were determined by the urgency of the question, the perceived needs among HPs and patients, and the need to inform citizenship and HPs on specific ethical problems.
The documents are composed of several parts: an introduction on the topic, an ethical discussion on the different perspectives related to the subject and finally some practical suggestions to implement ethical oriented care in the local context.
The topic of each document was discussed during the regular meetings to collect opinions, reflections, and comments by all the members. Then the President elaborated the emerging issues into a first draft, which the CEC discussed during the next meetings. After reaching the consensus of all the members, the final version was submitted to the IRCCS Chief Operating Officer. Then it was published on the CEC’s webpage. A total of 13 hours were spent for this activity.
Educational course and training
An educational, online, course called Il Comitato per l’Etica nella Clinica dell’Azienda USL-IRCCS di Reggio Emilia: strumenti e servizi per gestire i conflitti etici nei contesti di cura’ has been ideated and implemented by the CEC targeting all the HPs working at the LHA of Reggio Emilia.
The course was composed of five repeated sessions, lasting 2 hours each, and has been performed between May and November 2021. A total of 10 h of training have been provided, and 192 participants attended the course. Their characteristics are provided in Figure 1. Composition of ethical courses’ participants.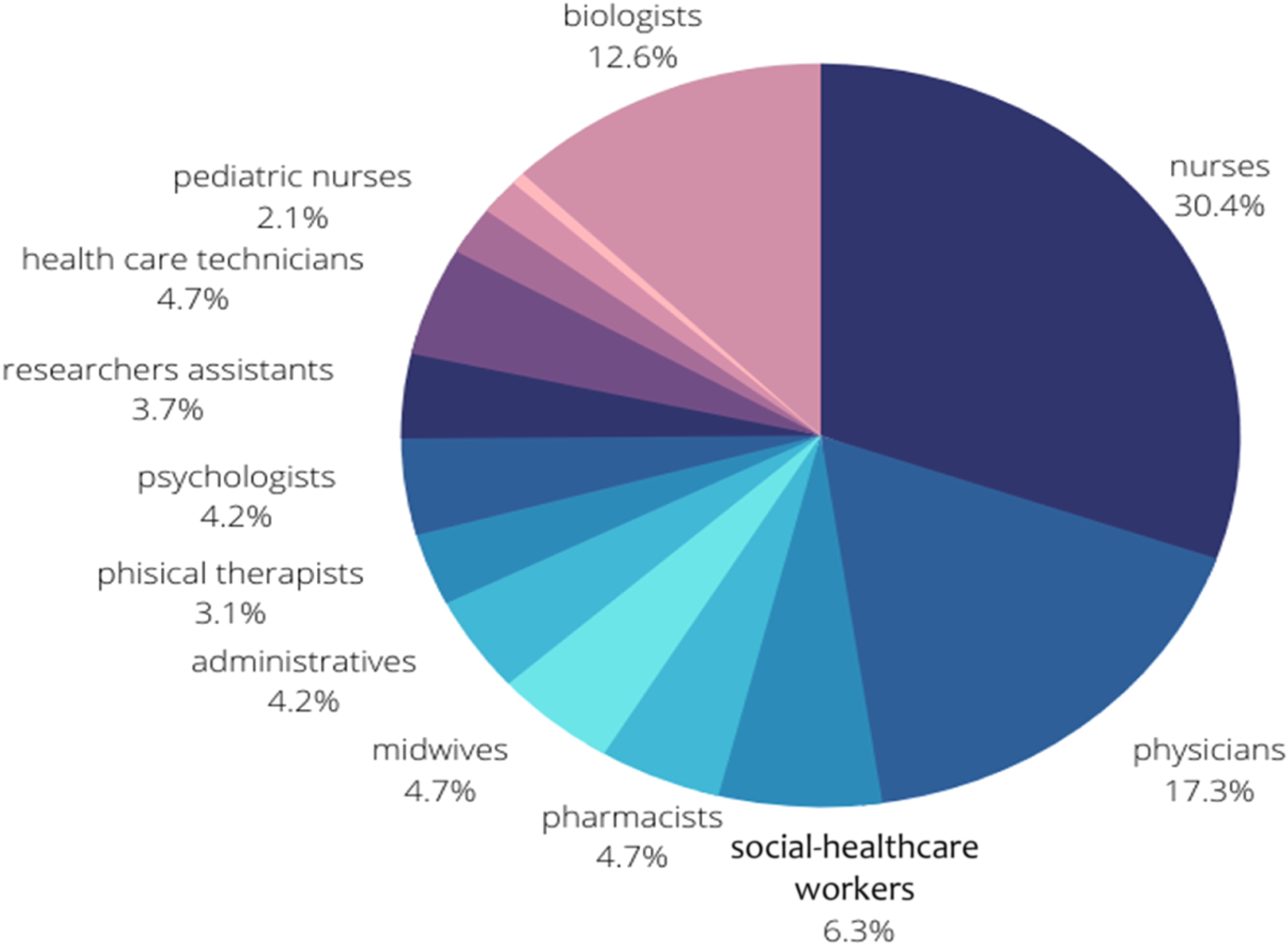
Each session was conducted by 2 external components of the CEC and was divided into several sections: an introductive part on the role, nature, the function of the CEC, a theoretical part related to EC and the role of CEC on the resolution of complex ethical situations, the discussion of a clinical case presenting a moral problem and its resolution from an ethical point of view, and a final discussion among participants.
The lessons were characterized by interaction among participants, who were attentive and interested in the topic discussed. The main questions emerged related to the practices and methods to support the healthcare team in dealing with complex cases, the access and functioning of the CEC, the ethical support in the decision-making process concerning pediatric cases, the predisposition of the healthcare team to request ethics support, the importance of ethics support to improve patient involvement in the decision-making process, and finally the complexity of decision-making and healthcare choices with psychiatric patients.
On the 6 of April 2022, an online Congress was organized by the BU and the CEC of Reggio Emilia in collaboration with the Emilia Romagna Region. It was focused on the role of ethics consultation in the healthcare relationship, the need to share experiences from local CECs’ activities and their future role within the Italian context.
Dissemination
A specific dissemination process has been provided through: 1. The creation of an online page dedicated to the CEC and targeting only HPs. 2. The creation of an Internet page dedicated to the CEC and accessible to anyone who surfs the Internet (https://www.ausl.re.it/comitato-per-letica-nella-clinica-cec). 3. The CEC illustration by the President and Vice-president during some selected Departments of the LHA, potentially interested in the support by the CEC. 4. The dissemination of the service through social channels.
Finally, we collected data on the amount of hours spent by the CEC in its activities and the resource employed by the CEC, as showed in figure Figure 2(a). Resources were considered as back off activities (preparation of meetings’ reports, organization of meetings, support in development and publication of written responses, and administrative issues). Figure 2(b) demonstrated the amount of time spent by the CEC for each activity. Amount of time (hours) spent by the CEC for each activities.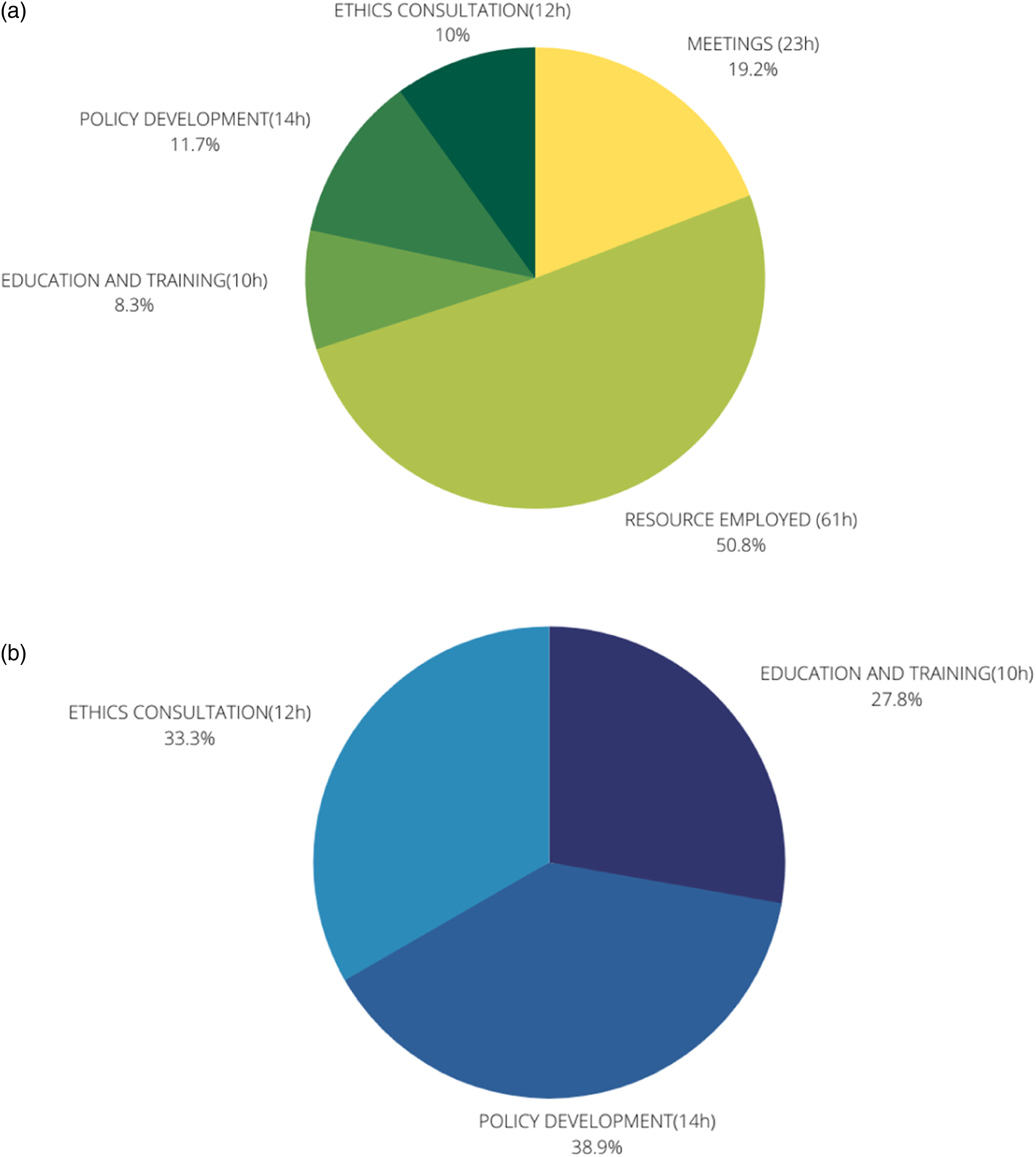
Discussion and Conclusion
Discussion
This article provides a preliminary description of the activities performed 20 months after the implementation of a CEC in an oncological research hospital in Northern Italy.
Our data demonstrated that the CEC widely fulfilled the standard threefold set of a CESS’s tasks and functions, namely, EC, ethics education, and policy development.2,17
Ethics consultation volume and the “integrated model of EC”
EC represents the main core business of a CEC, and data related to the annual volume of EC requests is increasingly seen as an essential element in understanding the CEC’s implementation and quality.18,19
It is interesting to note that our CEC received 3 EC requests in the first year, and 4 in the second. It is a considerable amount compared to both the national average of EC requests 0–1 request, 8 and the median number of American and Norwegian CECs, respectively, 3 requests 18 and 4.7. 20
We assume that this significant result is partially influenced by the activities promoted by the BU since its implementation in 2016 and, specifically, by the ethics support provided by the Head of the BU. She is a research scientist with a PhD in bioethics and expertise in research in palliative care. Along with research projects in empirical bioethics, she promoted individual EC to HPs and ethics supervision during scheduled team care meetings. Acting as a clinical ethicist, her support consisted of a proactive form of EC, aiming at supporting the development of HPs’ ethical competences to improve their decision-making process in daily clinical practice. 21
The possible interrelations and integration between different models of EC services, namely, clinical ethicist and CEC, are widely discussed among experts. With regards to our CEC, it can represent an interesting experience compared to emerging findings of EC services among USA and Europe. Indeed, our experience confirms that a high EC volume directly correlates from the presence of one or more full-time ethicists within a CEC 22 as emerged from the follow-up survey of Fox colleagues.
In a previous study, we showed that providing several activities in clinical ethics, including research in empirical bioethics, has led HPs to be progressively sensitized to the ethical aspect of care. 21 Moreover, the EC activities promoted by the bioethicist helped HPs to deal with moral distress and to develop a different perspective foster a more patient-centered decision-making process. 22 All considered, this experience may have facilitated HPs’ awareness of their need to be supported by a multidisciplinary institutional service like CEC in managing complex moral situations.
Then, the “integrated model of EC” developed at the LHA of Reggio Emilia is more in line with an American approach to EC, rather than the European one, which is more focused on the multi-professionals deliberation provided by a dedicated team, but can be a promising model, especially during the implementation phase of the service.
In the absence of a national regulation on CECs, our CEC has been developed, implemented, and evaluated as a complex intervention in clinical practice following an appropriate framework such as the MRC framework.24,25 Applying a research approach to the CEC, we can contribute to a growing number of studies emphasizing the need for a more in-depth understanding of the complex ethical interventions implemented, to explore more in detail what outcomes they explicitly aim to achieve and how they bring about change to clinical practice. 16 Implementing CESSs has always been challenging, especially in Europe, due to several issue concerning their regulation. 26 CECs has mainly been implemented through a bottom-up approach and regulation has mostly remained weak and decentralized due to the fear that too much regulation might diminish the CECs’ contribution to the development of biomedical citizenship and democratic structures in healthcare. 27 Then, CEC developed into local initiatives, answering to a perceived need to discuss moral problems in patient care, responding to hospital policy and considering the most difficult cases arising from clinical practice.28,29 Consequently, the successful implementation of CECs is still an open debate, especially as regard the best model to normalize EC in daily clinical practice.
EC deliberation and the different perspectives (not) involved: physicians, nurses, and patients
According to our data, EC was required only by physicians, although CEC’s regulation does not exclude EC requests from nurses or other HPs. Nurses, in contrast, represented the professional category attending the most in the ethical training course promoted by the CEC.
Our findings are in line with those of previous studies that showed significant differences in CEC access between physicians and nurses.
In line with previous experiences, CEC’s support is mainly required by physicians involved in contradictory cases or suffering from physician burnout,20,28 seeking moral support, confirming the appropriateness of actions, or needing clarification of the patient’s values and preferences. 29
However, nurses are HPs who, internationally, have a reputation for holding one of the highest levels of moral sensibilities that equip them to recognize and respond to moral issues. 30 They can be pivotal in promoting the analysis of ethical dilemmas and the use of ethical counseling and discussions, as stated in the Italian Code of Ethics for Nurses. 31
In this regard, it should be mentioned that in January 2023, an EC was submitted to the CEC by nurses from an Intensive Care Unit (ICU). This case was related to a complex pediatric case. Due to the timing of this report, this EC was not included in the results of this article. However, this EC was the first to directly involve nurses, who participated actively during CEC meetings explaining their perceptions, emotions, and difficulties in the case. Considering nurses’ ethical issues, the final response elaborated by the CEC included a paragraph dedicated to HPs moral distress. This experience confirms that CECs are helpful for nurses and other team members in supporting them while caring for patients at intersections with families and physicians, especially in their patient advocacy.32,33
According to Jansky et al., nurses seemed to expect CEC’s support more often than physicians because of several difficulties they usually experience in their interprofessional cooperation, such as difficulties in speaking up, inappropriate solving of disagreements, missing impact on decision-making, and lack of good nursing input not being well received. 34 Our data seem to confirm that nurses perceive more significant barriers than physicians in accessing CEC, such as lack of knowledge of CEC’s functions and roles and the hierarchical aspect of CEC. 23 Finally, this CEC deals with adult and pediatric cases and does not directly involve patients or next of kin during deliberation. Focusing EC on the professionals and not on the patient or family may increase the investment of the healthcare team toward the ethical analysis of an individual case, improving HPs’ confidence to manage similar dilemmas or professional/medical disagreement in the future. 35 However, involving next of kin in deliberation can also contribute to conflict resolution and signal that they are taken seriously. 36
Ethics education and CEC’s access
Considering education and training targeting HPs, the second CEC’s function, our findings provide several insights into its content, format, and other characteristics. First of all, participants who attended the course worked within different healthcare settings, confirming the wide transversality of the CEC and the potential interest of the service from various healthcare-related working issues.
Physicians with the least training and experience are the least likely to have access to and request EC. 37 Not feeling or recognizing the need for help in addressing ethical dilemmas is one of the main disincentives to EC request physicians. 23 Given the service’s novelty, it may be reasonable to expect physicians not to identify the circumstance in which the CEC can be helpful. Moreover, the ability to identify ethical problems is not a straightforward matter. Consequently, CEC should assume a proactive approach in making its help available to physicians, especially those with less training on ethics. 7
CEC and public health: Potential support and underdeveloped activities
Considering the third function, ethical policy development, it is interesting to note that all the documents developed by the CEC dealt with Covid-19 ethical issues. It confirms the potential support from CESSs in such complex circumstances and the need to provide HPs with further helps to deal with a different aspect of care and health.12–14
Finally, it must be noted that supporting the healthcare team in emergencies and the proposal of public initiatives to develop ethical awareness among citizenship, which were included in the CEC’s Regulation, have been pretty underdeveloped. As noted by Magelssen, CECs are indeed more and more required to overcome the standard threefold set mentioned, attempting different working methods—tailored seminars for particular departments, wards, or professional groups; leading ethics reflection groups in clinical wards; inviting wards to submit a case to CEC and participate in deliberation; dealing with organizational and ethics; and bringing ethical perspectives to other stakeholders in the organization or health services. 36
Conclusion
The study results can inform the ongoing debate around the CEC’s implementation, both at the national and international level.
Further studies are required to understand profession-specific barriers and benefits perceived by different HPs toward EC and CEC. Considered the nurses’ deontological call to deal with ethical dilemma, two actions can be implemented within and outside the CEC.
First of all, emphasizing the nurses’ perspectives within the CEC and during the CEC’s meetings will please help a more equal representation of different professionals in the service, and help HPs to improve the relational decision-making process among colleagues. 38 As we noted in our last consultation, including nurses’ voice in EC is pivotal to be aware of the moral distress perceived by the whole care team, not only by physicians. Moreover, considered the nurses’ high participation to the CEC’s training, an ongoing education and outreach to nurses regarding CEC functions and availability should be considered, to increase awareness and recognition of the support available and ease nurse’s access to the service. 32
Moreover, a particular attention should be provided to the CEC’s support for the community services, which will be more and more frequently challenged by ethical situations, due to aging population and the increasing incidence of chronic diseases. Due to fact that, generally, most resources are based in hospitals, community nurses may have little or no access to CDEC or ethicists, and are consequently exposed to a higher risk to develop moral distress and unresolved conflict. It may result in negative ramifications for nurses, for organizations, and for patients. Implement ethics reflection groups in community healthcare agencies should be promoted to ease the community-based healthcare professionals to CEC and EC, especially when community service are part of a larger healthcare organization that includes hospital(s) settings. 39
In conclusion, we expect that our findings may help refine the boundaries and areas of integration between the BU and the CEC and can provide meaningful insight on their impact in clinical practice for both HPs and quality of care in terms of EC’s utility and effectiveness.
Limitation
The two significant limitations of this study are the limited time of data collection and the experimental nature of the CEC. Even if the second one could be considered a strength, the data collected remain partial.
Footnotes
Acknowledgments
We are grateful to all the CEC’s members who dedicate their time to this service. Their collaboration has been invaluable, as is their commitment to bringing ethics to the patient’s bedside. This study was partially supported by Italian Ministry of Health – Ricerca Corrente Annual Program 2024.
Author contributions
MP elaborated and wrote the first draft of the paper; LdP revised the first and subsequent drafts; all authors have endorsed the final version of the manuscript. The authors contributed equally to the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.