
Abstract
Background
Physical restraints are routinely employed to ensure patient safety in Japanese acute care. Little is known about nursing students' perspectives and how they begin to question their value and knowledge in the face of restraint experiences in clinical practice.
Objective
To investigate nursing students’ questions about patient restraints and how they understand the ethics of the use of restraints in nursing.
Research design
Qualitative descriptive research using narrative analysis.
Participants and research context
Experiential data were generated and thematically analyzed from semi-structured interviews with 16 nursing students who had completed their bachelor’s degree program requirements.
Ethical considerations
The study was approved by academic and clinical ethics agencies. Participants provided written informed consent.
Results
Physical restraints were encountered in 16 incidents, 3 with children and 13 with older patients with dementia. Students struggled to comprehend the policies and protocols of restraint use and worried their use was primarily for security rather than therapeutic purposes. Five themes were identified: (1). Questioning the tension between person-centered care, patient autonomy, and restraints, (2). Questioning the nature of restraints in which participants analyzed the policies and protocols around restraint use, (3). Questioning the professional nursing self whereby students reflected on how restraint use challenged their nursing values, and (4). Questioning professional nursing practice, in which students explored how restraints fit within a nursing perspective and positioned themselves as patient advocates. Students encountering physical restraints should ask questions based on values of patient-centeredness, autonomy, and advocacy. There is a need for education that facilitates reflection and questioning so that it informs students’ ethical thinking which may enhance nurse advocacy to reduce restraint use.
Conclusions
Restraints provide contexts in which students must face tensions between nursing values and clinical reality. Further research on nursing education strategies within non-psychiatric settings is needed to reduce physical restraints.
Introduction
Nurses encounter ethical issues daily; 1 they use moral reasoning and critical thinking based on the principles of ethical sensitivity 2 to deal with varied ethical dilemmas.3,4
Physical restraint involves significant ethical dimensions which must be considered to uphold nursing values of person-centered care, patient-informed consent, and autonomy for patient and staff safety. 5 Despite substantial research on the ethics of physical restraints, there is a paucity of research on teaching about, or understanding nursing practice in the context of non-psychiatric use of physical restraints in nursing curricula. 6 Guiding nursing students through learning facts, skills, and theoretical or idealistic values to the practical clinical reality by employing critical thinking and questioning their practice and healthcare contexts, are fundamental competencies of professional nurses, essential for improving the quality of nursing practice and patient care outcomes. 7
This research involved the ethical questions students ask when they first encounter patients being restrained and how they make sense of the ethics behind restraint use in nursing. Understanding and clarifying these questions and their concepts/theorizing will help build evidence for more specific nursing education interventions.
Background
Physical restraints are used in acute care wards and emergency rooms, including pediatrics and psychiatry. Restraints use has increased with a rise in the number of elderly patients and dementia cases due to the COVID epidemic.8,9 Examples of common restraints include physical restrictions, such as bed rails, bed straps, chair belts, and wheelchair rests; social restrictions, such as visiting hours and social activity restrictions; and pharmacological restrictions, such as psychotropic medication use.10,11 Restraining children can be part of pediatric nurses’ routines when required for medical tasks such as immunizations or blood draws. 11
Physical restraints are an effective teaching tool to see support students questioning their nursing values and supporting the development of their clinical reasoning. Physical restraints are typically employed without patient consent and are a clear violation of professional ethical values, such as patient-centered care, autonomy, 12 and advocacy. Many factors that necessitate restraints are embedded in care routines and institutionalization of care processes, being considered routine procedures. 13 Modifiable predictors of restraint use include a negative work environment with poor nurse–physician relationships and uncertain and short registered nurse work hours per patient day. 14 Culture, irrespective of the mindset, normalizes the use of restraints.
In Japan, a national cross-sectional survey of acute care hospitals under the public healthcare insurance program found a point prevalence of 44.5% for physical restraints (n = 10,480). Physical restraints for patients with dementia remain common. 15
Cognitive dissonance occurs when students who have learned about nursing ideals are confronted with clinical realities in which their current practice may not reflect the best practices 16 as students typically have idealistic nursing and ethical values. 6 Thus, how are we to understand and support students who begin to question the difference between what they have learned about person-centered ethical care and legitimate means of enforcement based on patient safety?
One of the challenges in ethics education is students’ insufficient knowledge or clinical experience regarding this topic. 17 Ignoring ethical dimensions of physical restraint has far-reaching consequences, ranging from emotional distress to nurse turnover. Therefore, identifying students’ questions unaffected by organizational culture and routines could be the basis for nursing education interventions.
Objective
This study aimed to investigate nursing students’ questions regarding patient restraints in their clinical practice experiences and how they understand the ethics behind using restraints in nursing.
Research methodology
We used a qualitative narrative approach, wherein narratives were the object of investigation 18 and within which we identified critical thinking questioning processes. Storytelling reflects the understanding of human experiences and is an inherent aspect of social relationships. The importance of narratives18–20 within nursing presented an open opportunity for participants to express their experiences openly.18,21,22
Sixteen undergraduate, pre-graduation nursing students from one Japanese institution were recruited through purposeful sampling via email invitation. Inclusion criteria included being current fourth-year students who had completed program requirements and had written the national licensing exams but had not yet convocated. In Japan, they are designated “students” until they have officially graduated. Each participant encountered physical restraints in their clinical experiences. The university study site was different to the researcher’s place of employment.
Semi-structured interview data generation occurred concurrently with data analysis; considering the prevalence of COVID-19 at that time, a one-hour recorded virtual interview was conducted on ZOOM©. Following informed consent, open-ended questions were designed to elicit in-depth information about participants’ experiences and ethical questions.22,23 The main domains of questions were: • experiences with physical restraints. • emotional and cognitive responses to the use of restraints. • thinking processes involved in determining whether restraints are required, effective, or avoidable. • perceived impact on the patient and family. • questions or concerns about using restraints and how and whom they approached to answer those questions. • impact of restraint use on personal and shared nursing values and practices.
The interviewer did not interrupt the participant but continued to listen until they finished their narratives and then verified the content. Interviews were transcribed verbatim. We analyzed data using Riessman’s thematic narrative approach. 24 A first-person “I” narrative was employed to recover the ethical narratives described by study participants. Themes were extracted from the perspective of “what was being said” in the nursing students’ questions about physical restraints while maintaining each participant’s story. The themes were typified according to their characteristics and the types of questions.
To support the validity and probability of the narrative method, 24 study participants were provided the interview guide. Overall, the participants’ statements were consistent and reached optimum research quality or reliability for narrative analysis in this study. Frequent discussions with mentors, supervisors, and a team of research experts in nursing ethics and bioethics monitored bias, resolved differences in interpretation, and facilitated reflection, interpretation, and verification of analysis. 24
Ethical considerations
The research protocol was reviewed and approved by the researcher’s academic ethics review committee and ethics review body at the study site (No. 20-A079). The interviewer was not employed at the study site and did know the students. Participants provided written informed consent before the interview. All data were de-identified and kept confidential.
Results
Fifteen women and one male undergraduate nursing student participated in this study. All were recent graduates who had completed their Bachelor of Nursing program in February 2021, were due to graduate in March, and planned to start working as nurses in a health institution in April 2021. The average age was 23 years (SD: 22-39). One participant had a non-nursing degree. All of them encountered physical restraints in their clinical practice and wished to participate in the study voluntarily. Their interview time was approximately 1 h.
The restraint scenarios shared by the students are listed below: Thirteen cases involved older patients with dementia who were already restrained when the students encountered them. In three other instances, pediatric patients were restrained while the students were monitoring them, and in one case, a young psychiatric patient was in an isolation room. In 11 of these situations, the student was the nurse in charge, and all cases were supervised by a registered nurse and a faculty instructor. All cases occurred in the second half of the student’s third and fourth years when they were assigned to acute care inpatient.
Inhibitions and questions encountered by participants, and ethical questions and concepts.
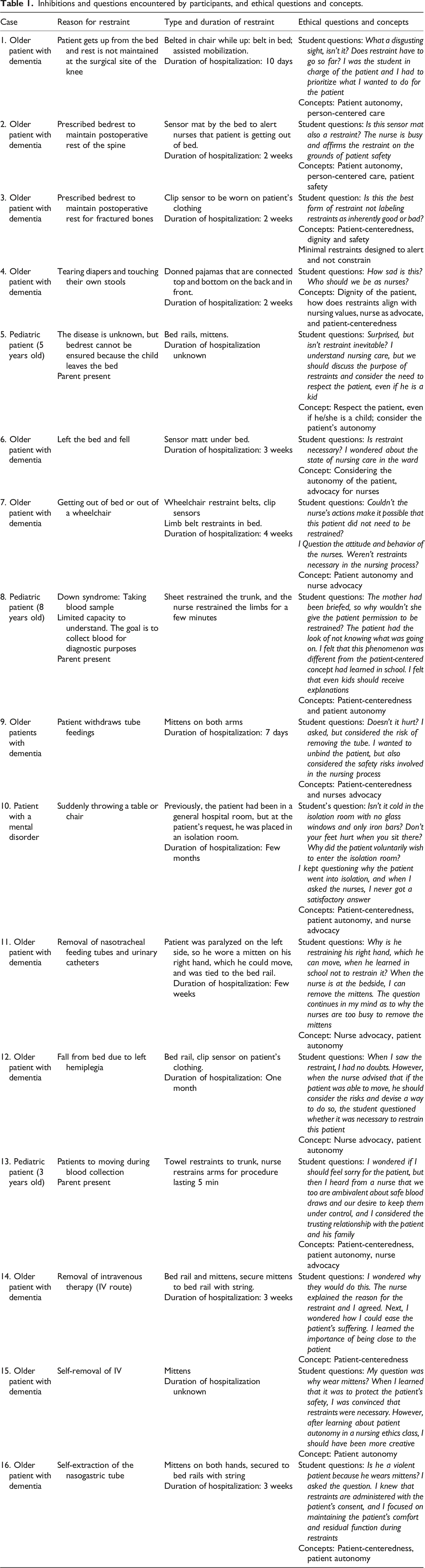
Central to all narratives were concepts of person-centered care, patient-informed consent, and autonomy and dignity, as one student expressed: “I believe that a patient’s actions have meaning. Patients move because they are suffering from phlegm entanglement or itching. The nurse should focus on the needs of that patient. If they do so, restraints may be reduced”.(I11) Issues of maintaining patient autonomy in action were balanced with the risk of safety, given the available resources in the nursing unit; “I believe restraints protect the patient. The nurses on this unit are busy. I think restraints are unavoidable because they are understaffed as I see it”. (I2)
Theme 1: Questioning the tension between person-centered care, patient autonomy, and restraints
Participants’ first concerns focused on the patient in front of them. They expressed concern for the patient in terms of their experience and discomfort and about how their autonomy and ability to provide informed consent was addressed or preserved when staff chose and applied the restraints. Most restraint scenarios described by participants were situations in which patient consent could not be directly obtained. Perceiving this lack of autonomy led to students changing their perspectives and wonder about the patient experience. Students were sensitive to nonverbal communication of distress, “I thought the patient looked distressed and uncomfortable while wearing the mittens” (P14) and “He looked sad as if he had given up resisting” (P7). Obvious manifestations of distress led to participants wondering about more tacit expressions, with one participant noting, “I wondered if patients instinctively dislike being restrained when they remove their clothes even when they are unconscious” (P14).
Participants questioned family involvement and reactions in the decisions to use physical restraints. In all pediatric situations, parents were present and involved. The nurse talked about the restraints only to the parents who understood and actively cooperated but not to the child. There were no family members or designated decision makers with the other patients who were all older and lived with either dementia or a mental health condition. Even when the patient appeared to be settled and the family was okay, students wondered if there were covert feelings regarding the restraint and patient: “Even if the family of the patient who is restrained right now was feeling okay, I was wondering in my mind how the family was feeling” (P16).
From this person-centered perspective, students then questioned how decisions to restrain were made, and if the choice to apply restraints was appropriate in that situation. For example, one participant described the reasons for using restraints on a wandering patient: “From what I saw, it was hard to imagine, for example, that he would walk away because he needed to go to the bathroom, but I wondered if the restraint was necessary for this person” (P3). Minimal forms of restraints, such as sensors, generated a different perspective because students could recognize attempts to keep the person safe by alerting staff about their movements, but which did not actually restrain their physical autonomy.
Inappropriate application of restraints or work-around restraint garments were questioned: “I wondered what the patient thought about wearing the restraint garment backward” (P4).
Students engaged in ethical clinical reasoning by focusing on the individual involved, wondering about their experience, discomfort, and level of informed consent. They quickly noticed that the most minimal forms of restraint could facilitate some autonomy in movement but they could alert staff to potential safety issues rather than preventing all or most autonomy. From this standpoint, they started to explore the nature of restraints themselves.
Theme 2: Question for the nature of restraints
Students expressed shock and surprise when encountering restraint. They needed to shift their thinking from social norms that assumed only criminals are restrained to an underexplored approach to nursing clinical reasoning that may not have the person as its central concern. Some participants were already aware of the questions to ask regarding restraint, safety, and patient autonomy before their clinical encounters. One participant commented, “Before I went to the [adult med-Surg clinical setting], I wondered where the line was between safety and restraint. When I went to the [setting], I saw many healthcare workers putting restraints on patients while holding them down and wondered if this was what restraint involved” (P6). Once they saw the restraints in action, students asked broader questions about the nature and methods of patient restraint. They began to compare their person-centered nursing values with concepts of safety, patient freedom, and autonomy, including clinical reasoning in evaluating the effectiveness of restraints.
Keeping patients at the center of the nursing gaze was now considered in the context of the realities of the staffing situation and whether a nursing presence could be safely maintained without restraints; they asked if restraints were the only way to keep both patients and staff safe. Notably, participants frequently asked instructors and staff but did not always get answers that satisfied their concerns about nursing values and actions. For example, students asked, “How can we be with the person without restraints?” (P1). Over time, frustration could build as they struggled to find answers, as one student noted, “How can we use restraints to safely treat the patient, that question has not been answered” (P7).
Student participants acknowledged that restraint use criteria necessarily considered the appropriate level of restraint for patients of different settings. Some students questioned restraints as an abstract concept that can be seen in other socially accepted situations, such as child car seats. One student said, “We had a class on the legal interpretation of restraints before I went to clinical practice, and I asked why it was okay for children (to use car seats and other restraints) but not okay for adults (to wear mittens and other restraints) to be safe, but I never got a clear answer” (P6).
Despite policy and procedure manuals available on units, these participants relied more on their classroom learning and found it difficult to integrate this with formal organizational policies observed in practice. Students struggled to understand procedures for releasing restraints and questioned how to safely release them; one student stated: “I still have questions about how to get involved and how to safely perform the procedure” (P7).
In sum, these participants first focused on their patients and then attempted to understand how and why a physical restraint was necessary and appropriate in that context. Many needed to integrate their general social knowledge that criminalized or disempowered individuals being restrained and those forms that are entirely socially legitimate. Unfortunately, most clinical nursing decision-making was not overtly reflective of institutional policies and procedures, which made the balancing of risk and benefit exceptionally challenging for these novice practitioners. Simultaneously, participants reflected on their own nursing values and the implications that these ethical tensions had on their sense of professional self.
Theme 3: Questions for the professional nursing self
Students quickly started to question themselves in terms of how they should perceive, manage, and act in patient restraint situations. Students encountered feelings of fear or dislike of restraints or restrained patients; in questioning their actions, participants’ focus moved from the patient to their role in the situation, as one of them stated, “The first thing I felt was, what should I do? What should I do that day” (P10).
Participants were acutely aware of their negative feelings regarding restraint use, which engendered critical questions about the ethics of removing a patient’s autonomy and choice. Common reactions to seeing restraints included dislike and emotional distress: “When I first saw the restraint, I had a big feeling that my heart was in pain” (P9); fear, “The patient shouted and slammed the inside of the door. When I saw that, I felt scared” (P5); and surprise “I am surprised to see the patient wearing mittens” (P15). Students whose first response was negative started to question whether they needed such extensive interventions, as one participant mentioned, “I thought I did not like the restraint. I wondered if I had to go this far” (P1).
Once students witnessed restraints, they reflected on their future decisions and actions. One participant said, “I am not looking forward to seeing the future, but I am wondering what I will think when I see restraints in the future” (P15). Participants wondered about alternative outcomes if they had to make these decisions, “I have always wondered what I should do if I oversaw this case” (P14).
Students recounted narratives in which they engaged in value-based clinical reasoning about how they would act as nurses in the future. “After the clinical training, I became interested in restraints and began to study the laws and guidelines. My studies continue to this day. I believe it will help me to consider the need for restraints when I become a nurse” (P10).
Participants reflected on the ethics of restraints beyond the immediate situation. Often, these questions were intended for other students and comprised a narrative about what they thought of restraints as a clinical intervention practice. A common strategy was to imagine themselves in the patient’s place: “I wondered what people think about physical restraint. I wanted to ask it. I had asked the [student] once at that time when we were eating lunch, what everyone would think if they were put in an isolation room” (P10). Participants used storytelling to communicate the situation and discuss ethical dilemmas with peers. The challenges they experienced in navigating their own ethical position in relation to restraints were offered to fellow students as a way to prepare and educate them prior to their own encounters with restraints.
Theme 4: Questioning professional nursing practice
Nursing students watched and thought about the actions and behaviors of nurses during clinical experiences. They questioned why the nurses determined that restraints were the best option for their patients and if the restraint’s application was optimal. Some students perceived that patients were not actively involved in decision-making and asked, “Why do nurses not ask the patient for permission to use physical restraints? I heard information that the patient had come to the outpatient clinic and was restrained several times, but that made me wonder why they did not tell the patient that they were going to restrain him” (P10).
Many student participants observed that physical restraints were used to reduce staff obligations to observe and monitor the patient directly or indirectly. Nurses were open in acknowledging physical restraints were frequently used with wandering patients simply due to a lack of staff to directly observe and monitor. One participant asked if it was possible to reduce the amount of time patients are restrained: “I thought maybe we could take off the mittens and play catch with origami or balloons, for example” (P15).
Theme 5: Positioning the self as a patient advocate
Synthesizing their formal and experiential knowledge about nursing practice and restraints generally led participants to reflect on their stance on being patient advocates. One student shared how seeing the physical restraints inspired her to consider doing something to advocate for her patients: “I thought restraints were a last resort. I worked hard to support this patient’s comfort. We removed the mittens, gave him a hand bath, and performed simple rehabilitation to take the contractures out of his hands. The patient seemed happy, and I thought, “This is nursing” (P16). Another participant spoke about becoming aware of the patient’s needs and considering the nursing advocacy role. “The patient’s lips were dry, her skin was cracked and sore. I could see that she did not want oral care and was physically active. Why did the nurse not notice that? I think it is inconsistent with the role of nursing to restrain her hands and feet” (P11). Other narratives involved confusion about what their role could or should be as a student. One participant stated, “I felt my perspective was limited because of my lack of knowledge...I am a student...I am not a nurse. I am a student, so I cannot do anything. I considered it difficult to remove this patient’s mittens” (P15). Subsequently, there were narratives from students who struggled with cognitive dissonance but did not feel they had the right or permission to speak as students: “This patient left the bed alone and a sensor mat was on the bed. I was terribly disappointed in the actions of the nurse who put it up. But I couldn’t say anything because I am a student” (P12).
These narratives suggested a normative attitude of powerlessness and voicelessness as a student, recognizing one’s own lack of knowledge, and still finding ways to realize the role of nurses situation.
Discussion
Nurses focus on the patient and their environment. Person-centered care, patient autonomy, and consent are key values in nursing practice. 6 When students encounter physical restraints used in clinical settings, it forces them to reflect on the gap between their theoretical nursing knowledge and the practical clinical reality. It is notable that students, as we want nurses to do, started questioning restraint practices by focusing on the patient.
Research indicates Japanese nursing students view the restriction of freedom due to being restrained as an ethical issue, not the restraint itself. 25 Our results suggest that the main question was not about physical restraints but about the patient. This implies that when encountering physical restraints, nursing students pay more attention to the patient than to the restraints, and focus on the reasons for restraints and their discomfort: “Why is the patient being restrained?” and “Is the patient in pain because of the restraint?” These are patient-centered care questions. In other research, healthcare staff find coercive interventions more acceptable, perhaps to legitimize their actions. 26 The present study’s results indicate that nursing students who encounter physical restraints focus their holistic gaze on the experience of the physically restrained patient as context before identifying the ethical issues. Tronto 27 argues that sympathizing with a person without acting does not constitute care. The initial questions raised by nursing students were about the patient; this was not sympathy, but rather a step in demonstrating their concern for patient-centered care. Helping students learn compassionate caring consists of five interlinking processes: attentiveness, responsibility, competence, responsiveness, and solidarity. 27 Attentiveness is the starting point of care, placing emphasis on the recipient of care and identifying their physical and mental needs. Without this process, appropriate care cannot occur. 27 This is what the nursing students were engaged in: paying attention to the person and assessing their needs through the nurse’s perspective. 28 Since the perspectives of a nursing student are not like those of an established nurse, Tronto’s concern for the recipient of care and nursing student’s questioning of the patient are not quite synonymous. 27 However, this questioning represents a gateway to learning the five processes; therefore, supporting, facilitating, and encouraging early questions are essential to promote ethical nursing practices that are grounded in real clinical practice. Specific interventions suggested as strategies for support include daily debriefings, journal reflections, in-school role plays, and simulations.
We also consider these five processes of nursing to be adaptable to educational interventions for restraint use. Renewed discussion among nurses about patient-centered care and autonomy would be a useful educational intervention to encourage clinicians to consider alternatives to physical restraints.
The student participants understood restraint as a clinical intervention and asked questions not only about the situation in front of them, but also about criteria for decision-making regarding restraint use, its release, and its ethics of it from various perspectives. Policies regarding restraints use should identify the types of approved restraints (e.g., mittens and belts), and establish clear ethical procedures to ensure patient safety while respecting human rights (e.g., autonomy and consent). The fact that questions were raised about the value of restraints and how values, policies, and procedures differed depending on whether the patient is a child or an adult, indicates that students test their core theoretical knowledge in different clinical contexts. The questions that trigger patient-centered care, autonomy, and advocacy are often derived from the knowledge and skills acquired in classroom exercises, which supports students in their own theoretical, organizational, and professional ethical perspectives. Scenarios involving physical restraints in psychiatric and non-psychiatric settings should be employed in classroom experiences as exemplars of situations in which the patient’s preferences and wishes are frequently dissonant with those of the healthcare team thus raising critical questions: For whose benefit is the restraint used and how are the risks and benefits weighed?
Patient-centered care, autonomy, advocacy value, and competency development include an iterative process utilizing both theoretical and experiential learning through all years of a nursing program. Thus, it is imperative that nurse educators be prepared to initiate or engage in discussions about the ethics of restraint use whenever students raise questions that might not initially appear to be ethics related; questioning about patient experiences and human rights, the nature of restraints, and their own and other healthcare team members roles and responsibilities are clues that a “teachable” moment is at hand. 29 Restraint use is associated with significant social determinants of health such as race, ethnicity, age, economic status, presence of health insurance, and homelessness. 30 It is an excellent vehicle to support students in applying ethical thinking in different contexts, and to transition from theory to clinical reality, including the impact organizational culture has on nurses’ decision-making and actions. 31
Nursing students noticed and questioned their own emotions toward physical restraints; these were invariably negative, such as dislike, fear, and surprise. The feeling is an “evaluative response situated among the various information processing processes.” 32 In general, feelings include a predominant physical sensation. 33 This emotional reaction precedes ethical reasoning and the determination of whether restraints were right or wrong, which is supported by previous research. 16 However, the influence of emotions during clinical simulations 34 is significant, as are the positive effects of peer-led debriefing on learners’ cognitive and psychomotor domains. 35 Nursing programs are increasingly including exposure and practice in addressing violence in clinical settings, 36 but there is no literature on the emotional effects nursing students experience during their practice with patients who are physically restrained. The scarce existing literature is limited to emotions and emotional labor when providing care. 37 It is well established that nurses, among other health care professionals, mitigate negative emotions such as guilt about restraints with explanations that patient and staff safety takes precedence. 38 Classroom or simulation-based exposure prior to clinical experiences is essential to ensure that students can be supported through their emotional reactions to engage more deeply in their ethical thinking.
The restraint-free model of care requires a holistic approach to safety, involving all team and family members. 39 Nurses need to put the patient at the center of their care and consider their role in protecting the safety and autonomy of that patient, including their choice of physical restraints, which means enhancing the nurses’ advocacy role. 40 Japanese nursing institutions need to prioritize legitimate roles in advocating for their patients, which is not apparent from these findings. Nurses’ responses to managing a patient being restrained have been described as a lack of emotion a concept known as nurse’s helplessness. 39 Further analysis of the tensions between advocacy and normalized nursing roles in restraint decision-making can help improve the quality of nursing care, including the development of educational theory, management theory, and design of instruments to assess nurses’ performance 41 and to develop means to reduce physical restraints in clinical practice.
Limitations
This study is that the results should be applied with caution beyond the Japanese context as the nursing profession and roles may vary across cultures and societies although nursing values around patient-centered care and autonomy are espoused as universal. This study recruited students who were eager to recount their experiences, so it is likely there are untapped perspectives. Future studies need to examine student reasoning in the context of physical restraints across nursing programs, cultures, and health settings.
Conclusion
Encountering physical restraints is a crucial learning point for nursing students. Restraints pose ethical tensions between their learned values of patient-centered care, autonomy, and advocacy, and the nursing clinical reality characterized by staff shortages and workarounds to keep patients safe while minimizing nursing work. Nursing students look to instructors and unit nurses to understand the ethics and practical implications of applying restraints and failure to see strong role modeling in decision-making behaviors complicates their ability to reconcile their theoretical knowledge and values with their practical experience. Nursing education needs to examine ways to connect these restraint questions to ethical domains of clinical reasoning and decision-making. The results of this study point to an urgent need to highlight non-psychiatric restraint use in nursing education and to further improve nurses’ advocacy roles to reduce the use of physical restraints.
Footnotes
Acknowledgments
We would like to sincerely thank all the nursing students for their support in conducting this study. We would also like to thank Dr. Mari Tsuruwaka for her guidance and Dr. Jude Spiers for her advice.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI [grant no. JP17K12127].
Ethics
The research protocol was reviewed and approved by the researcher’s academic ethics review committee and the ethics review body at the study site (No. 20-A079).